You might also like
- Cerebro Vascular AttackDocument10 pagesCerebro Vascular AttackKalyan Babu VakaNo ratings yet
- Hamda Mohammad Sa'adeh - PCI Final ReportDocument4 pagesHamda Mohammad Sa'adeh - PCI Final Reportshamaamo19No ratings yet
- Primary PCI To LAD and LCXDocument3 pagesPrimary PCI To LAD and LCXshamaamo19No ratings yet
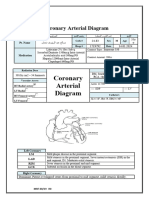
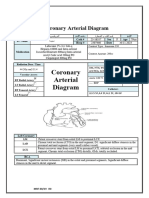
- Coronary Arterial DiagramDocument3 pagesCoronary Arterial Diagramshamaamo19No ratings yet
- Hemostatic Abnormalities in Dogs With HemangiosarcomaDocument4 pagesHemostatic Abnormalities in Dogs With HemangiosarcomaAllana Valau MoreiraNo ratings yet
- Clinical Controversy TPA Use in Cardiac ArrestDocument33 pagesClinical Controversy TPA Use in Cardiac Arrestkhangsiean89No ratings yet
- Cardiac CathDocument3 pagesCardiac Cathshamaamo19No ratings yet
- Mubeens Clinical Examinations Crib Sheet PDFDocument36 pagesMubeens Clinical Examinations Crib Sheet PDFTimothy HarwichNo ratings yet
- Duty Ricky CKD R.28 NewDocument4 pagesDuty Ricky CKD R.28 NewRicky Cornelius TariganNo ratings yet
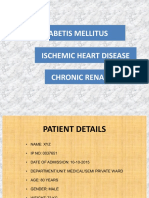
- Diabetis Mellitus Ischemic Heart Disease Chronic Renal FailureDocument24 pagesDiabetis Mellitus Ischemic Heart Disease Chronic Renal FailureBharath GowdaNo ratings yet
- Casos de Estudio Desordenes HemorragicosDocument8 pagesCasos de Estudio Desordenes HemorragicosGabriela SotoNo ratings yet
- Non POMR 22 Oktober 2019Document17 pagesNon POMR 22 Oktober 2019magda SiraitNo ratings yet
- Non POMR 22 Oktober 2019Document19 pagesNon POMR 22 Oktober 2019magda SiraitNo ratings yet
- MR 2 Juni OA, AzotemiaDocument32 pagesMR 2 Juni OA, AzotemiaAlvin PratamaNo ratings yet
- MR 2 Juni OA, AzotemiaDocument32 pagesMR 2 Juni OA, AzotemiaWenNy RupiNaNo ratings yet
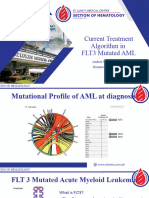
- Aml FLT3Document27 pagesAml FLT3Dea ReyesNo ratings yet
- Evolving Paradigm Shifts: Acute PE ManagementDocument53 pagesEvolving Paradigm Shifts: Acute PE Managementadamu mohammadNo ratings yet
- A 55 Years Old Man With Chest PainDocument23 pagesA 55 Years Old Man With Chest Painzulfikar adiNo ratings yet
- Cardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIDocument30 pagesCardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIFikriYTNo ratings yet
- Coronary Arterial DiagramDocument4 pagesCoronary Arterial Diagramshamaamo19No ratings yet
- Demo PresentationDocument29 pagesDemo PresentationGanesh ChaudhariNo ratings yet
- 10 1002@art 1780390218Document5 pages10 1002@art 1780390218MICHAEL NUGROHONo ratings yet
- Oxcarbazepine-Induced Hyponatremia, A Cross-Sectional StudyDocument3 pagesOxcarbazepine-Induced Hyponatremia, A Cross-Sectional StudydenisNo ratings yet
- Renalised HypertensionDocument43 pagesRenalised HypertensionsuganNo ratings yet
- Tube Additive Laboratory Use TestsDocument2 pagesTube Additive Laboratory Use TestsSilvia_dsc100% (1)
- Tpe in Critical C 19Document47 pagesTpe in Critical C 19arif dwi antoNo ratings yet
- Adobe Scan Apr 08, 2021Document7 pagesAdobe Scan Apr 08, 2021Kuldeep YadavNo ratings yet
- 5 Parathyroid Hormone5Document58 pages5 Parathyroid Hormone5Rawbeena RamtelNo ratings yet
- Abnormal Heart Rate Regulation in Murine Hearts With Familial Hypertrophic Cardiomyopathy-Related Cardiac Troponin T MutationsDocument10 pagesAbnormal Heart Rate Regulation in Murine Hearts With Familial Hypertrophic Cardiomyopathy-Related Cardiac Troponin T MutationsJill johhNo ratings yet
- Comparative QSAR Studies On Bibenzimidazoles and Terbenzimidazoles Inhibiting Topoisomerase IDocument9 pagesComparative QSAR Studies On Bibenzimidazoles and Terbenzimidazoles Inhibiting Topoisomerase IguptealpanaNo ratings yet
- Jcem 4398Document5 pagesJcem 4398vegagbNo ratings yet
- Sfss TurkeyDocument68 pagesSfss TurkeytasarimkutusuNo ratings yet
- TestsDocument3 pagesTestsaddajrfNo ratings yet
- Erna 2009Document25 pagesErna 2009Colleen Van SchalkwykNo ratings yet
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDocument65 pagesLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranNo ratings yet
- Presus MalariaDocument66 pagesPresus MalariaAlchemistalazkaNo ratings yet
- Humaclot Duo: Specifications & MoreDocument4 pagesHumaclot Duo: Specifications & MoreMaherNo ratings yet
- Mito NGSDocument49 pagesMito NGSLaél BullockNo ratings yet
- REV POMR KIPI SatyaDocument20 pagesREV POMR KIPI SatyaDoctoRides 46No ratings yet
- GeneXpert XDR Dummy Report (140123)Document2 pagesGeneXpert XDR Dummy Report (140123)Mahesh TilanteNo ratings yet
- 2007 PFTs The Forced Oscillation TechniqueDocument50 pages2007 PFTs The Forced Oscillation TechniqueServiço de Imunoalergologia - H.S. João100% (1)
- Hong Kong New-1Document59 pagesHong Kong New-1Muhammad Isnaini ZuhriNo ratings yet
- Spontaneous Feline Hyperthyroidism: January 1980Document2 pagesSpontaneous Feline Hyperthyroidism: January 1980Kurt SciclunaNo ratings yet
- 2.postoperative Arrhythmias in Open-Heart SurgeryDocument9 pages2.postoperative Arrhythmias in Open-Heart Surgeryganda gandaNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- Intensive Care Unit Report: Friday, November 19 2021Document8 pagesIntensive Care Unit Report: Friday, November 19 2021raymondNo ratings yet
- The Expression of Annexin II and Its Role in The Fibrinolytic Activity in Acute Promyelocytic LeukemiaDocument6 pagesThe Expression of Annexin II and Its Role in The Fibrinolytic Activity in Acute Promyelocytic LeukemiaLaura LópezNo ratings yet
- Lab Anim-1998-Asano-214-8Document6 pagesLab Anim-1998-Asano-214-8Лилия ПоляковаNo ratings yet
- Morning Report: Date: 6 April 2021Document17 pagesMorning Report: Date: 6 April 2021Adinda DianNo ratings yet
- Blood Brochure International - 210528Document4 pagesBlood Brochure International - 210528James NorldNo ratings yet
- Primary Aldosteronism ShiftsDocument3 pagesPrimary Aldosteronism ShiftsAngela WilsonNo ratings yet
- Distal LM TrifurcationDocument62 pagesDistal LM TrifurcationSebastian ChandraNo ratings yet
- Tratamentul Itu: Masuri GeneraleDocument34 pagesTratamentul Itu: Masuri Generalemihai mayorNo ratings yet
- Morning Report: Physician in ChargeDocument11 pagesMorning Report: Physician in ChargeImam Mi'raj SuprayogaNo ratings yet
- Acute Care of Burns PatientsDocument30 pagesAcute Care of Burns PatientsRafael BagusNo ratings yet
- Austin HematologyDocument3 pagesAustin HematologyAustin Publishing GroupNo ratings yet
- Friday 2-2-2018 Multiple MyelomaDocument20 pagesFriday 2-2-2018 Multiple MyelomaJefri SusantoNo ratings yet
- Molecular Diagnosis: in Oncology & GeneticsDocument101 pagesMolecular Diagnosis: in Oncology & GeneticsSorin LazarNo ratings yet
- Calculation of Renal Tubular Reabsorption of Phosphate: The Algorithm Performs Better Than The NomogramDocument4 pagesCalculation of Renal Tubular Reabsorption of Phosphate: The Algorithm Performs Better Than The NomogramutamiprakosoNo ratings yet
- 510 (K) Substantial Equivalence Determination Decision MemorandumDocument11 pages510 (K) Substantial Equivalence Determination Decision MemorandumJamesNo ratings yet
- Synchron System(s) Chemistry Information Sheet T4: ThyroxineDocument14 pagesSynchron System(s) Chemistry Information Sheet T4: ThyroxineJamesNo ratings yet
- Lab Forward: Quality Forward Consistency ForwardDocument12 pagesLab Forward: Quality Forward Consistency ForwardJamesNo ratings yet
- K090588Document9 pagesK090588JamesNo ratings yet
- Synchron System(s) Chemistry Information Sheet T4: ThyroxineDocument14 pagesSynchron System(s) Chemistry Information Sheet T4: ThyroxineJamesNo ratings yet
- Department of Health & Human ServicesDocument24 pagesDepartment of Health & Human ServicesJamesNo ratings yet
- DXC 700 AU Competency ChecklistDocument7 pagesDXC 700 AU Competency ChecklistJamesNo ratings yet
- J. Reynolds, B Godber, K.L Breasley, S O'Mahony, D. Fitzgerald, H.Kelly Beckman Coulter, Co Clare, IrelandDocument1 pageJ. Reynolds, B Godber, K.L Breasley, S O'Mahony, D. Fitzgerald, H.Kelly Beckman Coulter, Co Clare, IrelandJames100% (1)
- Blood Glucose: J - Michael McmillinDocument4 pagesBlood Glucose: J - Michael McmillinJamesNo ratings yet
- Structure of DNA PDFDocument7 pagesStructure of DNA PDFJamesNo ratings yet
- Clinical Toxicology Page 1 of 9Document9 pagesClinical Toxicology Page 1 of 9JamesNo ratings yet
- Diabetic Profile: Ravi KumudeshDocument61 pagesDiabetic Profile: Ravi KumudeshJamesNo ratings yet
- The Impact of Preanalytic Factors of Glucose MeasuDocument30 pagesThe Impact of Preanalytic Factors of Glucose MeasuJamesNo ratings yet
- SSchindler DNADocument27 pagesSSchindler DNARafael GermanoNo ratings yet
- Bacteria Eukarya EukaryogenesisDocument20 pagesBacteria Eukarya EukaryogenesisJamesNo ratings yet
- Dna StructureDocument7 pagesDna StructurehoneyworksNo ratings yet
- Structure of DNA PDFDocument7 pagesStructure of DNA PDFJamesNo ratings yet
- Dna Structure and FunctionDocument18 pagesDna Structure and FunctionAdonai Jireh Dionne BaliteNo ratings yet
- Characteristics and Properties of Amino Acids (AA)Document52 pagesCharacteristics and Properties of Amino Acids (AA)JamesNo ratings yet
- 1953: The Discovery of The Structure of DNADocument6 pages1953: The Discovery of The Structure of DNAJamesNo ratings yet
- Dnastructureandproperties 120302083818 Phpapp01Document31 pagesDnastructureandproperties 120302083818 Phpapp01Shiella Mae Baltazar BulauitanNo ratings yet
- Molecular Diagnostics Techniques Polymerase Chain ReactionDocument7 pagesMolecular Diagnostics Techniques Polymerase Chain ReactionJamesNo ratings yet
- Dna ReplicationDocument2 pagesDna ReplicationJamesNo ratings yet
- Oswald AveryDocument2 pagesOswald AveryJamesNo ratings yet
- Oral Gas ChromatographyDocument3 pagesOral Gas ChromatographyJamesNo ratings yet
- RC507 BarbituratesDocument13 pagesRC507 BarbituratesJamesNo ratings yet
- CHROMATOGRAPHY - Bonham ChemistryDocument8 pagesCHROMATOGRAPHY - Bonham ChemistryJamesNo ratings yet
- 2.1 - Basic SpectrophotometryDocument4 pages2.1 - Basic SpectrophotometryJamesNo ratings yet
- High Pressure Liquid Chromatography (HPLC)Document21 pagesHigh Pressure Liquid Chromatography (HPLC)JamesNo ratings yet
- PresentationDocument16 pagesPresentationarun aryaNo ratings yet
- Abegail Joy B. Manlunas BS Psychology: Endocrine System Organ Hormone Function Disorder If Too High Disorder If Too LowDocument4 pagesAbegail Joy B. Manlunas BS Psychology: Endocrine System Organ Hormone Function Disorder If Too High Disorder If Too LowabegailmanlunasNo ratings yet
- CHAPTER 10 ANAPHY TransesDocument8 pagesCHAPTER 10 ANAPHY TransesHoly HaeinNo ratings yet
- Parathyroid Disease Lecture SlidesDocument50 pagesParathyroid Disease Lecture SlidesMaxwell PalSingh100% (1)
- Anatomy and Function of The HypothalamusDocument13 pagesAnatomy and Function of The HypothalamusNrs Sani Sule MashiNo ratings yet
- Thyroid (Hyper & Hypo) - Patho, Causes, LabsDocument1 pageThyroid (Hyper & Hypo) - Patho, Causes, LabsVishalNo ratings yet
- Quiz EndocrineDocument16 pagesQuiz EndocrineMon DoceNo ratings yet
- Endocrine System Pathology PPT Lecture SeriesDocument285 pagesEndocrine System Pathology PPT Lecture SeriesMarc Imhotep Cray, M.D.100% (6)
- Hillson Thyroid DisordersDocument90 pagesHillson Thyroid DisordersGirish SubashNo ratings yet
- Healthy Hormones Happy Brain 2420Document15 pagesHealthy Hormones Happy Brain 2420Eva MNo ratings yet
- MEDTHERA 3.06 Drugs Used in Thyroid ConditionsDocument28 pagesMEDTHERA 3.06 Drugs Used in Thyroid ConditionsNDJNo ratings yet
- Endocrine Anesthesia MCQsDocument18 pagesEndocrine Anesthesia MCQsMuhammad Aasim Maan100% (2)
- The Renin Angiotensin Aldosterone System - RAASDocument3 pagesThe Renin Angiotensin Aldosterone System - RAASrienz nicnic peraltaNo ratings yet
- Thyroid Function Tests FaqDocument1 pageThyroid Function Tests FaqUttam AuddyNo ratings yet
- Sem 4 MCQ Week 4 Jan 2014 CTL McqsDocument15 pagesSem 4 MCQ Week 4 Jan 2014 CTL McqsFlowerNo ratings yet
- Gazz Med Ital - Arch Sci Med-3099 - Proof in PDF - V1 - 2014-10-30Document12 pagesGazz Med Ital - Arch Sci Med-3099 - Proof in PDF - V1 - 2014-10-30Bassem RefaatNo ratings yet
- Chapter 9 - Endocrine System NotesDocument9 pagesChapter 9 - Endocrine System Notesvictoria skoubourisNo ratings yet
- Royal Alexandra Hospital For Children: Policy & Procedures ManualDocument73 pagesRoyal Alexandra Hospital For Children: Policy & Procedures ManualDivya NarayanNo ratings yet
- ENDOCRINE SYSTEM - Anatomy and PhysiologyDocument10 pagesENDOCRINE SYSTEM - Anatomy and PhysiologyJay Crishnan Morales CajandingNo ratings yet
- Sciences2lp ModakiratDocument29 pagesSciences2lp Modakiratapi-24974205850% (4)
- Pengaruh Pendidikan Kesehatan Terhadap Pengetahuan Dan Sikap Ibu Hamil Tentang Skrining Hipotiroid Bayi Baru Lahir Di Wilayah Kerja Puskesmas KawalDocument10 pagesPengaruh Pendidikan Kesehatan Terhadap Pengetahuan Dan Sikap Ibu Hamil Tentang Skrining Hipotiroid Bayi Baru Lahir Di Wilayah Kerja Puskesmas KawalAgum Nila SariNo ratings yet
- Thyroid PathologyDocument9 pagesThyroid PathologyNada MuchNo ratings yet
- Hashimoto and Grave DiseaseDocument9 pagesHashimoto and Grave DiseaseNadia ElaizaNo ratings yet
- 7.3 Endocrine Disorders PPTDocument36 pages7.3 Endocrine Disorders PPTLorelie AsisNo ratings yet
- EMS Case 1 MPHDDocument44 pagesEMS Case 1 MPHDFatita Restu HermawanNo ratings yet
- Hypothalamic and Pituitary FunctionDocument3 pagesHypothalamic and Pituitary FunctionHannah SolomonNo ratings yet
- Adrenal GlandDocument47 pagesAdrenal GlandsuthaNo ratings yet
- PituitaryDocument15 pagesPituitaryBivek PokhrelNo ratings yet
- Pitfalls in The Assessment of Gestational Transient ThyrotoxicosisDocument7 pagesPitfalls in The Assessment of Gestational Transient ThyrotoxicosisTandyo TriasmoroNo ratings yet
- MUL, Dick PDFDocument240 pagesMUL, Dick PDFNursyamsuddin MoganaNo ratings yet
- Endocrine System 5Document15 pagesEndocrine System 5Ace Vincent LunaNo ratings yet