You might also like
- Cardiac Diagnostic TestsDocument14 pagesCardiac Diagnostic TestsSimran Josan100% (5)
- Obstructive UropathyDocument3 pagesObstructive UropathyGerardLum100% (1)
- Anatomy and Physiology of HeartDocument2 pagesAnatomy and Physiology of HeartSimran JosanNo ratings yet
- Contributing Factors and Treatment of Benign Prostatic HyperplasiaDocument1 pageContributing Factors and Treatment of Benign Prostatic HyperplasiaSarah RonquilloNo ratings yet
- Assessment, Diagnosis, Planning, Intervention and Evaluation of a Client with Increased Airway SecretionsDocument3 pagesAssessment, Diagnosis, Planning, Intervention and Evaluation of a Client with Increased Airway SecretionsNicholas TagleNo ratings yet
- Case Study TabhsoDocument7 pagesCase Study TabhsoGina Barredo Bustamante100% (1)
- Cardiac Tamponade, Also Known As Pericardial Tamponade, Is AnDocument7 pagesCardiac Tamponade, Also Known As Pericardial Tamponade, Is AnSimran Josan100% (1)
- SUBMITTED TO - Resp. Mr. Somorjit SinghDocument8 pagesSUBMITTED TO - Resp. Mr. Somorjit SinghSimran JosanNo ratings yet
- Introduction to Ida Jean Orlando's Nursing TheoryDocument52 pagesIntroduction to Ida Jean Orlando's Nursing TheorySimran Josan100% (1)
- Acynotic Heart DiseasesDocument13 pagesAcynotic Heart DiseasesSimran JosanNo ratings yet
- Hirschsprung Disease: A Congenital Birth Defect of the IntestinesDocument3 pagesHirschsprung Disease: A Congenital Birth Defect of the IntestinesJan Rae Barnatia AtienzaNo ratings yet
- PathophysiologyDocument4 pagesPathophysiologyAngelou Joefred Congreso100% (1)
- Guideline Eeg Pediatric 2012Document60 pagesGuideline Eeg Pediatric 2012Chindia Bunga100% (1)
- NURSING CARE PLAN-Impired Physical MobilityDocument5 pagesNURSING CARE PLAN-Impired Physical MobilityKathleen Leana Viray JeanjaquetNo ratings yet
- LESSON PLAN ON CommunicationDocument11 pagesLESSON PLAN ON CommunicationSimran Josan100% (6)
- Single Patch Test PDFDocument17 pagesSingle Patch Test PDFmimienamNo ratings yet
- Scientific Analysis Goal: Goal:: Subjective CuesDocument2 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- Assessing and Managing Ineffective Airway ClearanceDocument3 pagesAssessing and Managing Ineffective Airway ClearanceNelle Agni100% (1)
- ABG Analysis Guide for NursesDocument6 pagesABG Analysis Guide for NursesSimran Josan100% (4)
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- ENDOTRACHEAL INTUBATIOn SandeepDocument17 pagesENDOTRACHEAL INTUBATIOn SandeepSimran JosanNo ratings yet
- SP CSDocument4 pagesSP CSKhan HansNo ratings yet
- Course Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsDocument8 pagesCourse Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsSimran JosanNo ratings yet
- Introduction AbsenteeismDocument23 pagesIntroduction AbsenteeismVasanthi Shashi Kiran73% (11)
- Precipitating Factors: Alcoholism Diet ( FAT) Hypertension Predisposing FactorsDocument1 pagePrecipitating Factors: Alcoholism Diet ( FAT) Hypertension Predisposing FactorsKevin Jade HerreraNo ratings yet
- Orem's Self-Care Deficit Nursing TheoryDocument45 pagesOrem's Self-Care Deficit Nursing TheorySimran JosanNo ratings yet
- Nursing Process and Care PlansDocument2 pagesNursing Process and Care PlansSimran Josan63% (8)
- Unit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsDocument4 pagesUnit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsSimran Josan100% (1)
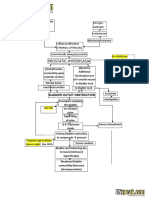
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDocument2 pagesBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNo ratings yet
- Drug StudyDocument4 pagesDrug StudyPam RomeroNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Hepatitis A PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Hepatitis A PDFswapnilazarusNo ratings yet
- FHNCP SmokingDocument1 pageFHNCP SmokingGamer DogeNo ratings yet
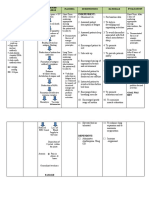
- NCP (BPH)Document8 pagesNCP (BPH)NataCo50% (2)
- Drug-Study NCPDocument5 pagesDrug-Study NCPMURILLO, FRANK JOMARI C.No ratings yet
- NCPDocument2 pagesNCPsphinx809100% (2)
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Short TermDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Short TermFrancis Xavier S. MendezNo ratings yet
- Cefipime HCL (AXERA)Document2 pagesCefipime HCL (AXERA)Kristine YoungNo ratings yet
- Adolescent NCPDocument1 pageAdolescent NCPClaire DobleNo ratings yet
- Basic Concept Map - RH IncompatibilityDocument1 pageBasic Concept Map - RH IncompatibilityTechnoShindoNo ratings yet
- Hypovolemic Shock Concept MapDocument1 pageHypovolemic Shock Concept MapJM AsentistaNo ratings yet
- SildenafilDocument2 pagesSildenafilSheryl Ann PedinesNo ratings yet
- Nursing Care Plan for Functional Urinary IncontinenceDocument4 pagesNursing Care Plan for Functional Urinary IncontinenceJez RarangNo ratings yet
- NCP (Acute Pain)Document2 pagesNCP (Acute Pain)jennilois100% (1)
- NCP SeratroDocument2 pagesNCP SeratroKristine YoungNo ratings yet
- Sample (Concept Map)Document1 pageSample (Concept Map)NMDNMSSDNo ratings yet
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationDocument1 pageNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationCharina AubreyNo ratings yet
- Acute Pain Nursing Diagnosis and InterventionsDocument2 pagesAcute Pain Nursing Diagnosis and InterventionsSheril Sularte CasanesNo ratings yet
- Abc NCPDocument3 pagesAbc NCPKL AstudilloNo ratings yet
- NCP Proper - Obstructive JaundiceDocument8 pagesNCP Proper - Obstructive JaundiceWyen Cabatbat100% (1)
- Assessing Nursing Diagnoses and Expected OutcomesDocument20 pagesAssessing Nursing Diagnoses and Expected OutcomesZamranosNo ratings yet
- Assessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationDocument6 pagesAssessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationimnasNo ratings yet
- NCP H MoleDocument6 pagesNCP H MoleMina RacadioNo ratings yet
- Cues Nursing Diagnosis Rationale Planning Nursing Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Rationale Planning Nursing Intervention Rationale EvaluationErika Mae MananganNo ratings yet
- NURSING CARE PLAN (Disturbed Body Image)Document1 pageNURSING CARE PLAN (Disturbed Body Image)Kay D. BeredoNo ratings yet
- NCP Self Care DeficitDocument3 pagesNCP Self Care DeficitLeizel ApolonioNo ratings yet
- Cystic Mass PathophysiologyDocument1 pageCystic Mass PathophysiologyMa Cheryll DueñasNo ratings yet
- Ncp-For-Sle-Fatigue-And-Pain EDITEDDocument4 pagesNcp-For-Sle-Fatigue-And-Pain EDITEDJordz PlaciNo ratings yet
- Nursing Care Plan - Fatigue (Antepartum)Document3 pagesNursing Care Plan - Fatigue (Antepartum)kaimimiyaNo ratings yet
- Measles PathophysiologyDocument1 pageMeasles PathophysiologyAl TheóNo ratings yet
- NCP - ERDocument5 pagesNCP - ERAnnelore ArcayNo ratings yet
- Nursing Care Plan NCP Group 3 Fatigue ..Document2 pagesNursing Care Plan NCP Group 3 Fatigue ..Aerron Severus Secano ShuldbergNo ratings yet
- CopdDocument6 pagesCopdapi-3717941100% (2)
- Pathophysiology of mesenchymal chondrosarcomaDocument7 pagesPathophysiology of mesenchymal chondrosarcomaMaria Grace Raquel Ormeneta100% (1)
- NURSING CARE PLAN Dog Bite InjuryDocument3 pagesNURSING CARE PLAN Dog Bite Injurykarrey danielNo ratings yet
- Breast Cancer Concept MapDocument1 pageBreast Cancer Concept MapKeepItSecret100% (1)
- Nursing Care PlanDocument3 pagesNursing Care PlanAnnahNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanJASMINE JOY BADUANo ratings yet
- Child - ImmunizationsDocument1 pageChild - ImmunizationsJOHN100% (1)
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- NCP & Drug Study (Tondo Med)Document5 pagesNCP & Drug Study (Tondo Med)Kevin_Remollo_2431No ratings yet
- Ov Ov OvDocument15 pagesOv Ov OvHayyana Mae Taguba LadiaNo ratings yet
- Request Letter For CHNDocument1 pageRequest Letter For CHNdusty kawiNo ratings yet
- Nursing Care Plan-1: Medical Diagnoses: Colorectal CancerDocument2 pagesNursing Care Plan-1: Medical Diagnoses: Colorectal CancerBheru LalNo ratings yet
- Impaired Tissue Integrity BurnDocument1 pageImpaired Tissue Integrity BurntabaloveNo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Pathways Nefrolithiasis Group 1Document1 pagePathways Nefrolithiasis Group 1Fuzna DahliaNo ratings yet
- Pa Tho Physiology of Pleural EffusionDocument1 pagePa Tho Physiology of Pleural EffusionventimiglionNo ratings yet
- Medical AsepsisDocument9 pagesMedical AsepsisSimran JosanNo ratings yet
- Nursing Theory: Betty Neuman's: By: Harpreet Kaur M.Sc. 1 YearDocument34 pagesNursing Theory: Betty Neuman's: By: Harpreet Kaur M.Sc. 1 YearSimran JosanNo ratings yet
- Orem'S Self-Care Deficit TheoryDocument52 pagesOrem'S Self-Care Deficit TheorySimran JosanNo ratings yet
- Curriculum FOR B.Sc. Nursing CourseDocument133 pagesCurriculum FOR B.Sc. Nursing Coursesimonjosan100% (1)
- FEVERDocument8 pagesFEVERSimran JosanNo ratings yet
- Course of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsDocument3 pagesCourse of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsSimran JosanNo ratings yet
- Cardiac Surgery and InvestigationDocument30 pagesCardiac Surgery and InvestigationSimran JosanNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument6 pagesCyanotic Congenital Heart DiseaseSimran JosanNo ratings yet
- Cardiac Invasive Diagnostic Tests GuideDocument19 pagesCardiac Invasive Diagnostic Tests GuideSimran JosanNo ratings yet
- Complete FractureDocument10 pagesComplete FractureSimran JosanNo ratings yet
- Unit Plan MSC 1 FRST Year - Docx 22Document5 pagesUnit Plan MSC 1 FRST Year - Docx 22Simran JosanNo ratings yet
- Anatomy and Physiology of Colon of Case StudyDocument4 pagesAnatomy and Physiology of Colon of Case StudySimran JosanNo ratings yet
- Disease Condition... Diabetes MellitusDocument6 pagesDisease Condition... Diabetes MellitusSimran JosanNo ratings yet
- Anatomy and Physiology of Nervous SystemDocument13 pagesAnatomy and Physiology of Nervous SystemSimran JosanNo ratings yet
- Disease Condition of MastectomyDocument5 pagesDisease Condition of MastectomySimran JosanNo ratings yet
- Disease Condition of ColonDocument4 pagesDisease Condition of ColonSimran JosanNo ratings yet
- Disease Condition of MastectomyDocument5 pagesDisease Condition of MastectomySimran JosanNo ratings yet
- Single-Cell Map of Diverse Immune Phenotypes in The Breast Tumor MicroenvironmentDocument53 pagesSingle-Cell Map of Diverse Immune Phenotypes in The Breast Tumor MicroenvironmentRoger FigueiredoNo ratings yet
- Microbiology Flowchart Dr. NikitaDocument2 pagesMicrobiology Flowchart Dr. NikitaKshitij Singh RajputNo ratings yet
- Why SufferingDocument7 pagesWhy SufferingRandall Dean WestNo ratings yet
- Blood Lesson Planning and AssessmentDocument10 pagesBlood Lesson Planning and Assessmentapi-364329432No ratings yet
- Documentation On Medicinal Plants Sold I PDFDocument9 pagesDocumentation On Medicinal Plants Sold I PDFGbadeyanka O WuraolaNo ratings yet
- Brought Dead Protocol - RefDocument2 pagesBrought Dead Protocol - Refjesvin prathapNo ratings yet
- S2 Session 1Document3 pagesS2 Session 1s9419No ratings yet
- Oral and Maxillofacial PathologyDocument79 pagesOral and Maxillofacial PathologyMai AnhNo ratings yet
- Shea Dorsey CV 07-Apr-2023Document3 pagesShea Dorsey CV 07-Apr-2023api-668697374No ratings yet
- Hepatite B CoinfeçãoDocument31 pagesHepatite B Coinfeçãojefferson2392No ratings yet
- BSN 1-1 Biochem Week 6Document2 pagesBSN 1-1 Biochem Week 6PAULINE KAYE QUITANNo ratings yet
- CLINPR 100331 Edit ReportDocument8 pagesCLINPR 100331 Edit Reportjohnysalem88No ratings yet
- 0610 w04 QP 1Document16 pages0610 w04 QP 1Vipin DasNo ratings yet
- Research Paper On Brassica RapaDocument8 pagesResearch Paper On Brassica Rapangqcodbkf100% (1)
- Operating Manual Electronic Column Scale M20610Document8 pagesOperating Manual Electronic Column Scale M20610Bryan GarciaNo ratings yet
- Midwifery MGT L5Document77 pagesMidwifery MGT L5MaxNo ratings yet
- Colon cancer screening recommendations and barriersDocument7 pagesColon cancer screening recommendations and barriersKen Ancheta LagayadaNo ratings yet
- Six Tiered HMDocument21 pagesSix Tiered HMDoctors NewsNo ratings yet
- Gujarat Council On Science and Technology, GandhianagarDocument42 pagesGujarat Council On Science and Technology, GandhianagarMergu Bala RajuNo ratings yet
- Neuromuscular Disorders in Geriatric PatientsDocument16 pagesNeuromuscular Disorders in Geriatric PatientsAhmed NasrNo ratings yet
- Mesenteric Venous Thrombosis NejmDocument6 pagesMesenteric Venous Thrombosis NejmJUAN LUIS PASAPERANo ratings yet
- Journal Club: DR Meera Nandan 3 Year MD ClinicalyogaDocument54 pagesJournal Club: DR Meera Nandan 3 Year MD ClinicalyogaMeera NandanNo ratings yet
- I. LISTENING (5 Points)Document16 pagesI. LISTENING (5 Points)Nhật TiếnNo ratings yet
- Workshop1 1Document2 pagesWorkshop1 1Aple Mae Cudiamat Letranca-CastroNo ratings yet
- Red Flags ArticleDocument4 pagesRed Flags ArticleINNOCENT KHULIWANo ratings yet
- Disusun Untuk Memenuhi Sebagian Syarat Kepaniteraan Klinik Dibagian Ilmu Penyakit Anak RSUD MuntilanDocument3 pagesDisusun Untuk Memenuhi Sebagian Syarat Kepaniteraan Klinik Dibagian Ilmu Penyakit Anak RSUD MuntilanAdistha TofanoNo ratings yet