You might also like
- Covid FormDocument3 pagesCovid FormGena Fe L. JagusNo ratings yet
- Visitor Health Declaration FormDocument2 pagesVisitor Health Declaration FormKaryl Eunice Macabale IboniaNo ratings yet
- Borang PENGISYTIHARAN KESIHATANDocument1 pageBorang PENGISYTIHARAN KESIHATANأميرول آدمNo ratings yet
- COVID-19 (Coronavirus) Exposure Questionnaire: Part 1 - Applicable For All ApplicantsDocument2 pagesCOVID-19 (Coronavirus) Exposure Questionnaire: Part 1 - Applicable For All ApplicantsMovin PrabhakaranNo ratings yet
- Daily Health Screening Checklist - COVID19 (For Visitors) : TemperatureDocument2 pagesDaily Health Screening Checklist - COVID19 (For Visitors) : TemperatureHelen GamboaNo ratings yet
- Health Declaration Form1Document2 pagesHealth Declaration Form1JULCON ARAIZNo ratings yet
- Health ChecklistDocument14 pagesHealth ChecklistClark Kent BatucanNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJilli JardiolinNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration Formmalaki ang titik ONo ratings yet
- A Healthy World Starts Here: Nwdi Requirements For Sars Cov-2 (Covid-19) Antibody Rapid Diagnostic TestDocument2 pagesA Healthy World Starts Here: Nwdi Requirements For Sars Cov-2 (Covid-19) Antibody Rapid Diagnostic TestEric NagumNo ratings yet
- COVID 19 Revised Monitoring Form 2021Document3 pagesCOVID 19 Revised Monitoring Form 2021Aaron Paul BernasNo ratings yet
- Covid Screening (Passive Screening)Document2 pagesCovid Screening (Passive Screening)danushaNo ratings yet
- Inbound 2251609052538566261Document1 pageInbound 2251609052538566261sam.sarip0No ratings yet
- Health Screening Form For Visitors: Dear Valued Clients and VisitorsDocument1 pageHealth Screening Form For Visitors: Dear Valued Clients and VisitorsBhonNo ratings yet
- Covid 19 Exposure Questionnaire May 2020Document2 pagesCovid 19 Exposure Questionnaire May 2020Selma Violon PepitoNo ratings yet
- Annex B - Health Screening Form For VisitorsDocument1 pageAnnex B - Health Screening Form For VisitorsReynaldo YuNo ratings yet
- ISO Health ChecklistDocument1 pageISO Health ChecklistRonnel SaludezNo ratings yet
- Health Checklist 2Document2 pagesHealth Checklist 2Ria HernandezNo ratings yet
- COVID-19 Patient Reporting Form: Reporter InformationDocument2 pagesCOVID-19 Patient Reporting Form: Reporter InformationShinta Devianti100% (1)
- Patient Registration Packet For COVID Vaccine 1.19.2021Document3 pagesPatient Registration Packet For COVID Vaccine 1.19.2021Revengie CunalibanNo ratings yet
- Brainy Bunch - Health Declaration FormDocument1 pageBrainy Bunch - Health Declaration Formsarahhazwani56No ratings yet
- HD - Reception SantierraDocument1 pageHD - Reception SantierraAnezka Danett CortinaNo ratings yet
- MAO Self Declaration FormDocument1 pageMAO Self Declaration FormShan Eean TolentinoNo ratings yet
- COVID Patient Questinnaire FormDocument1 pageCOVID Patient Questinnaire Formanshum guptaNo ratings yet
- Cecilio Apostol Elementary School Attendees' Health ChecklistDocument1 pageCecilio Apostol Elementary School Attendees' Health ChecklistMikoy Fordan AntolinoNo ratings yet
- Health and Safety Declaration Form July 2020 - March 29, 2021Document1 pageHealth and Safety Declaration Form July 2020 - March 29, 2021mistyNo ratings yet
- Covid Screening ToolDocument1 pageCovid Screening TooljpNo ratings yet
- Asian Hospital Consult FormDocument1 pageAsian Hospital Consult FormEmily AdedojaNo ratings yet
- Health Declaration ChecklistDocument2 pagesHealth Declaration ChecklistCatherine Caluste AlipatNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Covid-19 Health DeclarationDocument1 pageCovid-19 Health DeclarationManpreetNo ratings yet
- Health DEclaration Form SET ADocument26 pagesHealth DEclaration Form SET AROLLY BALONo ratings yet
- COVID-19 Health Declaration FormDocument1 pageCOVID-19 Health Declaration Formkrizzane SuriaNo ratings yet
- DateDocument1 pageDateEarn cruzNo ratings yet
- Health Declaration Form 1Document2 pagesHealth Declaration Form 1Elorde M. ShalaniNo ratings yet
- CovidDocument2 pagesCovidJhun EspinaNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormJANET ILLESESNo ratings yet
- COVID-19 Screening Questionnaire - Ed2Document2 pagesCOVID-19 Screening Questionnaire - Ed2GilbertNo ratings yet
- Seafarer's Declaration at The Company DoctorDocument1 pageSeafarer's Declaration at The Company Doctorranjit malikNo ratings yet
- Daily Covid-19 Symptom Monitoring LogDocument5 pagesDaily Covid-19 Symptom Monitoring LogDaud HussainNo ratings yet
- Please Answer The Following Questions Truthfully. 2.: Tick Yes/NoDocument2 pagesPlease Answer The Following Questions Truthfully. 2.: Tick Yes/NoSusan Loida SorianoNo ratings yet
- Consent FormDocument2 pagesConsent FormDon Renz San JoseNo ratings yet
- COVID-19 (Coronavirus) Recovery QuestionnaireDocument3 pagesCOVID-19 (Coronavirus) Recovery QuestionnaireHasilwan ChanNo ratings yet
- Luciano Lombardi Derecktor Dania Fortlauder Dale, FL 33004: Test ReportDocument2 pagesLuciano Lombardi Derecktor Dania Fortlauder Dale, FL 33004: Test ReportLuciano LombardiNo ratings yet
- BlehDocument3 pagesBlehkula diamondNo ratings yet
- COVID-19 Physician/Patient Notes For Employers: - As of May 20, 2020 - Health Policy and PhysicianDocument3 pagesCOVID-19 Physician/Patient Notes For Employers: - As of May 20, 2020 - Health Policy and Physiciansecretos webNo ratings yet
- Student Health Assessment FormDocument1 pageStudent Health Assessment Formhey cuteNo ratings yet
- SMI COVID-19 Health Survey Form - RevisedDocument2 pagesSMI COVID-19 Health Survey Form - RevisedJess Rey Q. BaranNo ratings yet
- Norsu Health Declaration Form 1 September 2022Document1 pageNorsu Health Declaration Form 1 September 2022Joshua Allen AjetoNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
- Vera Gonzalez Pia NA NA, FL 33139 Test ReportDocument2 pagesVera Gonzalez Pia NA NA, FL 33139 Test ReportClaudio PereiraNo ratings yet
- Health Declaration Slip: (For Contact Tracing)Document2 pagesHealth Declaration Slip: (For Contact Tracing)Aylene GersanibNo ratings yet
- (Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureDocument1 page(Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureNatividad Jo Ann CuadroNo ratings yet
- Dhiraj Mishra: COVID-19 (Coronavirus) Exposure QuestionnaireDocument3 pagesDhiraj Mishra: COVID-19 (Coronavirus) Exposure QuestionnaireadiNo ratings yet
- Health Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Document1 pageHealth Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Jhon Micheal AlicandoNo ratings yet
- Health Checklist Employees 1 Converted 1Document2 pagesHealth Checklist Employees 1 Converted 1the7thAliceNo ratings yet
- ACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DEDocument1 pageACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DERoden BernardoNo ratings yet
- Health Declaration Checklist For Feb 4 & 6 Bar ExaminationDocument1 pageHealth Declaration Checklist For Feb 4 & 6 Bar ExaminationMark GeronimoNo ratings yet
- Result 14164 00251Document2 pagesResult 14164 00251Ministerio Sobrenatural GlobalNo ratings yet
- Observation ReportDocument3 pagesObservation ReportCatherine Jane CallangaNo ratings yet
- Observation ReportDocument9 pagesObservation ReportCatherine Jane CallangaNo ratings yet
- Evaluation of FlourDocument1 pageEvaluation of FlourCatherine Jane CallangaNo ratings yet
- QA Management Plan (Magna Prime)Document2 pagesQA Management Plan (Magna Prime)Catherine Jane CallangaNo ratings yet
- Food Safety Audit: Qa DepartmentDocument10 pagesFood Safety Audit: Qa DepartmentCatherine Jane CallangaNo ratings yet
- Process Flow LUZONDocument1 pageProcess Flow LUZONCatherine Jane CallangaNo ratings yet
- Process Flow DAVAODocument1 pageProcess Flow DAVAOCatherine Jane CallangaNo ratings yet
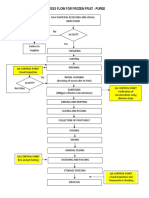
- Process Flow (Fruit Puree)Document1 pageProcess Flow (Fruit Puree)Catherine Jane CallangaNo ratings yet
- Q1. Do Control Measure/s Exist: Not A CCPDocument1 pageQ1. Do Control Measure/s Exist: Not A CCPCatherine Jane CallangaNo ratings yet
- System, Cleaning and Sanitizing Monitoring FormDocument1 pageSystem, Cleaning and Sanitizing Monitoring FormCatherine Jane CallangaNo ratings yet
- Sanitation Standard Operating ProcedureDocument6 pagesSanitation Standard Operating ProcedureCatherine Jane CallangaNo ratings yet
- Safety and Health Policy and ProcedureDocument11 pagesSafety and Health Policy and ProcedureCatherine Jane CallangaNo ratings yet
- 2 5WSafeFoodHandlingDocument14 pages2 5WSafeFoodHandlingkhairil2781No ratings yet
- Glass and Hard Plastic ControlDocument1 pageGlass and Hard Plastic ControlCatherine Jane Callanga100% (2)
- Necija Po - 080811 For Local and PolytradeDocument3 pagesNecija Po - 080811 For Local and PolytradeCatherine Jane CallangaNo ratings yet