You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Vaccine Friendly PlanDocument4 pagesVaccine Friendly PlanAna Sampaio89% (9)
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Rating: 5 out of 5 stars5/5 (1)
- MeningitisDocument9 pagesMeningitisNader Smadi88% (8)
- Pediatric Infectious Disease - A Practically Painless Review (2015)Document213 pagesPediatric Infectious Disease - A Practically Painless Review (2015)Fajrin Ashari100% (2)
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioNo ratings yet
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfNo ratings yet
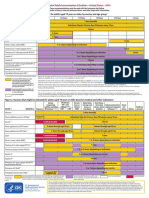
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- Adult Schedule 11x17Document2 pagesAdult Schedule 11x17lcmurilloNo ratings yet
- Vacunas 2012Document7 pagesVacunas 2012dr.alexisleon9124No ratings yet
- States, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDocument7 pagesStates, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDolores KilpatrickNo ratings yet
- Adult Combined Schedule VaccineDocument33 pagesAdult Combined Schedule VaccinehatsuneNo ratings yet
- Adult Combined ScheduleDocument6 pagesAdult Combined ScheduleAstrid Elaine RosalesNo ratings yet
- Practice Changing UpDates - UpToDateDocument13 pagesPractice Changing UpDates - UpToDatemayteveronica1000No ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002No ratings yet
- ScheduleDocument2 pagesScheduleapi-286634335No ratings yet
- The Sinovac VaccineDocument4 pagesThe Sinovac VaccineMontasir BalambagNo ratings yet
- Vaccination Requirements and Form I-693: Mary Naughton, MD, MPHDocument55 pagesVaccination Requirements and Form I-693: Mary Naughton, MD, MPHErinaNo ratings yet
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDocument24 pagesImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahNo ratings yet
- COVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologyDocument10 pagesCOVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologydrToikNo ratings yet
- BIMA Oxford AZ Vaccine Detailed Position StatementDocument5 pagesBIMA Oxford AZ Vaccine Detailed Position StatementVegha NedyaNo ratings yet
- Recommended Immunizations FS enDocument2 pagesRecommended Immunizations FS enirfanmajeed1987No ratings yet
- 07 Childschd 6x4.5 1-Page PRDocument2 pages07 Childschd 6x4.5 1-Page PRSteluta GalbenusNo ratings yet
- MMWR HiB PDFDocument20 pagesMMWR HiB PDFworksheetbookNo ratings yet
- Current Presumptive Immunization SchedulesDocument4 pagesCurrent Presumptive Immunization SchedulesPedro Julian Tenorio ApesteguiNo ratings yet
- Clinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Document8 pagesClinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Hery PriyantoNo ratings yet
- Immunization Routine Table1Document9 pagesImmunization Routine Table1MeeKo VideñaNo ratings yet
- Protocolo CanadaDocument5 pagesProtocolo Canadashluly23No ratings yet
- iNMUNIZACIONES Adulto ACIP2022 aNNALSDocument14 pagesiNMUNIZACIONES Adulto ACIP2022 aNNALSEmilio Ulises Napoles LealNo ratings yet
- Complete Summary: Guideline TitleDocument30 pagesComplete Summary: Guideline TitleAlexandre MedeirosNo ratings yet
- WHO 2019 nCoV Vaccines SAGE Recommendation BIBP 2021.1 EngDocument7 pagesWHO 2019 nCoV Vaccines SAGE Recommendation BIBP 2021.1 EngDiane LigmanNo ratings yet
- Adult Immunization: It's Your Best Shot!Document40 pagesAdult Immunization: It's Your Best Shot!minerva_stanciuNo ratings yet
- InfuenzaDocument30 pagesInfuenzaChandra_INHU_RiauNo ratings yet
- Guidelines For Vaccination in Normal Adults in India - PMCDocument14 pagesGuidelines For Vaccination in Normal Adults in India - PMCSKMH INSURANCENo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years and Older)Document5 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years and Older)Hannah Caburian RemoNo ratings yet
- Human Papillomavirus Bivalent Vaccin1Document8 pagesHuman Papillomavirus Bivalent Vaccin1alejandro fernandezNo ratings yet
- Immunizaton During PregnancyDocument6 pagesImmunizaton During PregnancyMohamed SulimanNo ratings yet
- ImmunizationsDocument2 pagesImmunizationsSonny KusumaNo ratings yet
- Annex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleDocument175 pagesAnnex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleEfendi AnuarNo ratings yet
- Human Papillomavirus Vaccination For Adults: Updated Recommendations of The Advisory Committee On Immunization PracticesDocument5 pagesHuman Papillomavirus Vaccination For Adults: Updated Recommendations of The Advisory Committee On Immunization PracticesTiara RahmanandaNo ratings yet
- C Ovid Taskforce Update 11Document4 pagesC Ovid Taskforce Update 11Patricia FernándezNo ratings yet
- What's New On The Child and Adolescent Immunization SchedulesDocument30 pagesWhat's New On The Child and Adolescent Immunization SchedulesMark ReinhardtNo ratings yet
- Public FAQDocument15 pagesPublic FAQIan WeberNo ratings yet
- Antiviral Summary ClinicianDocument20 pagesAntiviral Summary ClinicianPurpleeyoreNo ratings yet
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDocument22 pages2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanNo ratings yet
- 2006 118 1774-1793 Subcommittee On Diagnosis and Management of BronchiolitisDocument22 pages2006 118 1774-1793 Subcommittee On Diagnosis and Management of BronchiolitisAlejandra Castro Salas エールNo ratings yet
- Annals of Medicine - HPV VaccineDocument12 pagesAnnals of Medicine - HPV VaccineJudicial Watch, Inc.100% (3)
- Guia de Vacunacion FelinaDocument5 pagesGuia de Vacunacion FelinaRaul KimNo ratings yet
- 2019 Guide For ImmunizationDocument195 pages2019 Guide For ImmunizationReigner paul DavidNo ratings yet
- Research Paper in English: Perception On COVID-19 Vaccines of Residents in Barangay Canlapwas, Pagsanghan SamarDocument10 pagesResearch Paper in English: Perception On COVID-19 Vaccines of Residents in Barangay Canlapwas, Pagsanghan SamarDivina CacheroNo ratings yet
- Antiviral Summary Clinicians InfluenzaDocument8 pagesAntiviral Summary Clinicians InfluenzaSylvia GonzalezNo ratings yet
- Hepatitis A Virus Infection - Treatment and Prevention - UpToDateDocument31 pagesHepatitis A Virus Infection - Treatment and Prevention - UpToDateGabrielle AndersonNo ratings yet
- Guidelines For The Use of Antiretroviral Agents in HIV-1-Infected Adults and AdolescentsDocument48 pagesGuidelines For The Use of Antiretroviral Agents in HIV-1-Infected Adults and AdolescentsAgus OrtNo ratings yet
- Recommended Childhood and Adolescent Immunization Schedule: United States, 2020Document5 pagesRecommended Childhood and Adolescent Immunization Schedule: United States, 2020nanaNo ratings yet
- Can You Outline in A Few Sentences What Gardasil Does? and Why It Is Administered To 13 Year Olds?Document6 pagesCan You Outline in A Few Sentences What Gardasil Does? and Why It Is Administered To 13 Year Olds?api-249115191No ratings yet
- Guideline of ARV in Adult and Adolescents - Tables OnlyDocument132 pagesGuideline of ARV in Adult and Adolescents - Tables OnlyAlvi MuldaniNo ratings yet
- AA Tables PDFDocument133 pagesAA Tables PDFRafaelNo ratings yet
- Diagnosis/vaccination/: Hepatitis B VaccineDocument6 pagesDiagnosis/vaccination/: Hepatitis B Vaccinereza satriaNo ratings yet
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- PHE Complete Immunisation Schedule Jan2020 PDFDocument2 pagesPHE Complete Immunisation Schedule Jan2020 PDFJyotirmaya RajaNo ratings yet
- Sanofi 2015Document109 pagesSanofi 2015Abdulwahab AfridiNo ratings yet
- Neurologic Emergencies 2 MergedDocument71 pagesNeurologic Emergencies 2 MergedDanica FrancoNo ratings yet
- Immunization RecordDocument52 pagesImmunization RecordkonrajNo ratings yet
- Novartis Annual Report 2009Document268 pagesNovartis Annual Report 2009Santiago CuetoNo ratings yet
- Jonah Vaccine ProgramDocument40 pagesJonah Vaccine ProgramEdwin MagnoNo ratings yet
- Vaccines With Diluents How To Use ThemDocument1 pageVaccines With Diluents How To Use ThemMoinNo ratings yet
- Meningitis Bacteriana Aguda en El AdultoDocument12 pagesMeningitis Bacteriana Aguda en El AdultoJulian AlbarracínNo ratings yet
- Lecture 40-Travel MedicineDocument44 pagesLecture 40-Travel MedicineEsther Meyline XhypaNo ratings yet
- SHC Asplenia Vaccine Guide 11-8-18 RevisionDocument4 pagesSHC Asplenia Vaccine Guide 11-8-18 RevisionEl LenNo ratings yet
- What Is Meningitis?Document7 pagesWhat Is Meningitis?laujeroNo ratings yet
- Vaccination SchedDocument9 pagesVaccination SchedDaihachi DaimeNo ratings yet
- Travel Medicine: Health Quarantine 2021 Dr. Esther Meylina SipahutarDocument35 pagesTravel Medicine: Health Quarantine 2021 Dr. Esther Meylina SipahutarEsther Meyline XhypaNo ratings yet
- Meningococcal Disease: What College Communities Need To KnowDocument2 pagesMeningococcal Disease: What College Communities Need To KnowSinclair Broadcast Group - EugeneNo ratings yet
- Childhood Immunization Schedule 2021 EditedDocument11 pagesChildhood Immunization Schedule 2021 EditedPatricia Bernadette PalenciaNo ratings yet
- GSK Annual Report 2020Document244 pagesGSK Annual Report 2020S1626No ratings yet
- Meningococcal Meningitis - DR Ooi Phaik YeeDocument66 pagesMeningococcal Meningitis - DR Ooi Phaik YeeNg Chee KeongNo ratings yet
- Management of Pediatric Community-Acquired Bacterial PneumoniaDocument84 pagesManagement of Pediatric Community-Acquired Bacterial PneumoniaShahid Khan GhouriNo ratings yet
- St. Paul College of Ilocos SurDocument6 pagesSt. Paul College of Ilocos SurMarie Kelsey Acena Macaraig100% (1)
- VAKSINDocument29 pagesVAKSINLeonardo LiswojoNo ratings yet
- Immunization, Vaccines and Biologicals IVB Catalogue 2017: 13 January 2017Document83 pagesImmunization, Vaccines and Biologicals IVB Catalogue 2017: 13 January 2017pradip_26No ratings yet
- Amy Pharma ClaimesDocument8 pagesAmy Pharma ClaimesVishwas BijjahalliNo ratings yet
- Immunization Training GuideDocument91 pagesImmunization Training Guidezenagit123456100% (1)
- USC Immunization Checklist FormDocument2 pagesUSC Immunization Checklist FormbuiiiilderNo ratings yet
- Epi and ImmunizationsDocument66 pagesEpi and ImmunizationsreadmeamllionNo ratings yet
- Prep 2016Document864 pagesPrep 2016pkpowerhouse100% (3)
- LIST OF REGISTERED DRUGS As of December 2012Document52 pagesLIST OF REGISTERED DRUGS As of December 2012Benjamin TantiansuNo ratings yet