You might also like
- All The Words I Should Have Said - Rania NaimDocument167 pagesAll The Words I Should Have Said - Rania NaimNan Nan100% (2)
- Fixed Prosthodontics in Dental PracticeFrom EverandFixed Prosthodontics in Dental PracticeRating: 4 out of 5 stars4/5 (1)
- PokeDex ChecklistDocument7 pagesPokeDex ChecklistJosh StrıkeNo ratings yet
- Microtensile Bond Strength To Enamel Affected by Hypoplastic AmelogenesiDocument9 pagesMicrotensile Bond Strength To Enamel Affected by Hypoplastic AmelogenesiPablo BenitezNo ratings yet
- 5.pulpotomy Medicaments Used in Deciduous Dentition An UpdateDocument18 pages5.pulpotomy Medicaments Used in Deciduous Dentition An UpdateRahma IskNo ratings yet
- Provided by HKU Scholars HubDocument27 pagesProvided by HKU Scholars HubRavudai JabbalNo ratings yet
- Adhesion To Enamel of Teeth Affected by Molar Incisor Hypomineralization: Literature ReviewDocument7 pagesAdhesion To Enamel of Teeth Affected by Molar Incisor Hypomineralization: Literature ReviewanonimoNo ratings yet
- Comparison of Deproteinization Agents On BondingDocument8 pagesComparison of Deproteinization Agents On BondingpyrockerNo ratings yet
- Discoloration Potential of Endodontic Sealers: A Brief ReviewDocument5 pagesDiscoloration Potential of Endodontic Sealers: A Brief ReviewzaheerbdsNo ratings yet
- GRUPO 4 HIM-Caries Americano 2017Document11 pagesGRUPO 4 HIM-Caries Americano 2017Vanessa MinNo ratings yet
- Biomimetic Tooth Repair, Amelogenin-Derived Peptide Enables in Vitro Remineralization of Human EnamelDocument9 pagesBiomimetic Tooth Repair, Amelogenin-Derived Peptide Enables in Vitro Remineralization of Human Enamelzubair ahmedNo ratings yet
- Evaluation of Bond Strength of Acrylic Teeth To Denture BaseDocument3 pagesEvaluation of Bond Strength of Acrylic Teeth To Denture Basealestrada12345No ratings yet
- Archives of Oral Biology: ReviewDocument10 pagesArchives of Oral Biology: ReviewEDER YAHIR MONROY MENDOZANo ratings yet
- Classification Review of Dental Adhesives Systems From The IV Generation To The Universal TypeDocument17 pagesClassification Review of Dental Adhesives Systems From The IV Generation To The Universal TypeJoshua ValdezNo ratings yet
- 20 TH JC - SindhuDocument9 pages20 TH JC - SindhuDadi SindhuNo ratings yet
- Classification Review of Dental Adhesive Systems: From The IV Generation To The Universal TypeDocument17 pagesClassification Review of Dental Adhesive Systems: From The IV Generation To The Universal Typejuan diegoNo ratings yet
- Adhesivos UniversalesDocument9 pagesAdhesivos Universalesmaria posadaNo ratings yet
- Rio SDocument12 pagesRio SErni ErawatiNo ratings yet
- The Up To 21-Year Clinical Outcome and Survival of Feldspathic Porcelain Veneers: Accounting For ClusteringDocument9 pagesThe Up To 21-Year Clinical Outcome and Survival of Feldspathic Porcelain Veneers: Accounting For ClusteringAlexander L. Contreras PairaNo ratings yet
- Bioestadistica PDFDocument8 pagesBioestadistica PDFkevinNo ratings yet
- Amelogenesis Imperfecta: Case Study: Operative Dentistry September 2017Document14 pagesAmelogenesis Imperfecta: Case Study: Operative Dentistry September 2017Barbulescu Anca DianaNo ratings yet
- N Vitro Wear of Resin-Based Materials-: Simultaneous Corrosive and Abrasive WearDocument7 pagesN Vitro Wear of Resin-Based Materials-: Simultaneous Corrosive and Abrasive Wearu1azadNo ratings yet
- Ferraris Et Al IJED PIAR ARG 2 20212Document24 pagesFerraris Et Al IJED PIAR ARG 2 20212khaled emadNo ratings yet
- A Case Report of Enamel Hypoplasia: Alka Hazari, Rana K Varghese, Aditya Mitra, Nivedita V BajantriDocument4 pagesA Case Report of Enamel Hypoplasia: Alka Hazari, Rana K Varghese, Aditya Mitra, Nivedita V BajantriRuxandra FitaNo ratings yet
- Posterior Composite Restoration UpdateDocument10 pagesPosterior Composite Restoration UpdateBianca IovoaiaNo ratings yet
- Restorative Materials Used in Pediatric DentistryDocument6 pagesRestorative Materials Used in Pediatric DentistryS100% (2)
- 1 s2.0 S1991790215000550 MainDocument7 pages1 s2.0 S1991790215000550 MainOrtodoncia 1No ratings yet
- Jos 10 17Document7 pagesJos 10 17Thibaut BossuytNo ratings yet
- Australian Dental Journal - 2009 - Abbott - Internal Bleaching of Teeth An Analysis of 255 TeethDocument8 pagesAustralian Dental Journal - 2009 - Abbott - Internal Bleaching of Teeth An Analysis of 255 Teethnafsiyah xyzNo ratings yet
- Acondicionamiento, Adhesión y Cementado de Aparatología Ortodóncica en Dientes Con Alteraciones Del Esmalte. Revisión de LiteraturaDocument10 pagesAcondicionamiento, Adhesión y Cementado de Aparatología Ortodóncica en Dientes Con Alteraciones Del Esmalte. Revisión de Literaturaruqoyah022No ratings yet
- Estudio de Bondeado de BracketDocument4 pagesEstudio de Bondeado de BracketWilliam Alexander Bocanegra AcostaNo ratings yet
- Obturating Materials Used For Pulpectomy in Primary Teeth A ReviewDocument9 pagesObturating Materials Used For Pulpectomy in Primary Teeth A ReviewMohammed SaeedNo ratings yet
- Outcome of Bonded Vs All-Ceramic and PDFDocument21 pagesOutcome of Bonded Vs All-Ceramic and PDFsalshabilaNo ratings yet
- Aapd Guidelines - Restorative Dentistry PDFDocument8 pagesAapd Guidelines - Restorative Dentistry PDFMaqbul AlamNo ratings yet
- Treatment Decisions On Molar-Incisor HypomineralizDocument8 pagesTreatment Decisions On Molar-Incisor HypomineralizAlvaro ChacónNo ratings yet
- Adhesion of Multimode Adhesives To Enamel and Dentin 2017Document9 pagesAdhesion of Multimode Adhesives To Enamel and Dentin 2017Paul AlvarezNo ratings yet
- Tooth Wear Against Ceramic Crowns in Posterior RegDocument9 pagesTooth Wear Against Ceramic Crowns in Posterior RegPremshith CpNo ratings yet
- Homsy Et Al-2015-Journal of Prosthodontics PDFDocument7 pagesHomsy Et Al-2015-Journal of Prosthodontics PDFdanaNo ratings yet
- Self EtchingDocument16 pagesSelf EtchingHawzhen Masoud Mohammed SaeedNo ratings yet
- Investigating The Antimicrobial Activity of Different Root Canal Filling Pastes in Deciduous TeethDocument7 pagesInvestigating The Antimicrobial Activity of Different Root Canal Filling Pastes in Deciduous Teethanindya permatasyafiraNo ratings yet
- Shear Bond Strength of Orthodontic Brackets Bonded With Different Self-Etching AdhesivesDocument6 pagesShear Bond Strength of Orthodontic Brackets Bonded With Different Self-Etching AdhesivesKatia ValNo ratings yet
- Carillas de Porcelana - Nitesh Shetty - Savita Dandakeri - Shilpa DandekeriDocument5 pagesCarillas de Porcelana - Nitesh Shetty - Savita Dandakeri - Shilpa DandekeriJony OcañaNo ratings yet
- ResilonDocument33 pagesResilonhasNo ratings yet
- Adhesion in Restorative Dentistry 2016Document41 pagesAdhesion in Restorative Dentistry 2016mishNo ratings yet
- DesmineralizanteDocument7 pagesDesmineralizanteHolman FuyaNo ratings yet
- ProfessionalDocument6 pagesProfessionalhbusyNo ratings yet
- 15 PDFDocument4 pages15 PDFSanjeev AthiberanNo ratings yet
- Analysis of Enamel Rod End Pattern For Personal IdentificationDocument6 pagesAnalysis of Enamel Rod End Pattern For Personal IdentificationNaneunBaboNo ratings yet
- Assessment of Clinical Success of Three Sealants: Embrace-Wetbond, Clinpro, and Helioseal-F in Permanent Molars: An in Vivo StudyDocument7 pagesAssessment of Clinical Success of Three Sealants: Embrace-Wetbond, Clinpro, and Helioseal-F in Permanent Molars: An in Vivo StudyABNo ratings yet
- DT Oct 13 NPR Milnar Fnl1Document9 pagesDT Oct 13 NPR Milnar Fnl1Kranti PrajapatiNo ratings yet
- Adj 12682Document15 pagesAdj 12682pradnja surya paramithaNo ratings yet
- Obturating Materials in Pediatric Dentistry A ReviDocument9 pagesObturating Materials in Pediatric Dentistry A Revikathuriayug5No ratings yet
- Case Report: Aesthetic and Functional Rehabilitation of The Primary Dentition Affected by Amelogenesis ImperfectaDocument7 pagesCase Report: Aesthetic and Functional Rehabilitation of The Primary Dentition Affected by Amelogenesis ImperfectaPo PowNo ratings yet
- Guideline On Pediatric Restorative Dentistry: Originating Committee Review Council Adopted RevisedDocument7 pagesGuideline On Pediatric Restorative Dentistry: Originating Committee Review Council Adopted RevisedEduardo SánchezNo ratings yet
- Microfiltracion en CarillasDocument6 pagesMicrofiltracion en CarillasCdjuan GnNo ratings yet
- Promotion of Dental Pulp Wound Healing in New Zealand White Rabbits' Teeth by Thai Propolis ProductDocument8 pagesPromotion of Dental Pulp Wound Healing in New Zealand White Rabbits' Teeth by Thai Propolis ProductLuidi MarquesNo ratings yet
- Restoration of Root Canal Treated Teeth With Direct Composite Onlays: A Prospective Clinical StudyDocument3 pagesRestoration of Root Canal Treated Teeth With Direct Composite Onlays: A Prospective Clinical StudydeaNo ratings yet
- Nanohydroxyapatite and ChitosanDocument10 pagesNanohydroxyapatite and ChitosanRania HanafyNo ratings yet
- Crombie2009, Aetiology of Molar-Incisor Hypomineralization A Critical ReviewDocument11 pagesCrombie2009, Aetiology of Molar-Incisor Hypomineralization A Critical ReviewMairen RamirezNo ratings yet
- Enamel Hypoplasia RestorationDocument4 pagesEnamel Hypoplasia RestorationzaheerbdsNo ratings yet
- F. D.D.S.," L. MS."" W. D.Sc. : Retentive Properties of Dental CementsDocument9 pagesF. D.D.S.," L. MS."" W. D.Sc. : Retentive Properties of Dental CementsSaad LiaqatNo ratings yet
- 4 BaDocument18 pages4 BaSaad LiaqatNo ratings yet
- A Review of Conventional and Contemporary Luting Agents Used in DentistryDocument8 pagesA Review of Conventional and Contemporary Luting Agents Used in DentistryAnand KasiNo ratings yet
- 1 C PDFDocument9 pages1 C PDFSaad LiaqatNo ratings yet
- Maroulakos 2019Document12 pagesMaroulakos 2019Luis Alberto Carpio MorenoNo ratings yet
- Characterization and Analyses of Acid-Extractable and Leached Trace Elements in Dental CementsDocument7 pagesCharacterization and Analyses of Acid-Extractable and Leached Trace Elements in Dental CementsSaad LiaqatNo ratings yet
- A Review of Dental Cements: Kipp Wingo, DVM, DAVDCDocument10 pagesA Review of Dental Cements: Kipp Wingo, DVM, DAVDCSaad LiaqatNo ratings yet
- F. D.D.S.," L. MS."" W. D.Sc. : Retentive Properties of Dental CementsDocument9 pagesF. D.D.S.," L. MS."" W. D.Sc. : Retentive Properties of Dental CementsSaad LiaqatNo ratings yet
- Bahan 1 PDFDocument6 pagesBahan 1 PDFNabilah NazalikaNo ratings yet
- Dental Casting of Titanium and Ni-Ti Alloys by Casting MachineDocument5 pagesDental Casting of Titanium and Ni-Ti Alloys by Casting MachineSaad LiaqatNo ratings yet
- Surface Characterization of Passive Film On Nicr-Based Dental Casting AlloysDocument8 pagesSurface Characterization of Passive Film On Nicr-Based Dental Casting AlloysSaad LiaqatNo ratings yet
- Advances in Dental Research: Review of Dental Impression MaterialsDocument15 pagesAdvances in Dental Research: Review of Dental Impression MaterialsSaad LiaqatNo ratings yet
- Skupien2015 Factores Asociados Con La Retencion Del PosteDocument8 pagesSkupien2015 Factores Asociados Con La Retencion Del PosteAmparo AnayaNo ratings yet
- 8 DC PDFDocument6 pages8 DC PDFSaad LiaqatNo ratings yet
- 4 DCDocument13 pages4 DCSaad LiaqatNo ratings yet
- Artifacts From Dental Casting Alloys in Magnetic Resonance ImagingDocument5 pagesArtifacts From Dental Casting Alloys in Magnetic Resonance ImagingSaad LiaqatNo ratings yet
- Experimental Microleakage Around Ageing Dental Amalgam Restorations: A ReviewDocument11 pagesExperimental Microleakage Around Ageing Dental Amalgam Restorations: A ReviewSaad LiaqatNo ratings yet
- 3 Da PDFDocument14 pages3 Da PDFSaad LiaqatNo ratings yet
- 21 CoDocument26 pages21 CoSaad LiaqatNo ratings yet
- The Use of Mercury in Dentistry: A Critical Review of The Recent LiteratureDocument14 pagesThe Use of Mercury in Dentistry: A Critical Review of The Recent LiteratureSaad LiaqatNo ratings yet
- Biocompatibility of Dental Casting Alloys: A ReviewDocument12 pagesBiocompatibility of Dental Casting Alloys: A ReviewSaad LiaqatNo ratings yet
- 1 Da PDFDocument8 pages1 Da PDFSaad LiaqatNo ratings yet
- 6 Da PDFDocument11 pages6 Da PDFSaad LiaqatNo ratings yet
- Bond Strength of Universal Adhesives: A Systematic Review and Meta-AnalysisDocument12 pagesBond Strength of Universal Adhesives: A Systematic Review and Meta-AnalysisPablo BenitezNo ratings yet
- 14 CoDocument9 pages14 CoSaad LiaqatNo ratings yet
- 17 Co PDFDocument25 pages17 Co PDFSaad LiaqatNo ratings yet
- 19 Co PDFDocument15 pages19 Co PDFSaad LiaqatNo ratings yet
- 4 BaDocument18 pages4 BaSaad LiaqatNo ratings yet
- 15 CoDocument9 pages15 CoSaad LiaqatNo ratings yet
- 16 CoDocument9 pages16 CoSaad LiaqatNo ratings yet
- TITLE: ONBOARDING-Make Better The Experience of New Hire Executive Summary Onboarding, Also Known As Organizational Socialization, Refers To TheDocument3 pagesTITLE: ONBOARDING-Make Better The Experience of New Hire Executive Summary Onboarding, Also Known As Organizational Socialization, Refers To ThePavel BawaNo ratings yet
- Sogc AssignmentDocument2 pagesSogc Assignmentapi-573219210No ratings yet
- Crystal Report Viewer 1Document2 pagesCrystal Report Viewer 1David Lemayian SalatonNo ratings yet
- Chap 3Document40 pagesChap 3eshbliNo ratings yet
- CCINFMJ Passlist - 05082022Document2 pagesCCINFMJ Passlist - 05082022Kamlakar SadavarteNo ratings yet
- To FrameDocument5 pagesTo FrameMuhaimin RohizanNo ratings yet
- ISO 90012015checklist - tcm14 57745 PDFDocument25 pagesISO 90012015checklist - tcm14 57745 PDFDaniela Muñoz SaldiasNo ratings yet
- Modern Steel Construction March-2022Document76 pagesModern Steel Construction March-2022jackcan501No ratings yet
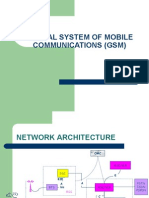
- GSMDocument38 pagesGSMapi-370641475% (8)
- Ascend P7: Huawei SchematicDocument51 pagesAscend P7: Huawei SchematicCarlos Andres EscamillaNo ratings yet
- The Good Governance Concept Revisited PDFDocument16 pagesThe Good Governance Concept Revisited PDFPritam AnantaNo ratings yet
- Kidstone Mines Start UpDocument5 pagesKidstone Mines Start UpCraftychemistNo ratings yet
- Change Pattern 1 To Pattern 2 by Moving Only Three Counters, Each Counter OnceDocument14 pagesChange Pattern 1 To Pattern 2 by Moving Only Three Counters, Each Counter OnceReshmiNo ratings yet
- Assignment 2 MKT 411Document3 pagesAssignment 2 MKT 411Farhad HossainNo ratings yet
- Life Cycle Asset ManagementDocument1 pageLife Cycle Asset ManagementJuan EspinosaNo ratings yet
- Ces511 - Structural Engineering Laboratory Lab Experiment: Bending Moment and Shear Force in Beams (Co2:Po5)Document13 pagesCes511 - Structural Engineering Laboratory Lab Experiment: Bending Moment and Shear Force in Beams (Co2:Po5)elhammeNo ratings yet
- M16a3 Upper SpecsDocument1 pageM16a3 Upper SpecsMosinNo ratings yet
- 6 Bhel - Noida ElectricalDocument9 pages6 Bhel - Noida Electricaldeepti sharmaNo ratings yet
- Constructionandmaintenanceof Riverembankments (Levees) - GuidelinesDocument7 pagesConstructionandmaintenanceof Riverembankments (Levees) - GuidelinesSushil DhunganaNo ratings yet
- Introducing The Open Banking StandardDocument12 pagesIntroducing The Open Banking StandardOpen Data Institute96% (25)
- BrusselsDocument1 pageBrusselskmiqdNo ratings yet
- Synopsis Format-Practice SchoolDocument4 pagesSynopsis Format-Practice SchoolArjun GoyalNo ratings yet
- Impact On OrganizationsDocument14 pagesImpact On OrganizationsogakhanNo ratings yet
- Max-E2/841™ Family Nema Premium Efficiency: Type Aehh8B, Aehh8Bcf, Aeuh8BdcDocument1 pageMax-E2/841™ Family Nema Premium Efficiency: Type Aehh8B, Aehh8Bcf, Aeuh8BdcAnibal QuezadaNo ratings yet
- Shiksha Sopan April 09Document4 pagesShiksha Sopan April 09Amrendra NarayanNo ratings yet
- M Pump - Plunger 300Document30 pagesM Pump - Plunger 300hebert perezNo ratings yet
- Ok - Las-Q2 Oral - Com W1Document5 pagesOk - Las-Q2 Oral - Com W1Ruben Rosendal De AsisNo ratings yet
- Sport Obermeyer PaperDocument10 pagesSport Obermeyer PaperagarwalankurkNo ratings yet