You might also like
- Part 1: Deformation: Prelab: Deformation, Earthquakes, & Preparedness Prelab ReportDocument4 pagesPart 1: Deformation: Prelab: Deformation, Earthquakes, & Preparedness Prelab ReportGil GameshNo ratings yet
- Sample ChecklistDocument46 pagesSample ChecklistPrecious PatrickNo ratings yet
- Junior Crew: Worksheet PackDocument32 pagesJunior Crew: Worksheet PacklicNo ratings yet
- Pulse Rate ChecklistDocument2 pagesPulse Rate ChecklistPatrick SantosNo ratings yet
- Cast CareDocument3 pagesCast CareSheryll Joy Lopez Calayan0% (1)
- Adventures in Diving Knowledge Review Answer KeysDocument38 pagesAdventures in Diving Knowledge Review Answer Keyssergio100% (1)
- RPP MfaDocument10 pagesRPP MfaIZZAT DANAZZATNo ratings yet
- Care of Client After SurgeryDocument4 pagesCare of Client After SurgeryscauinianNo ratings yet
- Lab session 4Document6 pagesLab session 4IreneNo ratings yet
- Therapeutic Modalities 4th Edition Starkey Test BankDocument5 pagesTherapeutic Modalities 4th Edition Starkey Test Bankalidasinh1yvpci100% (22)
- BOW Knowledge Reviews All 5 ModulesDocument10 pagesBOW Knowledge Reviews All 5 Modules4lexxNo ratings yet
- Part 1: Deformation: Prelab: Deformation, Earthquakes, & Preparedness Prelab ReportDocument4 pagesPart 1: Deformation: Prelab: Deformation, Earthquakes, & Preparedness Prelab ReportGil GameshNo ratings yet
- Emergency Procedures for DiversDocument38 pagesEmergency Procedures for DiversGwenolé de KermenguyNo ratings yet
- Basic Water Rescue WorkbookDocument15 pagesBasic Water Rescue WorkbookZedy GullesNo ratings yet
- "Show" Requirements Guide For First Aid Merit Badge CounselorsDocument14 pages"Show" Requirements Guide For First Aid Merit Badge CounselorsotousanNo ratings yet
- Pandemic Tabletop Exercise Report - Nov-23-2020Document10 pagesPandemic Tabletop Exercise Report - Nov-23-2020Jonathan CambaNo ratings yet
- eRDPML InstForUseDocument116 pageseRDPML InstForUsehuangkuanlunNo ratings yet
- Emergency Assistance PlanDocument10 pagesEmergency Assistance Planmojarad mojaradNo ratings yet
- Las 2Document2 pagesLas 2Corazon ReymarNo ratings yet
- DISASTER PREPAREDNESS Answer SheetDocument4 pagesDISASTER PREPAREDNESS Answer SheetAshley RañesesNo ratings yet
- Cold Weather Medical MilitaryDocument31 pagesCold Weather Medical MilitarycmonBULLSHITNo ratings yet
- Anti Drowing SystemDocument88 pagesAnti Drowing SystemMaximilian Sylvester100% (2)
- Confined Water Refresher & Quick Review Jan 2012Document5 pagesConfined Water Refresher & Quick Review Jan 2012Paulo MendesNo ratings yet
- EN719DT Rescue Diver Knowledge Review Answer Key v101 PDFDocument18 pagesEN719DT Rescue Diver Knowledge Review Answer Key v101 PDFmax minNo ratings yet
- The Recreational Dive PlannerDocument28 pagesThe Recreational Dive PlannerRaul LaggerNo ratings yet
- Lead Registration Form and LMP OutlineDocument5 pagesLead Registration Form and LMP OutlineonaljenNo ratings yet
- 2023 Hbl Unit 1 Exam Booklet One Mcq and Sa (4)Document27 pages2023 Hbl Unit 1 Exam Booklet One Mcq and Sa (4)Ralph Rezin MooreNo ratings yet
- Code Blue ProtocolDocument2 pagesCode Blue ProtocolChirag Ballani100% (4)
- Cco For Cyanide and MercuryDocument3 pagesCco For Cyanide and MercuryMarc ChristianNo ratings yet
- Household Services Summative wk3-6Document2 pagesHousehold Services Summative wk3-6donna kristine Delgado50% (2)
- 4 Pe 12Document3 pages4 Pe 12Charlie RiveraNo ratings yet
- Jmr-7200 - 9200series (e) 7zpna4446f (7版) Instructionl (Basicoperation) 190701Document374 pagesJmr-7200 - 9200series (e) 7zpna4446f (7版) Instructionl (Basicoperation) 190701Manuel VelezNo ratings yet
- 101-RadarSea JRC JMR-7200-9200 Instruct Manual Basic 29-8-2021Document376 pages101-RadarSea JRC JMR-7200-9200 Instruct Manual Basic 29-8-2021Thar Htun San100% (1)
- All Answered "YES": Worker's Representatives Workers EmployerDocument32 pagesAll Answered "YES": Worker's Representatives Workers EmployeranNo ratings yet
- EHS 030 First Aid Procedure SampleDocument3 pagesEHS 030 First Aid Procedure SampleAshish Mali0% (1)
- 03incident Investigation ReportDocument2 pages03incident Investigation ReportKhuda BukshNo ratings yet
- CMAS One Star Diver Training ProgrammeDocument5 pagesCMAS One Star Diver Training ProgrammehadiranjbarNo ratings yet
- Binder Aiomt Test-8 Mock-8Document64 pagesBinder Aiomt Test-8 Mock-8naveen.jain28495No ratings yet
- Intercontinental Terminals Company LLC Declaration of SecurityDocument2 pagesIntercontinental Terminals Company LLC Declaration of Securityseafarerissues100% (1)
- Therapeutic Modalities 4Th Edition Starkey Test Bank Full Chapter PDFDocument26 pagesTherapeutic Modalities 4Th Edition Starkey Test Bank Full Chapter PDFphelimletitiaioxb0100% (8)
- Critical Illness Doctor's Statement FormDocument2 pagesCritical Illness Doctor's Statement FormAna AzNo ratings yet
- Warning Order Format GuideDocument6 pagesWarning Order Format GuideOc VilNo ratings yet
- Physical Therapy Amputee Assessment FormDocument4 pagesPhysical Therapy Amputee Assessment FormTopaz CompanyNo ratings yet
- General Science 2 Lab ManualDocument41 pagesGeneral Science 2 Lab ManualRod100% (1)
- JRC JMR-7200-9200 Instruct Manual Basic 1-6-2020Document372 pagesJRC JMR-7200-9200 Instruct Manual Basic 1-6-2020Nguyen Phuoc HoNo ratings yet
- eRDPML InsforUse PDFDocument116 pageseRDPML InsforUse PDFMario R. KallabNo ratings yet
- Instituto Politécnico Nacional Cenlex Ust Study Guide Advanced 1 MTDocument11 pagesInstituto Politécnico Nacional Cenlex Ust Study Guide Advanced 1 MTLazlo LozlaNo ratings yet
- Diving ProcedureDocument7 pagesDiving ProcedureSurendar KhambraNo ratings yet
- Data Privacy Quiz 30Document11 pagesData Privacy Quiz 30Angelie PantajoNo ratings yet
- Detailed Learning Plan in TLE 7 - Week 1Document3 pagesDetailed Learning Plan in TLE 7 - Week 1shine davidNo ratings yet
- Test Booklet: General Studies Paper-IDocument24 pagesTest Booklet: General Studies Paper-ItopwarpercivalNo ratings yet
- SUUNTO Solution - Alpha - Manual - ENDocument41 pagesSUUNTO Solution - Alpha - Manual - ENEUROTANK MARITIMENo ratings yet
- Adverse Drug Reaction FormDocument2 pagesAdverse Drug Reaction FormDhananjay Saini100% (1)
- 4th Quarter Exam in DRRRDocument1 page4th Quarter Exam in DRRRkimmyNo ratings yet
- School of Saint Joseph (Naguilian, Isa.) Inc. Quezon, Naguilian, IsabelaDocument3 pagesSchool of Saint Joseph (Naguilian, Isa.) Inc. Quezon, Naguilian, IsabelaYvette Marie Yaneza NicolasNo ratings yet
- Unit 8 Test B: Use of English: GrammarDocument5 pagesUnit 8 Test B: Use of English: GrammarliehokgieNo ratings yet
- Answer Sheet Q4 Mod 12Document5 pagesAnswer Sheet Q4 Mod 12Rachelle Ann VelasquezNo ratings yet
- 1.教案Nevus ExcisionDocument5 pages1.教案Nevus Excision林宜璇No ratings yet
- User Instruction Manual: Closed Circuit Rebreather, IncorporatingDocument153 pagesUser Instruction Manual: Closed Circuit Rebreather, IncorporatingFernando Cadena DuqueNo ratings yet
- D Diiv Viin N: International Technical Diving MagazineDocument5 pagesD Diiv Viin N: International Technical Diving MagazineFernando Cadena DuqueNo ratings yet
- Baby Booster Manual GuideDocument24 pagesBaby Booster Manual GuideFernando Cadena DuqueNo ratings yet
- Sherwood Valves Cylinder ValvesDocument17 pagesSherwood Valves Cylinder Valvesklr_sean100% (1)
- DANnitroxNov2000 PDFDocument202 pagesDANnitroxNov2000 PDFFernando Cadena DuqueNo ratings yet
- Jetsam Technologies Ltd. Classic KISS ManualDocument48 pagesJetsam Technologies Ltd. Classic KISS ManualFernando Cadena DuqueNo ratings yet
- Diving Medicine For Scuba DiversDocument371 pagesDiving Medicine For Scuba Diversboca19660% (1)
- Aware Our WorldDocument115 pagesAware Our WorldArtin ZamanNo ratings yet
- E02 First Aid HB PDFDocument78 pagesE02 First Aid HB PDFRubenSolisNo ratings yet
- HSE - Differential Pressure PDFDocument118 pagesHSE - Differential Pressure PDFcivl g100% (1)
- Safe diving practices manualDocument201 pagesSafe diving practices manualNicolas RassoulovNo ratings yet
- Maersk Tender Fatal Diving Accident On 24 July 2 0 1 0Document52 pagesMaersk Tender Fatal Diving Accident On 24 July 2 0 1 0Fernando Cadena DuqueNo ratings yet
- Technical Maintenance Manual: Atx 200 First StageDocument18 pagesTechnical Maintenance Manual: Atx 200 First StageFernando Cadena DuqueNo ratings yet
- Investigacion de Escena Del CrimenDocument60 pagesInvestigacion de Escena Del CrimenCruz VerdeNo ratings yet
- Iso 24801 2 2014 en PDFDocument8 pagesIso 24801 2 2014 en PDFFernando Cadena DuqueNo ratings yet
- How Science Helps Navy Divers Stay SafeDocument35 pagesHow Science Helps Navy Divers Stay SafeFernando Cadena DuqueNo ratings yet
- CGTTP 3-72 4 Diving Casualty Investigation PDFDocument183 pagesCGTTP 3-72 4 Diving Casualty Investigation PDFFernando Cadena DuqueNo ratings yet
- Iso 24801 2 2007 FR en PDFDocument8 pagesIso 24801 2 2007 FR en PDFFernando Cadena DuqueNo ratings yet
- DAN EO2 Instructor GuideDocument46 pagesDAN EO2 Instructor GuideFernando Cadena DuqueNo ratings yet
- DeltaPHazards CADCDocument32 pagesDeltaPHazards CADCFernando Cadena DuqueNo ratings yet
- Diving Supervisor Guide TR 05-09Document39 pagesDiving Supervisor Guide TR 05-09Patricio Toledo FuenzalidaNo ratings yet
- Manual For Diving Safety: Scripps Institution of Oceanography University of California, San DiegoDocument58 pagesManual For Diving Safety: Scripps Institution of Oceanography University of California, San DiegoFernando Cadena DuqueNo ratings yet
- Disinfecting Scuba Equipment: The Future of Equipment Cleaning in The Wake of COVID-19Document24 pagesDisinfecting Scuba Equipment: The Future of Equipment Cleaning in The Wake of COVID-19Fernando Cadena DuqueNo ratings yet
- B-Virus Free: Removes Viruses, Bacteria, Moulds and Pollen From Breathing AirDocument5 pagesB-Virus Free: Removes Viruses, Bacteria, Moulds and Pollen From Breathing AirFernando Cadena DuqueNo ratings yet
- MOB USCG Boat Crew Seamanship Chapter 16 PDFDocument28 pagesMOB USCG Boat Crew Seamanship Chapter 16 PDFFernando Cadena DuqueNo ratings yet
- Mitchell - DCI Workshop 2 PDFDocument12 pagesMitchell - DCI Workshop 2 PDFFernando Cadena DuqueNo ratings yet
- Diving Unbilical SS521-AH-PRO-010Document83 pagesDiving Unbilical SS521-AH-PRO-010Fernando Cadena DuqueNo ratings yet
- Diver Medic BrochureDocument7 pagesDiver Medic BrochureFernando Cadena DuqueNo ratings yet
- PSDiverMonthlyIssue 111 SECUREDocument60 pagesPSDiverMonthlyIssue 111 SECUREFernando Cadena DuqueNo ratings yet
- CCC (Ue) Company ProfileDocument34 pagesCCC (Ue) Company Profilefaiz111180No ratings yet
- Underwater Construction PDFDocument12 pagesUnderwater Construction PDFastewayb_964354182No ratings yet
- Appendix I PMT GPP 05 (Installation)Document47 pagesAppendix I PMT GPP 05 (Installation)haydarburedahNo ratings yet
- DSV King FisherDocument11 pagesDSV King FisherJahel LootiNo ratings yet
- 95.4M / 300 Men Subsea Installation and Dive Support Barge: PW NatunaDocument1 page95.4M / 300 Men Subsea Installation and Dive Support Barge: PW NatunaIgorNo ratings yet
- OVPQ Master FullDocument40 pagesOVPQ Master FullFaidzy RahmanNo ratings yet
- Code of Practice For Offshore DivingDocument56 pagesCode of Practice For Offshore DivingDivers Dream PrahaNo ratings yet
- Breathing at Depth Physiologic and Clinical Aspects of Diving While Breathing Compressed Gas.Document26 pagesBreathing at Depth Physiologic and Clinical Aspects of Diving While Breathing Compressed Gas.FebyNo ratings yet
- Lloyd's - Register 2018Document188 pagesLloyd's - Register 2018Pranesh SbNo ratings yet
- Gas Supervisor QuestionsDocument3 pagesGas Supervisor QuestionsNicolas BesnardNo ratings yet
- Vessel Specs - OLV VENTURE 1 PDFDocument7 pagesVessel Specs - OLV VENTURE 1 PDFgo michibataNo ratings yet
- Offshore Diving Induction ProceduresDocument18 pagesOffshore Diving Induction Proceduresjeedan100% (1)
- SPHL Emergency Evacuation and Rescue ProceduresDocument30 pagesSPHL Emergency Evacuation and Rescue ProceduresPraise Sam Abraham100% (3)
- HSE L103 - 2014 - Commercial Diving Projects Offshore. Diving at Work Regulations 1997. Approved Code of PracticeDocument53 pagesHSE L103 - 2014 - Commercial Diving Projects Offshore. Diving at Work Regulations 1997. Approved Code of PracticeKris WilochNo ratings yet
- Benefits of Studying Traditional RemediesDocument41 pagesBenefits of Studying Traditional Remediesnada abdelrahmanNo ratings yet
- (Advances in Underwater Technology, Ocean Science and Offshore Engineering 1) James A. Lawrie (auth.) - Developments in Diving Technology_ Proceedings of an international conference, (Divetech ′84) or.pdfDocument159 pages(Advances in Underwater Technology, Ocean Science and Offshore Engineering 1) James A. Lawrie (auth.) - Developments in Diving Technology_ Proceedings of an international conference, (Divetech ′84) or.pdfQuyền Lê100% (2)
- L103 Acop Commercial Diving OffshoreDocument53 pagesL103 Acop Commercial Diving OffshorejohnNo ratings yet
- Diving SpreadDocument41 pagesDiving SpreadSyed Abdul RahmanNo ratings yet
- U-103 1st 2010 Petroleum Related Manned Underwater Operations InshoreDocument30 pagesU-103 1st 2010 Petroleum Related Manned Underwater Operations Inshoremechmohan26No ratings yet
- BWPRP4-Riser Clamp Installation ProcedureDocument56 pagesBWPRP4-Riser Clamp Installation Procedureelkrishnan100% (8)
- AF05-TECH.02 R00 - RANA AF05 Modular Saturation Diving System - Technical Data SheetDocument24 pagesAF05-TECH.02 R00 - RANA AF05 Modular Saturation Diving System - Technical Data SheetfrdsimNo ratings yet
- DSV RoyalIHCSeven Atlantic HSBDocument6 pagesDSV RoyalIHCSeven Atlantic HSBJorge Ricardo AlcivarNo ratings yet
- History - of - Underwater - Diving Surah Anbya Ayah 82Document25 pagesHistory - of - Underwater - Diving Surah Anbya Ayah 82qendrim zekaNo ratings yet
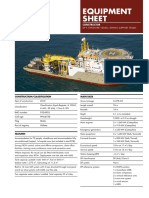
- Equipment Sheet: DP Ii Offshore Vessel / Diving Support VesselDocument2 pagesEquipment Sheet: DP Ii Offshore Vessel / Diving Support VesselGuest dstNo ratings yet
- Sat System RaffaellaDocument6 pagesSat System RaffaellaMarco VacchieriNo ratings yet
- 02 EPA EP72 GL 0052 Underwater Services Equipment SpecificationDocument94 pages02 EPA EP72 GL 0052 Underwater Services Equipment Specificationvijuindia1111No ratings yet
- 12 Man Saturation Diving System Rev 0Document20 pages12 Man Saturation Diving System Rev 0pert11No ratings yet
- Solarzilla ManualDocument45 pagesSolarzilla Manualmeor3705No ratings yet
- Catalogo Aqua AirDocument662 pagesCatalogo Aqua AirEvanotNo ratings yet
- UntitledDocument176 pagesUntitledldigasNo ratings yet