You might also like
- What Is Biochemistry NBME USMLE ABCDDocument37 pagesWhat Is Biochemistry NBME USMLE ABCDTanvir Ahmed100% (1)
- Gyne Book 20122Document194 pagesGyne Book 20122თამარ ჩალაურიNo ratings yet
- You Exec - KPIs - 169 - BlueDocument14 pagesYou Exec - KPIs - 169 - BlueEssa SmjNo ratings yet
- Finding The Answers To The Research Questions (Qualitative) : Quarter 4 - Module 5Document39 pagesFinding The Answers To The Research Questions (Qualitative) : Quarter 4 - Module 5Jernel Raymundo80% (5)
- RIBA Outline Plan of Work ExplainedDocument20 pagesRIBA Outline Plan of Work ExplainedkenNo ratings yet
- Why it's important to guard your free timeDocument2 pagesWhy it's important to guard your free timeLaura Camila Garzón Cantor100% (1)
- Pediatric Within-Day Biological Variation and Quality Specifications For 38 Biochemical Markers in The CALIPER CohortDocument12 pagesPediatric Within-Day Biological Variation and Quality Specifications For 38 Biochemical Markers in The CALIPER CohortElmyLiantika MaranantanNo ratings yet
- 2017 La Iniciativa de Laboratorio Canadiense Sobre Intervalos de Referencia Pediátricos. Un Documento Técnico de CALIPERDocument57 pages2017 La Iniciativa de Laboratorio Canadiense Sobre Intervalos de Referencia Pediátricos. Un Documento Técnico de CALIPERpintopablo108bNo ratings yet
- The Path To Perfect Pediatric Posology - Drug Development in PediatricsDocument10 pagesThe Path To Perfect Pediatric Posology - Drug Development in PediatricsMaki-Chan マキNo ratings yet
- 2015 Management of Ingested Foreign Bodies in Children - A Clinical Report of The NASPGHAN Endoscopy CommitteeDocument13 pages2015 Management of Ingested Foreign Bodies in Children - A Clinical Report of The NASPGHAN Endoscopy CommitteeCarlos CuadrosNo ratings yet
- 518 FullDocument12 pages518 FullMARIA CRUZNo ratings yet
- Clinical Case Study Old Boy With "Milky" SerumDocument3 pagesClinical Case Study Old Boy With "Milky" Serumالشهيد محمدNo ratings yet
- Pathologist Time Spent on Pediatric AutopsiesDocument6 pagesPathologist Time Spent on Pediatric AutopsiesbeosroNo ratings yet
- Advances in Pediatric Reference Intervals For Biochemical Markers: Establishment of The Caliper Database in Healthy Children and AdolescentsDocument9 pagesAdvances in Pediatric Reference Intervals For Biochemical Markers: Establishment of The Caliper Database in Healthy Children and AdolescentsSid TyagiNo ratings yet
- NSLB BulletinDocument32 pagesNSLB Bulletinfreddy salcedoNo ratings yet
- Medical Genetics Ethics Cases For InterviewsDocument34 pagesMedical Genetics Ethics Cases For InterviewscatherineNo ratings yet
- Ajph.63.11 Suppl.28 PDFDocument10 pagesAjph.63.11 Suppl.28 PDFAntonius448No ratings yet
- Strategies For Neonatal Hyperbilirubinemia A Literature ReviewDocument5 pagesStrategies For Neonatal Hyperbilirubinemia A Literature Reviewea7e9pm9No ratings yet
- Pediatric Critical Values Laboratory PedDocument4 pagesPediatric Critical Values Laboratory Pediq_dianaNo ratings yet
- Metabolic Screening and Postnatal Glucose Homeostasis in The NewbornDocument25 pagesMetabolic Screening and Postnatal Glucose Homeostasis in The NewbornGuillermo CalderaroNo ratings yet
- Neonatal JaundiceDocument3 pagesNeonatal JaundiceMohola Tebello GriffithNo ratings yet
- Original Research: Neonatal Peripherally Inserted Central Catheter Practices and ProvidersDocument13 pagesOriginal Research: Neonatal Peripherally Inserted Central Catheter Practices and ProvidersWinarti RimadhaniNo ratings yet
- Investigating and Managing Non-immune Fetal HydropsDocument14 pagesInvestigating and Managing Non-immune Fetal HydropsMariana González DíazNo ratings yet
- Acute Kidney Injury in ChildrenDocument8 pagesAcute Kidney Injury in ChildrenInfectologia ClinicaNo ratings yet
- Literature Review Neonatal JaundiceDocument6 pagesLiterature Review Neonatal Jaundiceafdtvdcwf100% (1)
- Hiperbilirrubinemia Neonatal ExtremaDocument3 pagesHiperbilirrubinemia Neonatal ExtremaKateNo ratings yet
- Best Practices For Sample Storage UrineDocument41 pagesBest Practices For Sample Storage UrinekinnusaraiNo ratings yet
- Ten-Year Single-Center Experience of The Ketogenic Diet: Factors in Uencing Efficacy, Tolerability, and ComplianceDocument8 pagesTen-Year Single-Center Experience of The Ketogenic Diet: Factors in Uencing Efficacy, Tolerability, and ComplianceMarcin CiekalskiNo ratings yet
- Karumbi Et Al 2013Document6 pagesKarumbi Et Al 2013sundaimeNo ratings yet
- BMC Pediatrics: Management of Neonatal Hyperbilirubinemia: Pediatricians' Practices and Educational NeedsDocument7 pagesBMC Pediatrics: Management of Neonatal Hyperbilirubinemia: Pediatricians' Practices and Educational Needsmaya maeNo ratings yet
- Neonatal Jaundice: A Review and Guidelines For Its Management in Resource Limited CountriesDocument29 pagesNeonatal Jaundice: A Review and Guidelines For Its Management in Resource Limited CountriesJovian LutfiNo ratings yet
- Georgirene D. Vladutiu, PH.DDocument9 pagesGeorgirene D. Vladutiu, PH.DfdablogNo ratings yet
- SR and Guidelines For Periop MGMT of Peds Patients Undergoing Major Plastic SurgeryDocument10 pagesSR and Guidelines For Periop MGMT of Peds Patients Undergoing Major Plastic SurgeryPaul MarjiNo ratings yet
- JOURNAL The Preanalytical Phase - Past, Present, and FutureDocument3 pagesJOURNAL The Preanalytical Phase - Past, Present, and FutureVincent ReyesNo ratings yet
- 1394 FullDocument9 pages1394 FullDanielle AndreiNo ratings yet
- Common Laboratory Investigations in Obstetrics and GynaecologyDocument4 pagesCommon Laboratory Investigations in Obstetrics and GynaecologyIndhumathiNo ratings yet
- JNNfinalDocument29 pagesJNNfinalmutia larasati albarNo ratings yet
- Thesis On Neonatal SepticemiaDocument4 pagesThesis On Neonatal Septicemiaveronicasulaimannewyork100% (2)
- Newborn Screening For Biliary Atresia: Technical ReportDocument9 pagesNewborn Screening For Biliary Atresia: Technical ReportCarlos CuadrosNo ratings yet
- Acute Management of Pediatric Cyclic Vomiting Syndrome A Systematic ReviewDocument11 pagesAcute Management of Pediatric Cyclic Vomiting Syndrome A Systematic ReviewNanda WibowoNo ratings yet
- Design of A Prospective Multicenter Randomized Controlled Trial Evaluating The Effects of Gastric Lavage On Coffee-Ground Emesis in Neonates: Study ProtocolDocument6 pagesDesign of A Prospective Multicenter Randomized Controlled Trial Evaluating The Effects of Gastric Lavage On Coffee-Ground Emesis in Neonates: Study ProtocoltriaanggareniNo ratings yet
- Gestation Management of Hyperbilirubinemia in The Newborn Infant 35 or More Weeks ofDocument22 pagesGestation Management of Hyperbilirubinemia in The Newborn Infant 35 or More Weeks ofArielRetamalNo ratings yet
- Bacterial inhibition assay for early detection of maple syrup urine diseaseDocument7 pagesBacterial inhibition assay for early detection of maple syrup urine diseasejon paul reyesNo ratings yet
- Health Maintenance in School-Aged Children: Part I. History, Physical Examination, Screening, and ImmunizationsDocument6 pagesHealth Maintenance in School-Aged Children: Part I. History, Physical Examination, Screening, and ImmunizationsPhilippe Ceasar C. BascoNo ratings yet
- EvaluationPediatricLT2014 PDFDocument37 pagesEvaluationPediatricLT2014 PDFDewanggaWahyuPrajaNo ratings yet
- Constipacion en Niños y Adolescentes Evaluacion y TtoDocument10 pagesConstipacion en Niños y Adolescentes Evaluacion y TtoSebastian Medina RiveraNo ratings yet
- Newborn Screening: New Developments, New Dilemmas: GeneticsDocument6 pagesNewborn Screening: New Developments, New Dilemmas: GeneticsChester Soriano BalabagNo ratings yet
- Optimizing Colon CleansingDocument7 pagesOptimizing Colon CleansingrebeccaNo ratings yet
- The Preanalytical PhaseDocument24 pagesThe Preanalytical PhaseArturo Eduardo Huarcaya OntiverosNo ratings yet
- Jurnal Hiperbilirubin 2Document3 pagesJurnal Hiperbilirubin 2Seni safitriNo ratings yet
- Bristol Stool ScaleDocument6 pagesBristol Stool ScaleKoas PatoNo ratings yet
- Medicina 56 00299 PDFDocument12 pagesMedicina 56 00299 PDFannisa sakinahNo ratings yet
- Prevalence and Potential Risk Factors of Hypokalemia in Pediatric Patients With Diabetic KetoacidosisDocument2 pagesPrevalence and Potential Risk Factors of Hypokalemia in Pediatric Patients With Diabetic KetoacidosisAti Rahmi PurwandariNo ratings yet
- Amsterdam Placental WorkshopDocument16 pagesAmsterdam Placental WorkshopCarlos Andrés Sánchez RuedaNo ratings yet
- 2 Mod Issue Brief Finalupdatedlogo Policy Oct2017 SMDocument2 pages2 Mod Issue Brief Finalupdatedlogo Policy Oct2017 SMJohnryl FranciscoNo ratings yet
- Evidence-Based Medicine For Obstetrics and Gynecology: Life Sciences LibraryDocument38 pagesEvidence-Based Medicine For Obstetrics and Gynecology: Life Sciences LibraryValeria EvtodievNo ratings yet
- ApheresisDocument18 pagesApheresisOanamikaela VaidaNo ratings yet
- 393 FullDocument7 pages393 FullmochkurniawanNo ratings yet
- Maki-2020-Perspective - Laboratory ConsiderationDocument13 pagesMaki-2020-Perspective - Laboratory ConsiderationKun Aristiati SusiloretniNo ratings yet
- Recommendations For Neonatal JaundiceDocument23 pagesRecommendations For Neonatal JaundiceYatin MehtaNo ratings yet
- Evidence Based Medicine in Neonatology: DefinitionDocument6 pagesEvidence Based Medicine in Neonatology: DefinitionAhmedAOmarNo ratings yet
- Management of The Undescended Testis in ChildrenDocument16 pagesManagement of The Undescended Testis in ChildrenRashmeeta ThadhaniNo ratings yet
- Presentation 3Document3 pagesPresentation 3MUHAMMAD09No ratings yet
- Summer 23Document11 pagesSummer 23MUHAMMAD09No ratings yet
- 2004 Book GhrelinDocument259 pages2004 Book GhrelinMUHAMMAD09No ratings yet
- WJG 23 6137Document16 pagesWJG 23 6137MUHAMMAD09No ratings yet
- JBDS 01 Hypo Algorithm January 2023Document1 pageJBDS 01 Hypo Algorithm January 2023MUHAMMAD09No ratings yet
- Nej MR A 2214617Document5 pagesNej MR A 2214617MUHAMMAD09No ratings yet
- MiniCEX Form 2Document1 pageMiniCEX Form 2MUHAMMAD09No ratings yet
- Webex WebcastDocument1 pageWebex WebcastMUHAMMAD09No ratings yet
- DaR Guidelines 2021 Full WebDocument333 pagesDaR Guidelines 2021 Full WebFransisca PekertiNo ratings yet
- Diagnosis and Management of Hyperglycemic Crises: DKA and HHSDocument82 pagesDiagnosis and Management of Hyperglycemic Crises: DKA and HHSArini Dwi NastitiNo ratings yet
- Nelson's Pediatric Antimicrobial PDFDocument331 pagesNelson's Pediatric Antimicrobial PDFMADHANKUMAR MANICKAVELNo ratings yet
- Voices: The Novel Coronavirus Outbreak: What We Know and What We Don'tDocument3 pagesVoices: The Novel Coronavirus Outbreak: What We Know and What We Don'tMUHAMMAD09No ratings yet
- GwBXq5xPwIpxRnMzneDu1603346193 2Document40 pagesGwBXq5xPwIpxRnMzneDu1603346193 2MUHAMMAD09No ratings yet
- Acute Intermittent Porphyria: The Right Clinical Information, Right Where It's NeededDocument29 pagesAcute Intermittent Porphyria: The Right Clinical Information, Right Where It's NeededMUHAMMAD09No ratings yet
- History Taking As A Diagnostic Test in Patients With Syncope: Developing Expertise in SyncopeDocument4 pagesHistory Taking As A Diagnostic Test in Patients With Syncope: Developing Expertise in SyncopeMUHAMMAD09No ratings yet
- Bowel Problems: The Bowel: What It Is, What It DoesDocument9 pagesBowel Problems: The Bowel: What It Is, What It DoesMUHAMMAD09No ratings yet
- Waykar Ali PDFDocument12 pagesWaykar Ali PDFMUHAMMAD09No ratings yet
- Waykar Ali PDFDocument12 pagesWaykar Ali PDFMUHAMMAD09No ratings yet
- ENDOCRINE PRACTICE Rapid Electronic Article in Press: AACE/ACE Consensus StatementDocument66 pagesENDOCRINE PRACTICE Rapid Electronic Article in Press: AACE/ACE Consensus StatementMUHAMMAD09No ratings yet
- Sca PDFDocument58 pagesSca PDFMUHAMMAD09No ratings yet
- Cerebral Venous Thrombosis-Treatment & PrognosisDocument37 pagesCerebral Venous Thrombosis-Treatment & PrognosisMUHAMMAD09No ratings yet
- The Honey BeeDocument5 pagesThe Honey BeeMUHAMMAD09No ratings yet
- Umar e Sani Qadam Ba Qadam by Abdullah FaraniDocument201 pagesUmar e Sani Qadam Ba Qadam by Abdullah Faraniawais2464753No ratings yet
- Aace Algorithm SlidesDocument11 pagesAace Algorithm SlidesMUHAMMAD09No ratings yet
- 10 Rules For Being A Great ModeratorDocument3 pages10 Rules For Being A Great ModeratorMUHAMMAD09No ratings yet
- 06 Oa Prevalence of Peripheral PDFDocument5 pages06 Oa Prevalence of Peripheral PDFMUHAMMAD09No ratings yet
- cd17-0119 FullDocument24 pagescd17-0119 FullMUHAMMAD09No ratings yet
- 2010 Endo & Diabetes (Amendment 2012)Document62 pages2010 Endo & Diabetes (Amendment 2012)MUHAMMAD09No ratings yet
- Atlas of Islamic Victories 02 in UrduDocument256 pagesAtlas of Islamic Victories 02 in UrduMUHAMMAD09No ratings yet
- Rg213 Rgflex Coax Braided Cable: Product Data Sheet RG213-50JFDocument1 pageRg213 Rgflex Coax Braided Cable: Product Data Sheet RG213-50JFPancho BerríosNo ratings yet
- Twingo 3 & Clio 4Document10 pagesTwingo 3 & Clio 4Alexandre Le GrandNo ratings yet
- All Creatures Great and SmallDocument4 pagesAll Creatures Great and SmallsaanviranjanNo ratings yet
- RTR Piping Inspection GuideDocument17 pagesRTR Piping Inspection GuideFlorante NoblezaNo ratings yet
- Nigeria Emergency Plan NemanigeriaDocument47 pagesNigeria Emergency Plan NemanigeriaJasmine Daisy100% (1)
- FIL M 216 2nd Yer Panitikan NG PilipinasDocument10 pagesFIL M 216 2nd Yer Panitikan NG PilipinasJunas LopezNo ratings yet
- Analects of A.T. Still-Nature Quotes-UnboundedDocument8 pagesAnalects of A.T. Still-Nature Quotes-UnboundedBruno OliveiraNo ratings yet
- Cebuano LanguageDocument15 pagesCebuano LanguageIsla PageNo ratings yet
- Olt CliDocument2 pagesOlt CliMohammad SaeedNo ratings yet
- Natural GasDocument86 pagesNatural GasNikhil TiwariNo ratings yet
- Inventario de Autoestima de Coopersmith PDFDocument10 pagesInventario de Autoestima de Coopersmith PDFNancy BerduzcoNo ratings yet
- CBK Test QuestionsDocument2 pagesCBK Test QuestionsMehul GuptaNo ratings yet
- Gartner CRM Handbook FinalDocument0 pagesGartner CRM Handbook FinalghanshyamdassNo ratings yet
- Atomic Structure QuestionsDocument1 pageAtomic Structure QuestionsJames MungallNo ratings yet
- Divisional Chart-IDocument1 pageDivisional Chart-Iabhisek1987No ratings yet
- Technical Information System Overview Prosafe-Com 3.00 Prosafe-ComDocument49 pagesTechnical Information System Overview Prosafe-Com 3.00 Prosafe-Comshekoofe danaNo ratings yet
- 2.2valves, Alarm - Ul Product IqDocument1 page2.2valves, Alarm - Ul Product Iqbhima irabattiNo ratings yet
- Science MELCsDocument42 pagesScience MELCsRanjell Allain TorresNo ratings yet
- INSYS - EBW Serie EbookDocument4 pagesINSYS - EBW Serie EbookJorge_Andril_5370No ratings yet
- Determination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Document11 pagesDetermination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Geovas GomezNo ratings yet
- VIP 32 Hybrid VentDocument8 pagesVIP 32 Hybrid VentsagarNo ratings yet
- 2iccas2005 Paper 377Document5 pages2iccas2005 Paper 377Cristian BandilaNo ratings yet
- Reporte Corporativo de Louis Dreyfus Company (LDC)Document21 pagesReporte Corporativo de Louis Dreyfus Company (LDC)OjoPúblico Periodismo de InvestigaciónNo ratings yet
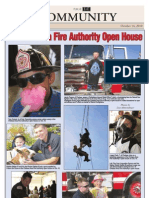
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- Application of Gis in Electrical Distribution Network SystemDocument16 pagesApplication of Gis in Electrical Distribution Network SystemMelese Sefiw100% (1)
- Villanueva Poetry Analysis Template BSEE 35Document7 pagesVillanueva Poetry Analysis Template BSEE 35CHRISTIAN MAHINAYNo ratings yet
- IEC61508 GuideDocument11 pagesIEC61508 Guidesrbehera1987No ratings yet