You might also like
- Miscellaneous For FinalsDocument30 pagesMiscellaneous For Finalsjames.a.blairNo ratings yet
- Long-Lasting SAVINGS: Save Each Time You Fill Your Mydayis Prescription.Document2 pagesLong-Lasting SAVINGS: Save Each Time You Fill Your Mydayis Prescription.rwurdigNo ratings yet
- Velez - Trade For WealthDocument91 pagesVelez - Trade For Wealthwappler99100% (14)
- Pediatric Hematology Oncology Ward Officer HandbookDocument40 pagesPediatric Hematology Oncology Ward Officer HandbookAnonymous FSUnLYr4yNo ratings yet
- RP Pattern Patsy Party Dress Ladies US Letter PDFDocument99 pagesRP Pattern Patsy Party Dress Ladies US Letter PDFЕкатерина Ростова100% (5)
- Gifts From The GodsDocument27 pagesGifts From The GodsLaura ClipsonNo ratings yet
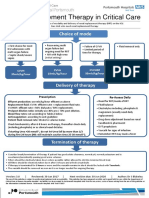
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Pediatric Hematology Oncology Ward Officer HandbookDocument40 pagesPediatric Hematology Oncology Ward Officer HandbookLetchumana KrishnanNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- Anticoagulant Pocket GuideDocument8 pagesAnticoagulant Pocket GuideDrew John Minardi100% (2)
- Low Molecular Weight Heparins (LMWH) : I. Mechanism of ActionDocument7 pagesLow Molecular Weight Heparins (LMWH) : I. Mechanism of ActionIniya RajendranNo ratings yet
- DabigatranDocument25 pagesDabigatranNagesh JadavNo ratings yet
- OctaplexDocument3 pagesOctaplexraul sinatoNo ratings yet
- Anticoagulant TherapyDocument47 pagesAnticoagulant TherapyAndriKusuma75% (4)
- Case Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerDocument19 pagesCase Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerUmme habeebaNo ratings yet
- ACLS ModuleDocument68 pagesACLS ModuleSalah ElbadawyNo ratings yet
- 1000 - Johnson Venous ThrombDocument33 pages1000 - Johnson Venous ThrombAlejandro Kanito Alvarez SNo ratings yet
- Anaesthesia For A Patient With Coagulation DisorderDocument33 pagesAnaesthesia For A Patient With Coagulation DisorderNdenwaneku OkuwaNo ratings yet
- Neuraxial Blockade and AnticoagulantsDocument69 pagesNeuraxial Blockade and Anticoagulantskamel6No ratings yet
- Drugs Related To ClottingDocument23 pagesDrugs Related To ClottingBig PigNo ratings yet
- Nursing Orientation Program Intravenous TherapyDocument45 pagesNursing Orientation Program Intravenous TherapyMarianne LayloNo ratings yet
- Heparin Drip ProtocolDocument16 pagesHeparin Drip Protocolapi-277534147100% (1)
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarNo ratings yet
- Critical Care Drugs 2Document23 pagesCritical Care Drugs 2Asri Ernadi100% (1)
- Anticoagulants: Presented By: ABHILASH Moderator: DR CH RAHUL MDDocument103 pagesAnticoagulants: Presented By: ABHILASH Moderator: DR CH RAHUL MDabhilashreddy45100% (1)
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDocument4 pagesAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoNo ratings yet
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- CASE PRESENTATION PneumoniaDocument13 pagesCASE PRESENTATION PneumoniaHari Singh RathoreNo ratings yet
- Anti CoagulantsDocument37 pagesAnti CoagulantsMaria khurshidNo ratings yet
- AnticoagulantDocument47 pagesAnticoagulantasma barhoomNo ratings yet
- Anticoagulation PharmacologyDocument36 pagesAnticoagulation PharmacologyaymenNo ratings yet
- Reversing The New AnticoagulantsDocument24 pagesReversing The New AnticoagulantsFurman BorstNo ratings yet
- ASRA Guidelines For CNBDocument66 pagesASRA Guidelines For CNBAshiyan IrfanNo ratings yet
- Acs 2023 Part 4 Presentation VersionDocument38 pagesAcs 2023 Part 4 Presentation Versionapi-668470097No ratings yet
- AnticoagulantsDocument19 pagesAnticoagulantsOsama ZbedaNo ratings yet
- Blood and Blood ProductsDocument52 pagesBlood and Blood Productswellawalalasith100% (1)
- AnticoagulantsDocument64 pagesAnticoagulantsnainapattnaikNo ratings yet
- MoonlightingDocument282 pagesMoonlightingMeg Mateo100% (1)
- Pharmacological and Parenteral TherapiesDocument99 pagesPharmacological and Parenteral TherapieslNo ratings yet
- CP ON PUD (1) ADocument20 pagesCP ON PUD (1) ADeekshitha DanthuluriNo ratings yet
- Oncology CaseDocument15 pagesOncology CaseRimsha AzeemNo ratings yet
- IV To PO Conversion PolicyDocument4 pagesIV To PO Conversion PolicyIrham NiNo ratings yet
- COVID-19 Drugs & Treatment: BWH Quick-Reference GuideDocument1 pageCOVID-19 Drugs & Treatment: BWH Quick-Reference GuideBoules AtefNo ratings yet
- Diagnose CKD:: ACE inhibitor/ARB UseDocument2 pagesDiagnose CKD:: ACE inhibitor/ARB UseAman AmanNo ratings yet
- Rancangan Bentuk Sediaan Farmasi Compatibility ModeDocument18 pagesRancangan Bentuk Sediaan Farmasi Compatibility ModeNully Andaretha SugiantoNo ratings yet
- Pharmacology For Nclex PowerPointDocument209 pagesPharmacology For Nclex PowerPointEver Rose DangaseNo ratings yet
- Nigeria CME - Optimal - Care - For - Dvt-Pe - PatientsDocument48 pagesNigeria CME - Optimal - Care - For - Dvt-Pe - PatientsStella CooKeyNo ratings yet
- UHP ROTEM ImplementationDocument30 pagesUHP ROTEM Implementationppica8111No ratings yet
- Anticoagulants by DR TariqDocument46 pagesAnticoagulants by DR Tariqsinan kNo ratings yet
- Bivalirudine Drug Presentation From Nicvd DhakaDocument28 pagesBivalirudine Drug Presentation From Nicvd DhakaNavojit ChowdhuryNo ratings yet
- Cisplatin/ 5-Fluorouracil For Squamous Cell Carcinoma Head and Neck (HNSCC) - Day Unit ProtocolDocument6 pagesCisplatin/ 5-Fluorouracil For Squamous Cell Carcinoma Head and Neck (HNSCC) - Day Unit Protocoldwi harisNo ratings yet
- Anticoagulant DOACDocument39 pagesAnticoagulant DOACSukmawatiNo ratings yet
- Drugs Used in Cardiovascular SystemDocument57 pagesDrugs Used in Cardiovascular SystemSandeep ChaudharyNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Anticoagulation Dosing Recommendations COVID 19 PatientsDocument1 pageAnticoagulation Dosing Recommendations COVID 19 PatientsChalwe HowardNo ratings yet
- DILIDocument40 pagesDILIYunik YuliapsariNo ratings yet
- Orig 1 S 187 LBLDocument20 pagesOrig 1 S 187 LBLfarezpharmaNo ratings yet
- Anticoagulation in Hemodialysis: Arlene S. Munoz MD, FPCP, FPSNDocument51 pagesAnticoagulation in Hemodialysis: Arlene S. Munoz MD, FPCP, FPSNBryant MunozNo ratings yet
- Anticoagulation Monitoring Hand-OutDocument69 pagesAnticoagulation Monitoring Hand-OutApril OcampoNo ratings yet
- Trasylol Ti: Administration. The Risk For A Fatal Reaction Appears To Be Greater Upon ReDocument15 pagesTrasylol Ti: Administration. The Risk For A Fatal Reaction Appears To Be Greater Upon ReNARESH JANDIALNo ratings yet
- Bevacizumab Carboplatin Paclitaxel For Cervical Cancers CRP14GY017 v1.0Document6 pagesBevacizumab Carboplatin Paclitaxel For Cervical Cancers CRP14GY017 v1.0andibarosNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- 1 GENERAL NOTES MergedDocument23 pages1 GENERAL NOTES MergedLaedyn Faye IsipNo ratings yet
- EPRI - Research On Concrete For Nuclear PlantsDocument2 pagesEPRI - Research On Concrete For Nuclear Plantsvggupta2No ratings yet
- WLP Mapeh 10Document2 pagesWLP Mapeh 10marry rose gardoseNo ratings yet
- What Is Narrative ParagraphDocument3 pagesWhat Is Narrative ParagraphAnderson LeonNo ratings yet
- DESIGN CRITERIA FOR MASS HOUSING Vinod Gupta, M. N. Ganju, Romi KhoslaDocument3 pagesDESIGN CRITERIA FOR MASS HOUSING Vinod Gupta, M. N. Ganju, Romi KhoslaAnju WantiNo ratings yet
- ONVIF Profile Feature Overview v2-2Document6 pagesONVIF Profile Feature Overview v2-2nsadnanNo ratings yet
- OGDCL Trainee Test 2018 NTSDocument1 pageOGDCL Trainee Test 2018 NTSBilal AhmadNo ratings yet
- MATH 7 ADM Module 6 FINALDocument32 pagesMATH 7 ADM Module 6 FINALRonnil Quieta100% (9)
- ACC111 Week1-3 ULOaDocument24 pagesACC111 Week1-3 ULOaRyzza DaclanNo ratings yet
- Imamate PDFDocument16 pagesImamate PDFsaidatuladaniNo ratings yet
- Final Report (Azlan) PDFDocument77 pagesFinal Report (Azlan) PDFEnrick TedNo ratings yet
- KLP 104 ManualDocument10 pagesKLP 104 ManualTania LuzonNo ratings yet
- Physics Investigatory Project Class 12Document22 pagesPhysics Investigatory Project Class 12Vaibhav JethaniNo ratings yet
- Nature of Fraud and Its Effects in The Medical Insurance KenyaDocument12 pagesNature of Fraud and Its Effects in The Medical Insurance KenyaSaarah ConnieNo ratings yet
- Real Life Application of Linear AlgebraDocument9 pagesReal Life Application of Linear AlgebraSeerat BatoolNo ratings yet
- wph14 01 Rms 20240307Document16 pageswph14 01 Rms 20240307huzaifashahid590No ratings yet
- Resolute Electronics: Quotation Quotation No: Quotation DateDocument1 pageResolute Electronics: Quotation Quotation No: Quotation DatePANCHATCHARAM SNo ratings yet
- S36-23302 SIE Service Offshore 12pp.Document7 pagesS36-23302 SIE Service Offshore 12pp.Uhrin ImreNo ratings yet
- Taxiway Signs, Markings, LightsDocument2 pagesTaxiway Signs, Markings, Lightsapi-282893463No ratings yet
- Etsi DMR ProtocoloDocument177 pagesEtsi DMR ProtocoloIvan Flores MelchorNo ratings yet
- Darla ResumeDocument2 pagesDarla Resumeapi-3709962No ratings yet
- Esa Lecture Notes PDFDocument205 pagesEsa Lecture Notes PDFSwaroop MunavalliNo ratings yet
- Cornisas de PoliestirenoDocument84 pagesCornisas de PoliestirenoJorgeSalazarBorquezNo ratings yet
- TPN8C30 M&E Inspection FormDocument32 pagesTPN8C30 M&E Inspection FormWunNaNo ratings yet
- Classifications of Hotel Departments UNIT 4Document19 pagesClassifications of Hotel Departments UNIT 4Fransiska Way Warti RobertsonNo ratings yet
- Sage X3 - User Guide - HTG-RNI Report PDFDocument6 pagesSage X3 - User Guide - HTG-RNI Report PDFcaplusincNo ratings yet