You might also like
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- Phase 2Document82 pagesPhase 2Sheila JuddNo ratings yet
- Treatment Planning: 5. Phase 3 RehabilitationDocument39 pagesTreatment Planning: 5. Phase 3 RehabilitationSheila JuddNo ratings yet
- Treatment Planning Tutorial: 3. Developing A Phase 1 Treatment PlanDocument56 pagesTreatment Planning Tutorial: 3. Developing A Phase 1 Treatment PlanSheila JuddNo ratings yet
- Treatment Planning in DentistryDocument87 pagesTreatment Planning in DentistrysamhitaNo ratings yet
- Day 1 - Thursday - 1030 AM - Andrew BucklerDocument21 pagesDay 1 - Thursday - 1030 AM - Andrew BucklerPrevent Cancer FoundationNo ratings yet
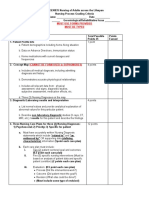
- Nursing Care Plan: Medical Diagnosis DX Procedures Labs MedicationsDocument3 pagesNursing Care Plan: Medical Diagnosis DX Procedures Labs MedicationsCaren CarlstedtNo ratings yet
- FCS (SA) Intermediate Paper 2 Blueprints 20-10-2019Document7 pagesFCS (SA) Intermediate Paper 2 Blueprints 20-10-2019Kishan NaiduNo ratings yet
- Prioritizing The Nursing: Problem ListDocument29 pagesPrioritizing The Nursing: Problem ListElay PedrosoNo ratings yet
- AMH Six Sigma Wait Time ProjectDocument26 pagesAMH Six Sigma Wait Time ProjectTania100% (1)
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- PN CJM AssignmentDocument7 pagesPN CJM Assignmenttcarmen49No ratings yet
- Benefit of Early Class II Treatment: Progress Report of A Two-Phase Randomized Clinical TrialDocument11 pagesBenefit of Early Class II Treatment: Progress Report of A Two-Phase Randomized Clinical TrialJoshua StalinNo ratings yet
- Post Test 13Document3 pagesPost Test 13Evangeline Olarte QuilantangNo ratings yet
- NCP Soft Copy LeonesDocument4 pagesNCP Soft Copy Leones2G Balatayo Joshua LeoNo ratings yet
- 5019 Changes in The Beck Depression Inventory II Scores of TMD Subjects After Measured Occlusal TreatmentDocument13 pages5019 Changes in The Beck Depression Inventory II Scores of TMD Subjects After Measured Occlusal TreatmentfebrinaNo ratings yet
- Q09070 Proposal Cheery TPZ in Cancer Phase II DM BS 20210125Document17 pagesQ09070 Proposal Cheery TPZ in Cancer Phase II DM BS 20210125Leo LiangNo ratings yet
- The Cynefin Framework Applying An Understanding ofDocument5 pagesThe Cynefin Framework Applying An Understanding ofleslie medinaNo ratings yet
- Sbar Nsg-ProcessDocument7 pagesSbar Nsg-ProcessShyra Mae Riano MarinNo ratings yet
- Must Use Forms Provided Must Be TypedDocument8 pagesMust Use Forms Provided Must Be TypedVincent Karimi GichimuNo ratings yet
- Patient Triage Data ChartDocument2 pagesPatient Triage Data ChartChandler BrownNo ratings yet
- CP StrokeDocument4 pagesCP Strokeratna kartikaNo ratings yet
- Managing Acute Heart Failure in The Emergency Department: Patient Case StudyDocument33 pagesManaging Acute Heart Failure in The Emergency Department: Patient Case StudyDummyAcc13No ratings yet
- NURSING-CARE-PLAN With AnswersDocument4 pagesNURSING-CARE-PLAN With AnswersTracy Malingin QuimqueNo ratings yet
- ADN Student Advancing Clinical Practice WorksheetDocument3 pagesADN Student Advancing Clinical Practice Worksheetdoirge47No ratings yet
- Clinical Diary FormatDocument2 pagesClinical Diary FormatGauravakansha YadavNo ratings yet
- Volume 03 No.4Document29 pagesVolume 03 No.4Rebin AliNo ratings yet
- 6 Care Plan DiarrheaDocument2 pages6 Care Plan DiarrheaTimi Terpstra75% (4)
- Perio LogbookDocument19 pagesPerio LogbookKarim Ahmed100% (1)
- Surgery and Diagnostic ReportDocument26 pagesSurgery and Diagnostic ReportElishaDaceyNo ratings yet
- Critical Pathways of CareDocument19 pagesCritical Pathways of CareNivedita NivuNo ratings yet
- CNP FormatDocument20 pagesCNP FormatRhona Mae HernandezNo ratings yet
- Jemmalyn M. Mallari Maria Allyna R. Mallari Bspt4 Objective Structured Clinical Examination (OSCE) - Neurological Rehabilitation Clinic DescriptionDocument6 pagesJemmalyn M. Mallari Maria Allyna R. Mallari Bspt4 Objective Structured Clinical Examination (OSCE) - Neurological Rehabilitation Clinic DescriptionCeline Kyla MalloNo ratings yet
- 2021 TDC Module Case Analysis GuidelinesDocument5 pages2021 TDC Module Case Analysis GuidelinesLeuqcar Ramos DonascoNo ratings yet
- Mrcs Part A Essential Revision Notes Boo K 1Document22 pagesMrcs Part A Essential Revision Notes Boo K 1Fath Elrahman MohammedNo ratings yet
- Module 4 NRG 203 Intrapartum - 2023 2024Document20 pagesModule 4 NRG 203 Intrapartum - 2023 2024alliahjaneadlawanNo ratings yet
- B1. QCC Mini Heart - Thailand Tobacco Monopoly HospitalDocument38 pagesB1. QCC Mini Heart - Thailand Tobacco Monopoly HospitalnurcholisNo ratings yet
- Cinical Duty Student Orientation Outline (N-109 MCN 2 RLE)Document2 pagesCinical Duty Student Orientation Outline (N-109 MCN 2 RLE)Krizelle MesinaNo ratings yet
- Clinical Final ExamDocument7 pagesClinical Final ExamsalamredNo ratings yet
- Brief Confusion Assessment Method (bCAM) : Instruction Manual v1Document11 pagesBrief Confusion Assessment Method (bCAM) : Instruction Manual v1AlejandroVargasNo ratings yet
- Module 4 Nursing ProcessDocument14 pagesModule 4 Nursing ProcessArjay Cuh-ingNo ratings yet
- (New) Case Study FormatDocument7 pages(New) Case Study FormatSophia Sweet SantosNo ratings yet
- Neonatal and EBM Case Report Guide 2023Document7 pagesNeonatal and EBM Case Report Guide 2023azri.hafiziNo ratings yet
- User's Guide For The Synoptic MRI Report For Pre-Operative Staging of Rectal Cancer, 2015 - CCOMRIRectalStagingUserGuideDocument25 pagesUser's Guide For The Synoptic MRI Report For Pre-Operative Staging of Rectal Cancer, 2015 - CCOMRIRectalStagingUserGuideСергей СадовниковNo ratings yet
- Perioperative Nursing Concept PDFDocument21 pagesPerioperative Nursing Concept PDFMari Fe100% (1)
- Piis0007091217349061 2Document6 pagesPiis0007091217349061 2Ana Belén Artero CastañoNo ratings yet
- Clinical Audit On Code BlueDocument7 pagesClinical Audit On Code BlueSunny AnthonyNo ratings yet
- 2 Making Clinical Decicions - Lifespan Neurorehabilitation 2018Document28 pages2 Making Clinical Decicions - Lifespan Neurorehabilitation 2018Abi Dennise Nahuelpán LienlafNo ratings yet
- Ramirez-Yañez 2008 JCPD 32 325-30Document6 pagesRamirez-Yañez 2008 JCPD 32 325-30Omer Roy MustafaNo ratings yet
- Risk Based E/M CodingDocument5 pagesRisk Based E/M CodingSandra WeeksNo ratings yet
- A3 ReportDocument4 pagesA3 ReportmfernandNo ratings yet
- Pedia Case Study FormatDocument4 pagesPedia Case Study FormatJohn Carlo B. Dungca100% (1)
- E&M Coding and Basic Questions. !Document12 pagesE&M Coding and Basic Questions. !Ashitha Km100% (1)
- PBS 324 TriageDataChartDocument1 pagePBS 324 TriageDataChartkayleeclements82No ratings yet
- NRS210 Clinical Assignment PacketDocument16 pagesNRS210 Clinical Assignment PacketSally GigelioNo ratings yet
- Scheduling Algorithm Applications To Solve Simple Problems in Diagnostic Related Health Care CentersDocument3 pagesScheduling Algorithm Applications To Solve Simple Problems in Diagnostic Related Health Care Centerschiranjeev sharmaNo ratings yet
- Case Analysis Format: Medical-Surgical & Maternal and Child Health Nursing ConceptsDocument4 pagesCase Analysis Format: Medical-Surgical & Maternal and Child Health Nursing ConceptsEmmy Flor ValmoriaNo ratings yet
- Moh Syahrul Discharge PlanningDocument16 pagesMoh Syahrul Discharge PlanningRulix SevenfoldNo ratings yet
- Point-of-Care Testing: Millennium Technology For Critical CareDocument7 pagesPoint-of-Care Testing: Millennium Technology For Critical CareDelladuasatu stellaNo ratings yet
- APN108-Assessment 1A-T3Document24 pagesAPN108-Assessment 1A-T3Rommisa ShujaNo ratings yet
- Faculty of Dentistry Academic Calendar 2018-2019Document179 pagesFaculty of Dentistry Academic Calendar 2018-2019Sheila JuddNo ratings yet
- IELTS Practice Tests by Peter May PDFDocument177 pagesIELTS Practice Tests by Peter May PDFSheila Judd78% (9)
- Prescribing and Dispensing Drugs: Standards & GuidelinesDocument15 pagesPrescribing and Dispensing Drugs: Standards & GuidelinesSheila JuddNo ratings yet
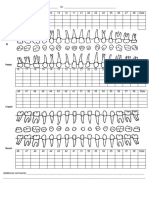
- Sample Odontogram Existing and Planned Treatment PDFDocument2 pagesSample Odontogram Existing and Planned Treatment PDFSheila Judd100% (1)
- Sample Periodontal Chart PDFDocument1 pageSample Periodontal Chart PDFSheila JuddNo ratings yet
- Sample Initial Periodontal Occlusal Examination Form PDFDocument1 pageSample Initial Periodontal Occlusal Examination Form PDFSheila JuddNo ratings yet
- Sample Initial Periodontal Occlusal Examination Form PDFDocument1 pageSample Initial Periodontal Occlusal Examination Form PDFSheila JuddNo ratings yet
- Sample Medical History Form77576Document1 pageSample Medical History Form77576Sheila JuddNo ratings yet
- Sample Odontogram Existing and Planned Treatment897Document2 pagesSample Odontogram Existing and Planned Treatment897Sheila Judd100% (1)
- Sample Initial Periodontal Occlusal Examination Form687585Document1 pageSample Initial Periodontal Occlusal Examination Form687585Sheila JuddNo ratings yet
- Patient-Centred Care and The Business of Dentistry: Standards & GuidelinesDocument6 pagesPatient-Centred Care and The Business of Dentistry: Standards & GuidelinesSheila JuddNo ratings yet
- Oral Cancer Clinical Practice GuidelineDocument8 pagesOral Cancer Clinical Practice GuidelineSheila JuddNo ratings yet
- DR - Shaheen Part 2 PDFDocument13 pagesDR - Shaheen Part 2 PDFmidhunNo ratings yet
- Cambra PDFDocument10 pagesCambra PDFSharlene OngNo ratings yet
- Concepts of AnchorageDocument9 pagesConcepts of AnchoragePooya FarNo ratings yet
- Digital Smile Design For Computer Assisted Esthetic RehabilitationDocument10 pagesDigital Smile Design For Computer Assisted Esthetic RehabilitationRoberto PucNo ratings yet
- Missionary Recommendation Physician Dental FormDocument5 pagesMissionary Recommendation Physician Dental FormdozieojiakuNo ratings yet
- Nutritional Status, Prevalence of Early Childhood.9Document7 pagesNutritional Status, Prevalence of Early Childhood.9drshailanathanNo ratings yet
- Dental Management of Children Undergoing Liver TransplantationDocument9 pagesDental Management of Children Undergoing Liver Transplantationwahyudi_donnyNo ratings yet
- C SpeeDocument4 pagesC SpeeCynthia AlfaroNo ratings yet
- Wells - OralanaDocument6 pagesWells - OralanaAlej DonesaNo ratings yet
- 2011 Comtemporary Periodontal Surgery CPCCDocument193 pages2011 Comtemporary Periodontal Surgery CPCCwuhan lalalaNo ratings yet
- Fixed MCQDocument9 pagesFixed MCQMahmoud EmeiraNo ratings yet
- 2011 EJED DitramaxDocument10 pages2011 EJED DitramaxPabloSevillaHernandezNo ratings yet
- Damon SystemDocument139 pagesDamon SystemYUYU189288% (8)
- Capítulo 4 Carranza 11 Ed.Document21 pagesCapítulo 4 Carranza 11 Ed.Estefanía Paz Torrejón GuzmánNo ratings yet
- PN 1Document1 pagePN 1Florin Eugen ConstantinescuNo ratings yet
- Introduction To ProthesisDocument56 pagesIntroduction To Prothesisreem eltyebNo ratings yet
- Tajweed (Picture Explaination)Document1 pageTajweed (Picture Explaination)JawedsIslamicLibrary100% (7)
- JConservDent263338-1469939 040459Document6 pagesJConservDent263338-1469939 040459Shubham KingraNo ratings yet
- FailuresinDentalImplants 2Document14 pagesFailuresinDentalImplants 2Muaadzatul izzahNo ratings yet
- Transpalatal, Nance & Lingual Arch Appliances: Clinical Tips and ApplicationsDocument9 pagesTranspalatal, Nance & Lingual Arch Appliances: Clinical Tips and Applicationsmr bể cáNo ratings yet
- Iñaki Gamborena 2020Document19 pagesIñaki Gamborena 2020Ulises DiazNo ratings yet
- In The Name of Allah The Most Gracious The Most MercifulDocument118 pagesIn The Name of Allah The Most Gracious The Most Mercifulkhlid21mtz100% (2)
- Orthodontics BlueprintDocument2 pagesOrthodontics BlueprintRamy FathyNo ratings yet
- Traumatogenic Occlusion in A Pediatric Dental Patient: A Case ReportDocument45 pagesTraumatogenic Occlusion in A Pediatric Dental Patient: A Case ReportShameena KnNo ratings yet
- Prosthetic Options For Implant-Supported Overdentures - October 2015 - Inside DentistryDocument4 pagesProsthetic Options For Implant-Supported Overdentures - October 2015 - Inside Dentistrymaithilieaggarwalmds2124No ratings yet
- Colgate Brand: Prepared byDocument20 pagesColgate Brand: Prepared bykrunalNo ratings yet
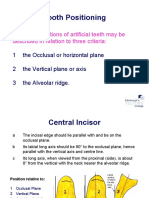
- Tooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaDocument19 pagesTooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaCherine SnookNo ratings yet
- 1 eNDODONTICS To PrintDocument19 pages1 eNDODONTICS To PrintDENTAL REVIEWER ONLYNo ratings yet
- Oral and Dental HistologyDocument6 pagesOral and Dental HistologyCésar HelenoNo ratings yet
- Kertas Soalan Peperiksaan Bulan Oktober. Y1docxDocument7 pagesKertas Soalan Peperiksaan Bulan Oktober. Y1docxAmin NuruddinNo ratings yet