You might also like
- Jumping Compactor Inspection ChecklistDocument1 pageJumping Compactor Inspection Checklistarunjith rNo ratings yet
- JSA - Batching Plant OperationDocument3 pagesJSA - Batching Plant OperationNisith SahooNo ratings yet
- SPI HSE FR 02 Tower Erection ChecklistDocument1 pageSPI HSE FR 02 Tower Erection ChecklistChandan KumarNo ratings yet
- Boom Placer Inspection ChecklistDocument1 pageBoom Placer Inspection ChecklistMyo LwinNo ratings yet
- Daily Safety ChecklistDocument4 pagesDaily Safety ChecklistKalyan ReddyNo ratings yet
- Luffing Tower Crane Preshift InspectionDocument1 pageLuffing Tower Crane Preshift InspectionEdmond KeraNo ratings yet
- Fire Water TankDocument1 pageFire Water TankAnonymous yCpjZF1rFNo ratings yet
- Transit Mixer Safety Inspection Checklist: SR. No Item OK Not OK NA RemarksDocument1 pageTransit Mixer Safety Inspection Checklist: SR. No Item OK Not OK NA RemarksRísês ÃfrözNo ratings yet
- RS Concrete Pumping Risk AssessmentDocument8 pagesRS Concrete Pumping Risk AssessmentLito PanchoNo ratings yet
- Piling Rig Plant Pre-Acceptance ChecklisDocument3 pagesPiling Rig Plant Pre-Acceptance Checklisosama F. MohamedNo ratings yet
- Manual Handling ChartDocument20 pagesManual Handling ChartTatak Bay Ahmed100% (1)
- WAH - Working On Roofs - 0Document13 pagesWAH - Working On Roofs - 0Rizki DarmawanNo ratings yet
- SWP-SF010A - 6 Daily Vibratory Roller Compactor Rev. ADocument1 pageSWP-SF010A - 6 Daily Vibratory Roller Compactor Rev. ACliffordNo ratings yet
- Frames Erection ProcDocument18 pagesFrames Erection Procrobby_hipNo ratings yet
- Movable Tower Light-Monthly Inspection Checklist: Acceptable Not Acceptable N/ADocument1 pageMovable Tower Light-Monthly Inspection Checklist: Acceptable Not Acceptable N/Amunna yadav100% (1)
- Job Safety Analysis: Helmet, Shoes, Goggles, Leather Gloves, Noise Mask, Face Shield, Apron EtcDocument3 pagesJob Safety Analysis: Helmet, Shoes, Goggles, Leather Gloves, Noise Mask, Face Shield, Apron Etc123shripadNo ratings yet
- Fire Safety Checklist for Construction SitesDocument1 pageFire Safety Checklist for Construction SitesJosiahNo ratings yet
- De-Shuttering PermitDocument1 pageDe-Shuttering PermitHariharan Muthukrishanan100% (1)
- 07 - TDS - Masterflow 520Document3 pages07 - TDS - Masterflow 520Alexi ALfred H. TagoNo ratings yet
- Scissor Lift Maintenance Inspection ReportDocument3 pagesScissor Lift Maintenance Inspection ReportAfiq BxrnNo ratings yet
- Batching Plant Method StatmentDocument9 pagesBatching Plant Method Statmentmohamed.elkomyNo ratings yet
- Dr. Nirali Patel Pediatric Emergency MedicineDocument31 pagesDr. Nirali Patel Pediatric Emergency Medicinemarsan12No ratings yet
- Consolidated Construction Consortium LTD.: DOC No.:CCCL/HSE/003 OCP No.31 DateDocument1 pageConsolidated Construction Consortium LTD.: DOC No.:CCCL/HSE/003 OCP No.31 DateradhouaneNo ratings yet
- Fan InstallationDocument2 pagesFan InstallationKrishna PatilNo ratings yet
- Scissor Lift Pre-Use Inspection Checklist 2Document1 pageScissor Lift Pre-Use Inspection Checklist 2Harun SaniNo ratings yet
- Pre Mob Flatbed Truck Daily Inspection Checklist FormDocument3 pagesPre Mob Flatbed Truck Daily Inspection Checklist Formagusbudianto.dk168No ratings yet
- GD380A-L ListDocument6 pagesGD380A-L ListNam Won HongNo ratings yet
- Monthly Ladder Inspection ChecklistDocument1 pageMonthly Ladder Inspection ChecklistshahidNo ratings yet
- Asian Paints - Prem Gloss EnamelDocument1 pageAsian Paints - Prem Gloss EnamelwilliumstNo ratings yet
- Daily checklist inspection derrick winchDocument2 pagesDaily checklist inspection derrick winchangger aminda noorcipta joharNo ratings yet
- Concrete Mixer Safety ChecklistDocument1 pageConcrete Mixer Safety ChecklistSafety Man Shop100% (1)
- Application To Perform Work - Grass CuttingDocument2 pagesApplication To Perform Work - Grass CuttingRauf HuseynovNo ratings yet
- Bar Cutting Machine Safety Inspection ChecklistDocument1 pageBar Cutting Machine Safety Inspection ChecklistsanjeetNo ratings yet
- Job Safety Analysis: S.No Activities Hazard Risk Control MeasuresDocument2 pagesJob Safety Analysis: S.No Activities Hazard Risk Control Measureskhaja asifuddinNo ratings yet
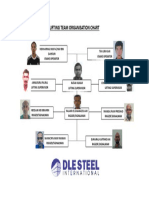
- Lifting Team Organisation ChartDocument1 pageLifting Team Organisation ChartGricNo ratings yet
- Tower Light Inspection ChecklistDocument1 pageTower Light Inspection ChecklistHabib ur rahmanNo ratings yet
- Weekly Tower Light Check ListDocument1 pageWeekly Tower Light Check ListpjosesmNo ratings yet
- Flagman & Lookout Requirement for Vehicle ReversingDocument1 pageFlagman & Lookout Requirement for Vehicle ReversingarslanahmedkhawajaNo ratings yet
- Rigging Up Checklist: Rig ModelDocument2 pagesRigging Up Checklist: Rig Model89simbuNo ratings yet
- QUSAHWIRA FIELD DEVELOPMENTDocument1 pageQUSAHWIRA FIELD DEVELOPMENTJayaprakasan Koyadan KorothNo ratings yet
- Risk Assessment - Tower DecommissioningDocument5 pagesRisk Assessment - Tower DecommissioningJeffery Mulei100% (1)
- Air Compressor Risk MG T FormDocument8 pagesAir Compressor Risk MG T FormFateh AliyaNo ratings yet
- The 12 Golden Rules: Safety at WorkDocument11 pagesThe 12 Golden Rules: Safety at WorkStacey FejerNo ratings yet
- Daily TBT Attendance Record 4Document1 pageDaily TBT Attendance Record 4Mobin Thomas AbrahamNo ratings yet
- Compactor Daily Inspection ChecklistDocument1 pageCompactor Daily Inspection ChecklistThandabantu Magengelele33% (3)
- 17.scafold Inspection UNISCO (PF) - 17Document2 pages17.scafold Inspection UNISCO (PF) - 17Benasher IbrahimNo ratings yet
- Job Hazard Analysis DemolishDocument4 pagesJob Hazard Analysis Demolishyajid bustomiNo ratings yet
- YZ12HD Vibratory Roller SpecsDocument4 pagesYZ12HD Vibratory Roller SpecsIwa RizaNo ratings yet
- Manual Chain Hoist Inspection Checklist: Health, Safety and Environment Management SystemDocument1 pageManual Chain Hoist Inspection Checklist: Health, Safety and Environment Management SystemEdward DineshNo ratings yet
- Truck Crane Inspection FormDocument3 pagesTruck Crane Inspection FormAdhy Darmawan100% (1)
- Mobile Scaffold Inspection ChecklistDocument3 pagesMobile Scaffold Inspection Checklistanthony murphyNo ratings yet
- All JSAsDocument88 pagesAll JSAsQamar KhanNo ratings yet
- EHS 2-F8 PTW LiftingDocument2 pagesEHS 2-F8 PTW LiftingLee Xiao YuNo ratings yet
- Truck Inspection Checklist 2021Document1 pageTruck Inspection Checklist 2021muhammad anasNo ratings yet
- 28.1.1 Mobile Equipment Inspection ChecklistDocument1 page28.1.1 Mobile Equipment Inspection Checklistmohamed abdelmoniemNo ratings yet
- Index: Cv. Dira Utama SejahteraDocument12 pagesIndex: Cv. Dira Utama SejahteraFreshop SurabayaNo ratings yet
- SOP Module Unloading & StorageDocument1 pageSOP Module Unloading & StorageRahul SahaNo ratings yet
- Standard PDF en PDFDocument1 pageStandard PDF en PDFMohamed Moustafa ElashwahNo ratings yet
- Checked, Approved and in Good Working Order Checked, Found Faulty, Notified Supervisor Not Applicable To This ItemDocument1 pageChecked, Approved and in Good Working Order Checked, Found Faulty, Notified Supervisor Not Applicable To This ItemMohamed Moustafa ElashwahNo ratings yet
- Er 10 4 01Document8 pagesEr 10 4 01Mohammad Shafaet JamilNo ratings yet
- Yr 3 R5Document32 pagesYr 3 R5Mohamed Moustafa ElashwahNo ratings yet
- Menna Car Repair HistoryDocument1 pageMenna Car Repair HistoryMohamed Moustafa ElashwahNo ratings yet
- TextDocument1 pageTextMohamed Moustafa ElashwahNo ratings yet
- Maintenance Management Information Syste PDFDocument6 pagesMaintenance Management Information Syste PDFMohamed Moustafa ElashwahNo ratings yet
- Checked, Approved and in Good Working Order Checked, Found Faulty, Notified Supervisor Not Applicable To This ItemDocument1 pageChecked, Approved and in Good Working Order Checked, Found Faulty, Notified Supervisor Not Applicable To This ItemMohamed Moustafa ElashwahNo ratings yet
- Construction Equipment PlanningDocument33 pagesConstruction Equipment PlanningMohamed Moustafa ElashwahNo ratings yet
- Standard PDF en PDFDocument1 pageStandard PDF en PDFMohamed Moustafa ElashwahNo ratings yet
- Fundamentals of Reliability Engineering - Part 1 Feb 2012Document59 pagesFundamentals of Reliability Engineering - Part 1 Feb 2012Mohamed Moustafa Elashwah100% (1)
- Maintenance Repair Request Form PDFDocument1 pageMaintenance Repair Request Form PDFMohamed Moustafa ElashwahNo ratings yet
- Excel Tutorial: Learn Formatting, Charts, and MoreDocument12 pagesExcel Tutorial: Learn Formatting, Charts, and Moremjay15No ratings yet
- RD218 Gardan 3110 Ob2226657 NDocument1 pageRD218 Gardan 3110 Ob2226657 Nopen hartigNo ratings yet
- Large Generators WEBDocument16 pagesLarge Generators WEBMaycon MaranNo ratings yet
- Teachers' Notes: ©film Education 1Document20 pagesTeachers' Notes: ©film Education 1רז ברקוNo ratings yet
- Student quiz answer sheetsDocument26 pagesStudent quiz answer sheetsSeverus S PotterNo ratings yet
- CSE 323-Final-Summer 2021Document2 pagesCSE 323-Final-Summer 2021nahimur rahmanNo ratings yet
- Diagnosing and Managing Acute and Chronic SinusitisDocument14 pagesDiagnosing and Managing Acute and Chronic SinusitisAnonymous y3TIOwX8100% (1)
- SECURED TRANSACTION BAR CHECKLISTDocument4 pagesSECURED TRANSACTION BAR CHECKLISTatw4377100% (1)
- Self-test on the COSO ERM frameworkDocument6 pagesSelf-test on the COSO ERM frameworkLady BirdNo ratings yet
- TEFL I Course Prepares Students to Teach EnglishDocument8 pagesTEFL I Course Prepares Students to Teach EnglishErma DomosNo ratings yet
- Beowulf The Monsters and The Critics SevDocument20 pagesBeowulf The Monsters and The Critics SevNirmala GaneshNo ratings yet
- Neil Strauss - The Annihilation Method - Style's Archives - Volume 1 - The Origin of Style - How To Transform From Chump To Champ in No TimeDocument132 pagesNeil Strauss - The Annihilation Method - Style's Archives - Volume 1 - The Origin of Style - How To Transform From Chump To Champ in No TimeDaniel Nii Armah Tetteh100% (2)
- Fundamentals Deep Learning Activation Functions When To Use ThemDocument15 pagesFundamentals Deep Learning Activation Functions When To Use ThemfaisalNo ratings yet
- African in The Modern WorldDocument18 pagesAfrican in The Modern WorldSally AnkomaahNo ratings yet
- Staff Nurse HallticketDocument2 pagesStaff Nurse HallticketHiking DiaryNo ratings yet
- Airport Design GuidelinesDocument408 pagesAirport Design Guidelinesnickolololo67% (9)
- Lembar Jawaban Skillab Evidence Based Medicine (Ebm) Nama: Rafika Triasa NIM: 040427223270003Document11 pagesLembar Jawaban Skillab Evidence Based Medicine (Ebm) Nama: Rafika Triasa NIM: 040427223270003Yahya Darmais FaridNo ratings yet
- Frogkisser! by Garth Nix (Excerpt)Document17 pagesFrogkisser! by Garth Nix (Excerpt)I Read YA0% (1)
- Asme B18.24-2020Document190 pagesAsme B18.24-2020윤규섭0% (1)
- OnScreen B2 Quiz 2ADocument2 pagesOnScreen B2 Quiz 2ALaura B.100% (1)
- Hajipur Resume GVVDocument2 pagesHajipur Resume GVVRajnish JhaNo ratings yet
- READING U8Document4 pagesREADING U8Như TrầnNo ratings yet
- WordPress Introduction: CMS BasicsDocument21 pagesWordPress Introduction: CMS BasicsNgô Ngọc Hải phươngNo ratings yet
- tmp82D3 TMPDocument12 pagestmp82D3 TMPFrontiersNo ratings yet
- 32 Productivity Increase in A PeirceSmith Convert 153013Document14 pages32 Productivity Increase in A PeirceSmith Convert 153013amirlpNo ratings yet
- Kristine Jane T. Zipagan Assignment: 1. Parts of InfographicsDocument2 pagesKristine Jane T. Zipagan Assignment: 1. Parts of InfographicsChristyNo ratings yet
- Saura, Jasmin E. - DVM - 2B Biochemistry (Activity 2)Document2 pagesSaura, Jasmin E. - DVM - 2B Biochemistry (Activity 2)Jasmin SauraNo ratings yet
- Lyrics: Original Songs: - JW BroadcastingDocument56 pagesLyrics: Original Songs: - JW BroadcastingLucky MorenoNo ratings yet
- Micro800 4-Channel and 8-Channel Analog Voltage/Current Input and Output ModulesDocument12 pagesMicro800 4-Channel and 8-Channel Analog Voltage/Current Input and Output ModulesSyarifudin WahidNo ratings yet
- CEO Corner New Products Powerful Pocket SimulatorDocument23 pagesCEO Corner New Products Powerful Pocket SimulatorMOHAMMA MUSANo ratings yet
- B1 UDO Trace LogDocument14 pagesB1 UDO Trace LogCh M KashifNo ratings yet