You might also like
- Apollo KH Hospital: Nursing ManualDocument8 pagesApollo KH Hospital: Nursing ManualSheela Solomon100% (3)
- GNSS Signal StructuresDocument45 pagesGNSS Signal StructuresVasikaran PrabaharanNo ratings yet
- Drug Therapy MonitoringDocument48 pagesDrug Therapy MonitoringPooja agarwalNo ratings yet
- Survival GuideDocument4 pagesSurvival Guideeclipse1130No ratings yet
- 1MA207 1e Radar and Component TestDocument23 pages1MA207 1e Radar and Component TestVasikaran PrabaharanNo ratings yet
- Systems Thinking in The Healthcare Professions - A Guide For EducaDocument117 pagesSystems Thinking in The Healthcare Professions - A Guide For EducaMariana EloiNo ratings yet
- Case Quality Management - Mayra SalirrosasDocument2 pagesCase Quality Management - Mayra Salirrosasmayra salirrosas100% (1)
- Assignment ON Documentation: Submitted To: Submitted byDocument12 pagesAssignment ON Documentation: Submitted To: Submitted byNagulan Nagul100% (1)
- Behind the Dental Chair: How Smart Dentists Crack the Code and Build a Dream PracticeFrom EverandBehind the Dental Chair: How Smart Dentists Crack the Code and Build a Dream PracticeRating: 5 out of 5 stars5/5 (2)
- Anecdotal RecordsDocument21 pagesAnecdotal RecordsShubhrima Khan100% (1)
- Anthem® Blue Cross Your Plan: Snap, Inc: Custom Classic PPO 500/20/20 Your Network: Prudent Buyer PPODocument9 pagesAnthem® Blue Cross Your Plan: Snap, Inc: Custom Classic PPO 500/20/20 Your Network: Prudent Buyer PPOSamson FungNo ratings yet
- Bronze HSA 5000Document4 pagesBronze HSA 5000Vasikaran PrabaharanNo ratings yet
- 2021 BAAG - Technologies - TalentDocument2 pages2021 BAAG - Technologies - TalentDalt RaNo ratings yet
- Schedule of BenefitsDocument7 pagesSchedule of BenefitsMaddy CruzNo ratings yet
- Blueoptimum Plus Ppo Plan: Benefit SummaryDocument4 pagesBlueoptimum Plus Ppo Plan: Benefit Summarylooksmart111No ratings yet
- Materials Testing and Consulting Inc 2024 Classic 1000 BsDocument5 pagesMaterials Testing and Consulting Inc 2024 Classic 1000 Bsapi-307235383No ratings yet
- What You Pay in The PPO PlanDocument2 pagesWhat You Pay in The PPO Plannathan wongNo ratings yet
- 2023 Talent BAAGDocument3 pages2023 Talent BAAGThi HanNo ratings yet
- 2021 GemPlan Summary of BenefitsDocument53 pages2021 GemPlan Summary of BenefitsRaja Churchill DassNo ratings yet
- 2023 FMCNA Medical Plan Cost ComparisonDocument2 pages2023 FMCNA Medical Plan Cost ComparisonCristal PeoplesNo ratings yet
- Benefits DocumentDocument11 pagesBenefits DocumentAndrew VlackNo ratings yet
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Document6 pagesKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisNo ratings yet
- Aetna Open Choice Ppo: Plan DetailsDocument2 pagesAetna Open Choice Ppo: Plan DetailsSnake Diet RyanNo ratings yet
- 2019 Plan BenefitsDocument14 pages2019 Plan BenefitsMichelleJeungNo ratings yet
- Aetna California Managed Choice Open Access 1750 CA 2011Document1 pageAetna California Managed Choice Open Access 1750 CA 2011Dennis AlexanderNo ratings yet
- Trinity Health 020 Traditional Ppo Plan 10202021Document10 pagesTrinity Health 020 Traditional Ppo Plan 10202021emily WNo ratings yet
- Aetna California Preventative and Hospital Care 3000 2011Document1 pageAetna California Preventative and Hospital Care 3000 2011Dennis AlexanderNo ratings yet
- Cardea Schedule of Benefits Effective Jan 1st 2021Document4 pagesCardea Schedule of Benefits Effective Jan 1st 2021Wayne GajadharNo ratings yet
- WWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersRohitKumarNo ratings yet
- 2022 Steven Charles BAG - CODocument4 pages2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNo ratings yet
- 2022-2023 FCPS - Anthem KeyCare 25 SBCDocument13 pages2022-2023 FCPS - Anthem KeyCare 25 SBCRichardRobbinsNo ratings yet
- Photon Benefits 2022 (August)Document7 pagesPhoton Benefits 2022 (August)sojithesouljaNo ratings yet
- USS Pre-Medicare PPO With RX PlanDocument3 pagesUSS Pre-Medicare PPO With RX PlanAnonymous w0egAgMouGNo ratings yet
- 76962CT0010006-01 en USDocument98 pages76962CT0010006-01 en USKathy ApergisNo ratings yet
- 2010 UnitedHealthcare Benefits SummaryDocument1 page2010 UnitedHealthcare Benefits Summaryapi-27017317No ratings yet
- 2023 Open Enrollment Benefit Presenation - 11142022Document30 pages2023 Open Enrollment Benefit Presenation - 11142022margreen5No ratings yet
- MVP Health InsuranceDocument2 pagesMVP Health InsurancePSC RFQNo ratings yet
- Us Apple Plus Ppo Feb2019 en 1Document3 pagesUs Apple Plus Ppo Feb2019 en 1Lucas Coleta AlmeidaNo ratings yet
- BCBS Enrollment GuideDocument6 pagesBCBS Enrollment GuideAnonymous Lri40PrlkNo ratings yet
- United Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405Document8 pagesUnited Healthcare CA Select Plus Silver 30 2000 30 Aksa W 405zxcvNo ratings yet
- Summary of Benefits: Silver Trio Hmo 2300/70 OffexDocument12 pagesSummary of Benefits: Silver Trio Hmo 2300/70 OffexjaroopaitummaiNo ratings yet
- Summary of Benefits: Bronze Trio Hmo 7000/70 OffexDocument12 pagesSummary of Benefits: Bronze Trio Hmo 7000/70 OffexjaroopaitummaiNo ratings yet
- EmblemHealth Benefits 2019Document7 pagesEmblemHealth Benefits 2019Jorge Luis Rivera AgostoNo ratings yet
- Vanderbilt phf-21-22Document2 pagesVanderbilt phf-21-22api-458468763No ratings yet
- Anthem Silver Preferred Blue PPO 3000 20 7250 W HSA NH PPO Small 6UPP 01 01 2023 English SBC CYDocument12 pagesAnthem Silver Preferred Blue PPO 3000 20 7250 W HSA NH PPO Small 6UPP 01 01 2023 English SBC CYsantiagomNo ratings yet
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Document3 pagesBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherNo ratings yet
- Aurora - Baseline Option 2019 SOBIDocument4 pagesAurora - Baseline Option 2019 SOBISean MurrayNo ratings yet
- Summary of 2022 Benefit Changes: MedicalDocument5 pagesSummary of 2022 Benefit Changes: MedicalChinnu SalimathNo ratings yet
- Aetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425Document23 pagesAetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425kevin.mccreaNo ratings yet
- First Help PlanDocument1 pageFirst Help PlanIvan QuevedoNo ratings yet
- 2010 UHC Medical Plan ComparisonDocument2 pages2010 UHC Medical Plan Comparisonapi-20618861No ratings yet
- Keystone HMO Bronze Essential 750070140700Document11 pagesKeystone HMO Bronze Essential 750070140700ANKIT SINGHNo ratings yet
- Plan Comparison Chart Seniorcare Hip AetnaDocument5 pagesPlan Comparison Chart Seniorcare Hip AetnaRamonita GarciaNo ratings yet
- SBC Test PDF FileDocument10 pagesSBC Test PDF FileAyaz GulNo ratings yet
- FY 2022-2023 Instruction Partners Benefits OverviewDocument16 pagesFY 2022-2023 Instruction Partners Benefits OverviewSendhil RevuluriNo ratings yet
- Kaiser Permanente Compare Plans CA 2011 KPIFDocument1 pageKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderNo ratings yet
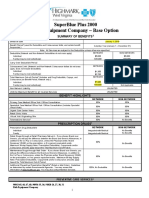
- Rish Equipment Base Plan Option Eff. 1.1.2019Document4 pagesRish Equipment Base Plan Option Eff. 1.1.2019michala anthonyNo ratings yet
- 2021 THNM Individual Health PlansDocument1 page2021 THNM Individual Health PlansSara SnowNo ratings yet
- LTIM - USA Employees Benefits Overview - 2024Document20 pagesLTIM - USA Employees Benefits Overview - 2024Ramesh Kumar KNo ratings yet
- S608CHC Blue Choice Silver PPO 024: This Is Only A SummaryDocument8 pagesS608CHC Blue Choice Silver PPO 024: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Benefits Overview 2018Document5 pagesBenefits Overview 2018Joby JoNo ratings yet
- AARP UHC 2024 Benefit Highlights LA 004P FocusDocument4 pagesAARP UHC 2024 Benefit Highlights LA 004P FocusAlaa ZaidNo ratings yet
- Keystone HMO Gold Preferred 4080650Document11 pagesKeystone HMO Gold Preferred 4080650ANKIT SINGHNo ratings yet
- Blueshield Gold Trio HMO 1500:35Document14 pagesBlueshield Gold Trio HMO 1500:35jaroopaitummaiNo ratings yet
- Important Questions Answers Why This Matters:: IndividualDocument7 pagesImportant Questions Answers Why This Matters:: Individualsashank varmaNo ratings yet
- Tufts Health Plan Spirit Benefit Summary: July 1, 2017Document6 pagesTufts Health Plan Spirit Benefit Summary: July 1, 2017MNo ratings yet
- Employee Benefits-Wellness Guide 2023-24Document30 pagesEmployee Benefits-Wellness Guide 2023-24shanzeh2609No ratings yet
- Anthem Silver PS HMO 60-2500-45 9B1J Summary 1-24Document13 pagesAnthem Silver PS HMO 60-2500-45 9B1J Summary 1-24bbspissoffNo ratings yet
- United Healthcare UHC Premier 1500 CEFP GoldDocument14 pagesUnited Healthcare UHC Premier 1500 CEFP GoldSteveNo ratings yet
- Advanced RFID MeasurementsDocument27 pagesAdvanced RFID MeasurementsVasikaran PrabaharanNo ratings yet
- Capacitor Selection For Coupling and Decoupling Applications - Passive Components BlogDocument11 pagesCapacitor Selection For Coupling and Decoupling Applications - Passive Components BlogVasikaran PrabaharanNo ratings yet
- Characterizing & Debugging EMI Issues For Wireless and IoT ProductsDocument14 pagesCharacterizing & Debugging EMI Issues For Wireless and IoT ProductsVasikaran PrabaharanNo ratings yet
- BDocument54 pagesBVasikaran PrabaharanNo ratings yet
- RF Chain - WikipediaDocument15 pagesRF Chain - WikipediaVasikaran PrabaharanNo ratings yet
- RFCafe CalculatorWorkbook v5p1Document18 pagesRFCafe CalculatorWorkbook v5p1Vasikaran PrabaharanNo ratings yet
- Qorvo Antenna Aperture Tuning EguideDocument20 pagesQorvo Antenna Aperture Tuning EguideVasikaran PrabaharanNo ratings yet
- Impedance Matching Smith Chart FundamentalsDocument18 pagesImpedance Matching Smith Chart FundamentalsVasikaran PrabaharanNo ratings yet
- Complex Analysis of The Lossy-Transmission Line Theory: A Generalized Smith ChartDocument22 pagesComplex Analysis of The Lossy-Transmission Line Theory: A Generalized Smith ChartVasikaran PrabaharanNo ratings yet
- AT&T Radiated Performance Requirements 20170504054000896Document2 pagesAT&T Radiated Performance Requirements 20170504054000896Vasikaran PrabaharanNo ratings yet
- AWR1243 Sensor: Highly Integrated 76-81-GHz Radar Front-End For Emerging ADAS ApplicationsDocument12 pagesAWR1243 Sensor: Highly Integrated 76-81-GHz Radar Front-End For Emerging ADAS ApplicationsVasikaran PrabaharanNo ratings yet
- LTEDocument26 pagesLTEVasikaran Prabaharan100% (1)
- SP17316 Smartphones RF Front-End Module Sample System Plus ConsultingDocument23 pagesSP17316 Smartphones RF Front-End Module Sample System Plus ConsultingVasikaran PrabaharanNo ratings yet
- OceanofPDF - Com A Suitable Boy 20th Anniversary Edition - Vikram Seth PDFDocument1,462 pagesOceanofPDF - Com A Suitable Boy 20th Anniversary Edition - Vikram Seth PDFDipanjana SahaNo ratings yet
- WS Retail Services Pvt. LTD.Document1 pageWS Retail Services Pvt. LTD.Vasikaran PrabaharanNo ratings yet
- IQxel TechSpecs 081915Document14 pagesIQxel TechSpecs 081915Vasikaran PrabaharanNo ratings yet
- Morning Case Report January 3, 2016Document15 pagesMorning Case Report January 3, 2016Pradnya ParamithaNo ratings yet
- Title 25 Chapter 134: Psychiatric HospDocument172 pagesTitle 25 Chapter 134: Psychiatric HosposcartxnNo ratings yet
- Pil - T16Document96 pagesPil - T16harsh jainNo ratings yet
- Pre Auth Form Revised PDFDocument5 pagesPre Auth Form Revised PDFNILESHNo ratings yet
- NURS FPX 6214 Assessment 1 Technology Needs AssessmentDocument4 pagesNURS FPX 6214 Assessment 1 Technology Needs Assessmentjoohnsmith070No ratings yet
- Sineflex Solutions: Partnering For Healthcare InnovationDocument10 pagesSineflex Solutions: Partnering For Healthcare InnovationD S Sagar Tripuramallu100% (1)
- Natasya Herliza 2211112297Document9 pagesNatasya Herliza 2211112297Natasya Herliza 2211112297No ratings yet
- Rahimah IsmailDocument1 pageRahimah Ismailnatashah designNo ratings yet
- Amber - Pavelka@go - Tarleton.edu - (254) 723-8960 - Stephenville, TX 76401Document2 pagesAmber - Pavelka@go - Tarleton.edu - (254) 723-8960 - Stephenville, TX 76401api-519803857No ratings yet
- Pengabmas Sudah Di UploadDocument5 pagesPengabmas Sudah Di UploadPutri FitriaNo ratings yet
- BS BuzzDocument8 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Acc6075 Moving Guide TechniqueDocument72 pagesAcc6075 Moving Guide TechniqueJasonJejametNo ratings yet
- Health Disparities and Health Education-1finalDocument13 pagesHealth Disparities and Health Education-1finalbrendahronoh254No ratings yet
- More For Your Health From A To Z PDFDocument20 pagesMore For Your Health From A To Z PDFmunawarnuml2913No ratings yet
- Older AdultsDocument4 pagesOlder Adultsapi-293182319No ratings yet
- Gastric GavageDocument3 pagesGastric GavageRico Delgado of WorldbexNo ratings yet
- EpicCare Link User Access Form 5-12-14Document1 pageEpicCare Link User Access Form 5-12-14KrushiNo ratings yet
- Clinical Nursing JudgementDocument6 pagesClinical Nursing Judgementapi-604539767No ratings yet
- 08 Claim FormDocument4 pages08 Claim Formanurag1309No ratings yet
- Ict LC#1Document14 pagesIct LC#1usmansafdar12535No ratings yet
- Profil Perusahaan Cynergy Care IndonesiaDocument18 pagesProfil Perusahaan Cynergy Care IndonesiaRomeo Jaka RNo ratings yet
- Defrino Relational WorkDocument19 pagesDefrino Relational WorkChimmsammy LoNo ratings yet
- Ensuring Good Dispensing PractiesDocument32 pagesEnsuring Good Dispensing PractiesTifa IstiwaNo ratings yet