You might also like
- Nursing Care PlanDocument9 pagesNursing Care PlanLura Xstilice B. Galinato100% (1)
- Gastroenterology FlashcardsDocument12 pagesGastroenterology FlashcardsRodrigo FonsecaNo ratings yet
- Bowels Open 6 Times Per 24 Hours: Document ControlDocument7 pagesBowels Open 6 Times Per 24 Hours: Document ControlKeith PohlNo ratings yet
- Palliative care-MBODocument17 pagesPalliative care-MBOChonnikan LimpongsanurukNo ratings yet
- Diagnostic and Prevention Approach in Post Endoscopic Retrograde Cholangiopancreatography PancreatitisDocument6 pagesDiagnostic and Prevention Approach in Post Endoscopic Retrograde Cholangiopancreatography PancreatitisAnonymous hF9HwHVuqNo ratings yet
- Acute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenDocument25 pagesAcute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenLuqman Arif Ahmad HazriNo ratings yet
- Acute Pancreatitis: ManagementDocument11 pagesAcute Pancreatitis: ManagementKakhaNo ratings yet
- Pancreatitis Aguda: Erik Rauch Sánchez Médico Gastroenterólogo Febrero 2016. / 999 290 697Document30 pagesPancreatitis Aguda: Erik Rauch Sánchez Médico Gastroenterólogo Febrero 2016. / 999 290 697NickNo ratings yet
- Acute PancreatitisDocument66 pagesAcute PancreatitisSamina GulNo ratings yet
- Inflammatory Colitis - A RecapDocument34 pagesInflammatory Colitis - A RecapanahitaasharmaNo ratings yet
- 2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportDocument4 pages2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportHany ElbarougyNo ratings yet
- Acute Pancreatitis: Dr. Ali Raza Dr. Talha Javed CHDocument31 pagesAcute Pancreatitis: Dr. Ali Raza Dr. Talha Javed CHahmad frazNo ratings yet
- Oncologic EmergenciespaghubasanDocument10 pagesOncologic EmergenciespaghubasanRoyce Vincent TizonNo ratings yet
- 6 Day Pediatric PancreatitisDocument16 pages6 Day Pediatric PancreatitisShreyash HaritwalNo ratings yet
- Management of Acute PancreatitisDocument31 pagesManagement of Acute PancreatitisLance sorianoNo ratings yet
- Acute Pancreatitis: Presented By: DAHAL SHIRISHADocument25 pagesAcute Pancreatitis: Presented By: DAHAL SHIRISHASiruNo ratings yet
- Cholecystitis and CholelithiasisDocument19 pagesCholecystitis and CholelithiasisChristine Salimbagat100% (1)
- Ten Tips To Manage Severe Acute Pancreatitis in An Intensive Care UnitDocument4 pagesTen Tips To Manage Severe Acute Pancreatitis in An Intensive Care UnitRicardo Victor PereiraNo ratings yet
- Acute Pancreatitis: Methas Arunnart MD. Songkhla HospitalDocument70 pagesAcute Pancreatitis: Methas Arunnart MD. Songkhla HospitalMohd ImranNo ratings yet
- Acute PancreatitisDocument40 pagesAcute PancreatitisAbdulsalam DostNo ratings yet
- GentDocument2 pagesGentOxford666No ratings yet
- Postendoscopic Retrograde Cholangiopancreatography PancreatitisDocument7 pagesPostendoscopic Retrograde Cholangiopancreatography PancreatitisErnest Ang GrekNo ratings yet
- Acute PancreatitisDocument9 pagesAcute PancreatitisestefygomezsNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- Ascites, SBP, Encephlopathy 2Document78 pagesAscites, SBP, Encephlopathy 2Rida AkramNo ratings yet
- Chauke NJ 201908564 NUTRITIONAL SCREENINGDocument7 pagesChauke NJ 201908564 NUTRITIONAL SCREENINGRulani PrinceNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Severe Pancreatitis: Yoshiaki Uda ICU Registrar Teaching 26/5/2010Document22 pagesSevere Pancreatitis: Yoshiaki Uda ICU Registrar Teaching 26/5/2010yoshiudaNo ratings yet
- Acute Colonic Pseudo-ObstructionDocument4 pagesAcute Colonic Pseudo-ObstructionJosé Luis Navarro Romero100% (1)
- Chronic Pancreatitis: DefinitionDocument4 pagesChronic Pancreatitis: DefinitionDrVishwa PrakashNo ratings yet
- Understanding Medical Surgical Nursing - 0841-0841Document1 pageUnderstanding Medical Surgical Nursing - 0841-0841Anas TasyaNo ratings yet
- Poisoning 2Document5 pagesPoisoning 2Lily AddamsNo ratings yet
- Chronic PancreatitisDocument3 pagesChronic PancreatitisCharry AlupiasNo ratings yet
- Acute Pancreatitis, Hepatitis, Liver Cirrhosis: Ma Eileen O Pascua, MD, FPCP, FPSG, FpsdeDocument24 pagesAcute Pancreatitis, Hepatitis, Liver Cirrhosis: Ma Eileen O Pascua, MD, FPCP, FPSG, FpsdePrincess Noreen SavellanoNo ratings yet
- Guideline PancreatitisDocument39 pagesGuideline Pancreatitisanda_No ratings yet
- Acute Pancreatitis: Department of Critical Care Medicine King Saud Medical City Riyadh, Saudi ArabiaDocument29 pagesAcute Pancreatitis: Department of Critical Care Medicine King Saud Medical City Riyadh, Saudi ArabiaONe's IwanNo ratings yet
- Nefrologi: I Gusti Ngurah Agung Tresna ErawanDocument69 pagesNefrologi: I Gusti Ngurah Agung Tresna ErawanDian PritaNo ratings yet
- University of Maryland Medical Center Fluconazole (Diflucan®)Document6 pagesUniversity of Maryland Medical Center Fluconazole (Diflucan®)damondouglasNo ratings yet
- Xi - Drug Study: Drugs Action Indication Contraindication Adverse Effect Nursing ConsiderationDocument18 pagesXi - Drug Study: Drugs Action Indication Contraindication Adverse Effect Nursing ConsiderationlicservernoidaNo ratings yet
- Chronic PancreatitisDocument42 pagesChronic PancreatitismmurugeshrajNo ratings yet
- Atezolizumab-FDA LabelDocument38 pagesAtezolizumab-FDA LabelClarissa BCNo ratings yet
- Daptomycin (Cubicin)Document1 pageDaptomycin (Cubicin)Adrianne BazoNo ratings yet
- Pancreatiti S Aguda: Catedra: Docente: EstudianteDocument35 pagesPancreatiti S Aguda: Catedra: Docente: EstudianteMaybelline Ruiz ReyesNo ratings yet
- Js - Case PresentationDocument61 pagesJs - Case Presentationapi-592676308No ratings yet
- Maham PrsentationDocument28 pagesMaham PrsentationAlbern ArifNo ratings yet
- DiverticulitaDocument6 pagesDiverticulitaoxichinolinNo ratings yet
- PancreatitisDocument3 pagesPancreatitisTarran PhagooNo ratings yet
- Clinical ManagementDocument10 pagesClinical Managementpruebaprueba321765No ratings yet
- Clinical Liver Disease - 2012 - Reverter - Management of An Acute Variceal Bleeding EpisodeDocument4 pagesClinical Liver Disease - 2012 - Reverter - Management of An Acute Variceal Bleeding EpisodeEUODIA HANA KRISTINANo ratings yet
- DIARRHEADocument12 pagesDIARRHEAtintin srgpnNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Pediatric Acute Sepsis: Physician'S OrdersDocument4 pagesPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNo ratings yet
- American College of Gastroenterology Guideline .6Document16 pagesAmerican College of Gastroenterology Guideline .6Javier CubillosNo ratings yet
- PANCREATITISDocument38 pagesPANCREATITISVEDHIKAVIJAYANNo ratings yet
- Acute PancreatitisDocument6 pagesAcute PancreatitisErudite WhaleNo ratings yet
- Perioperative Anesthetic Management of Intestinal Pseudo-Obstruction As A Complication of PheochromocytomaDocument4 pagesPerioperative Anesthetic Management of Intestinal Pseudo-Obstruction As A Complication of Pheochromocytomaceneh5695weizixu.com xNo ratings yet
- 2013 - ACG - Management of Acute PancreatitisDocument16 pages2013 - ACG - Management of Acute PancreatitismohamedelsayedelmenyawyNo ratings yet
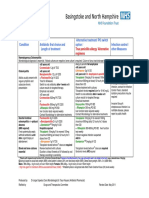
- Bone and Joint Infections BNHFT 2010 PDFDocument3 pagesBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriNo ratings yet
- PA - Gastroenterology - 2013 - Jun - 144 (6) - 1272Document10 pagesPA - Gastroenterology - 2013 - Jun - 144 (6) - 1272Lourianne NcNo ratings yet
- Critical Care NutritionDocument64 pagesCritical Care NutritionGeront AndrewsNo ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
- 6.1. Stool Specimen 6.1. Stool Specimen: 9/18/21 Tafeseb - Tufa 1Document67 pages6.1. Stool Specimen 6.1. Stool Specimen: 9/18/21 Tafeseb - Tufa 1Worku KifleNo ratings yet
- Vitamins: Organic Compounds Required in Minute Quantities Specific Body FunctionsDocument57 pagesVitamins: Organic Compounds Required in Minute Quantities Specific Body FunctionsWorku KifleNo ratings yet
- Small Intestine MMCDocument65 pagesSmall Intestine MMCWorku KifleNo ratings yet
- Lower Limb Fracture..MeDocument142 pagesLower Limb Fracture..MeWorku KifleNo ratings yet
- LaPlace's LawDocument2 pagesLaPlace's LawWorku KifleNo ratings yet
- Orofacial CystsDocument84 pagesOrofacial CystsWorku KifleNo ratings yet
- Ortho: - Orthopedic Instruments - Anatomy and Physiology - FractureDocument2 pagesOrtho: - Orthopedic Instruments - Anatomy and Physiology - FractureWorku KifleNo ratings yet
- Cast/Splint Choice and Application: Worku K. (MD)Document15 pagesCast/Splint Choice and Application: Worku K. (MD)Worku KifleNo ratings yet
- Arsi University College of Health Sciences Department of MedicineDocument127 pagesArsi University College of Health Sciences Department of MedicineWorku KifleNo ratings yet
- Dentistry HoDocument17 pagesDentistry HoWorku KifleNo ratings yet
- Aseptic Techniques: - Antiseptic or Antimicrobial AgentDocument17 pagesAseptic Techniques: - Antiseptic or Antimicrobial AgentWorku KifleNo ratings yet
- Maxillary Sinus DR - AssefaDocument65 pagesMaxillary Sinus DR - AssefaWorku KifleNo ratings yet
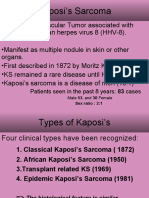
- Kaposi's Sarcoma: Patients Seen in The Past 8 Years: 83 CasesDocument12 pagesKaposi's Sarcoma: Patients Seen in The Past 8 Years: 83 CasesWorku KifleNo ratings yet
- Ped SurgDocument11 pagesPed SurgWorku KifleNo ratings yet
- Hypospadias Epispadias and Bladder Exstrophy: Khalid Abdella (MD) OCTOBER - 11 - 2006Document64 pagesHypospadias Epispadias and Bladder Exstrophy: Khalid Abdella (MD) OCTOBER - 11 - 2006Worku KifleNo ratings yet
- Melanoma Belay Z July, 6 2005Document20 pagesMelanoma Belay Z July, 6 2005Worku KifleNo ratings yet
- Acute Abdomen in ChildrenDocument61 pagesAcute Abdomen in ChildrenWorku KifleNo ratings yet
- Fluid and Electrolte Manageent in Paediatric Surgical PatientDocument29 pagesFluid and Electrolte Manageent in Paediatric Surgical PatientWorku KifleNo ratings yet
- Abdominal Wall DEFECTS: Omphalocele, Gastroschisis, Prune-BellyDocument38 pagesAbdominal Wall DEFECTS: Omphalocele, Gastroschisis, Prune-BellyWorku KifleNo ratings yet
- Neck Masses and FistulasDocument55 pagesNeck Masses and FistulasWorku KifleNo ratings yet
- Acute Abdomen: - DefinitionDocument27 pagesAcute Abdomen: - DefinitionWorku KifleNo ratings yet
- NEUROFIBROMATOSISDocument11 pagesNEUROFIBROMATOSISWorku KifleNo ratings yet
- Colilithiasis 2Document53 pagesColilithiasis 2Worku KifleNo ratings yet
- Vascular Malformation and LymphoedemaDocument44 pagesVascular Malformation and LymphoedemaWorku KifleNo ratings yet
- Melanoma: Meku Damtie (M.D.) July 18, 2006Document38 pagesMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNo ratings yet
- Gastrointestinal Hemorrhage2Document20 pagesGastrointestinal Hemorrhage2Worku KifleNo ratings yet
- Fluid & Electrolyte 2Document47 pagesFluid & Electrolyte 2Worku KifleNo ratings yet
- Obstruction of The Urinary TractDocument68 pagesObstruction of The Urinary TractWorku KifleNo ratings yet
- Perioperative Care 2Document28 pagesPerioperative Care 2Worku KifleNo ratings yet
- Sen Johnson Letter To FDA CDCDocument8 pagesSen Johnson Letter To FDA CDCZerohedge JanitorNo ratings yet
- Case Analysis in CholecystectomyDocument9 pagesCase Analysis in CholecystectomyMay Ann Magdaraog ArdamilNo ratings yet
- Method of Memorizing The Materia MedicaDocument72 pagesMethod of Memorizing The Materia MedicaFrank NavaNo ratings yet
- Sleep 20 1 18Document6 pagesSleep 20 1 18Turtle ArtNo ratings yet
- Blood Physio MCQSDocument6 pagesBlood Physio MCQSHammad Tariq0% (1)
- Clinical Pharma 3 فودةDocument210 pagesClinical Pharma 3 فودةRebwarNo ratings yet
- Infection Prevention (COVID-19) For Complementary Therapies and Sports MassageDocument15 pagesInfection Prevention (COVID-19) For Complementary Therapies and Sports MassageKristinaNo ratings yet
- Hygiene and Prevention: Hope 3Document11 pagesHygiene and Prevention: Hope 3Gerald TeañoNo ratings yet
- Go8 Road To RecoveryDocument192 pagesGo8 Road To RecoverygecrikNo ratings yet
- ASRM - Diagnostic Evaluation of The Infertile FemaleDocument11 pagesASRM - Diagnostic Evaluation of The Infertile FemaleMina zhouNo ratings yet
- Lesson Plan On Tuberculosis (Health Talk)Document8 pagesLesson Plan On Tuberculosis (Health Talk)Priyanka Jangra100% (2)
- Kaplan Q-Bank NotesDocument3 pagesKaplan Q-Bank NotesWirda ZafarNo ratings yet
- Treatment of Atypical Pneumonia With Azithromycin: Comparison of A 5-Day and A 3-Day CourseDocument6 pagesTreatment of Atypical Pneumonia With Azithromycin: Comparison of A 5-Day and A 3-Day Coursecath lauuuNo ratings yet
- The Small Intestine Channel of Hand TaiyangDocument165 pagesThe Small Intestine Channel of Hand TaiyangGeeta SajjanNo ratings yet
- 2023 Article 1392Document11 pages2023 Article 1392daniela.jara.mNo ratings yet
- Research A Clinical Study of Kankayan Vati in The Management of Arshas-Ayur ResearchDocument5 pagesResearch A Clinical Study of Kankayan Vati in The Management of Arshas-Ayur ResearchDrHassan Ahmed ShaikhNo ratings yet
- SURGERY 2020-2008 Chapter Wise Question Papers WBUHS © Medical JunctionDocument18 pagesSURGERY 2020-2008 Chapter Wise Question Papers WBUHS © Medical JunctionRanjan SorenNo ratings yet
- Special Report - The Real Cause of MigraineDocument22 pagesSpecial Report - The Real Cause of MigraineOriana LeoNo ratings yet
- Staphylococci & MicrococciDocument52 pagesStaphylococci & Micrococcihoneylemon.coNo ratings yet
- Dulcamara: SourceDocument8 pagesDulcamara: SourceKamalNo ratings yet
- KOD Final Year (M.B.B.S) - Survival GuideDocument30 pagesKOD Final Year (M.B.B.S) - Survival GuideMubasharAbrarNo ratings yet
- Case Study6 For HS 103 Week 7Document7 pagesCase Study6 For HS 103 Week 7Rijane Tabonoc OmlangNo ratings yet
- Readings IIDocument4 pagesReadings IIAdriana Berenice Rendón PortilloNo ratings yet
- Pathophysiology On Cellulitis On Left Facial AreaDocument9 pagesPathophysiology On Cellulitis On Left Facial AreaAdiNo ratings yet
- 2021 and 2022 Python IEEE Projects ListDocument4 pages2021 and 2022 Python IEEE Projects Listnikhil vardhanNo ratings yet
- Quality Improvement Case 1Document23 pagesQuality Improvement Case 1api-534814911No ratings yet
- 3.MCQ Good PushDocument19 pages3.MCQ Good Pushanderson ndabishakaNo ratings yet
- Basic Principles of Wound Management - UpToDateDocument44 pagesBasic Principles of Wound Management - UpToDatePriscillaNo ratings yet
- Dermatofitosis Estudios RecientesDocument21 pagesDermatofitosis Estudios RecientesFrancisca Thenée SerranoNo ratings yet