You might also like
- Marik Covid Protocol Summary PDFDocument2 pagesMarik Covid Protocol Summary PDFJody VivasNo ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol SummaryInternos YopalNo ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol Summaryshubham rathodNo ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol SummaryCamille05No ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol SummaryCaterina PrepelitaNo ratings yet
- Marik Covid Protocol Summary PDFDocument1 pageMarik Covid Protocol Summary PDFCiuvat Dumitru ValentinNo ratings yet
- FRONT LINE COVID-19 CRITICAL CARE ALLIANCE HOSPITAL TREATMENT PROTOCOLDocument2 pagesFRONT LINE COVID-19 CRITICAL CARE ALLIANCE HOSPITAL TREATMENT PROTOCOLBhanu Kumar100% (1)
- Hospital Treatment Protocol For Covid-19Document4 pagesHospital Treatment Protocol For Covid-19Adrian BoboceaNo ratings yet
- CCF IpDocument1 pageCCF IpBryan FjbNo ratings yet
- Hospital Treatment Protocol For Covid-19Document2 pagesHospital Treatment Protocol For Covid-19Nandor KissNo ratings yet
- FRONT LINE COVID-19 CRITICAL CARE ALLIANCE PROTOCOLSDocument2 pagesFRONT LINE COVID-19 CRITICAL CARE ALLIANCE PROTOCOLSCornel ComanNo ratings yet
- Farma StrokeDocument37 pagesFarma StrokeDAHLIANo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHDavid GrayNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHJhonn BlackNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHfernandohNo ratings yet
- COVID MX BsmmuDocument2 pagesCOVID MX BsmmuNuhiat NahreenNo ratings yet
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
- Spinal Cord CompressionDocument4 pagesSpinal Cord Compressionian3yeung-2No ratings yet
- MX Protocol Book FinalDocument42 pagesMX Protocol Book FinalPawan ChoudharyNo ratings yet
- Amiodarone Mechanism, Uses, Dosing & MonitoringDocument10 pagesAmiodarone Mechanism, Uses, Dosing & MonitoringsarahhhNo ratings yet
- Revised COVID 19 SARS-COV2 Treatment Protocol - FinalDocument6 pagesRevised COVID 19 SARS-COV2 Treatment Protocol - FinalupsahuNo ratings yet
- STEMI NotesDocument8 pagesSTEMI NotesIzzul HafiyNo ratings yet
- VTE-Prophylaxis-Protocol - MOHDocument13 pagesVTE-Prophylaxis-Protocol - MOHreham ONo ratings yet
- Antibiotic hospital manDocument1 pageAntibiotic hospital manarshiya.manasekiNo ratings yet
- Clinical Cases Pharmacology PDFDocument7 pagesClinical Cases Pharmacology PDFAnkur HazraNo ratings yet
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- ACLS Algorithms Adult 2010Document12 pagesACLS Algorithms Adult 2010anon_336736395No ratings yet
- Lab 11 AntianginalDocument4 pagesLab 11 AntianginalanaNo ratings yet
- Anti-Anginal DrugsDocument39 pagesAnti-Anginal Drugspoonam rana100% (1)
- ANTI-ARRHYTHMIC DRUGS Veterinary PharmacologyDocument5 pagesANTI-ARRHYTHMIC DRUGS Veterinary PharmacologyljramosNo ratings yet
- Medical TherapyDocument6 pagesMedical Therapyvinay reddyNo ratings yet
- Anticoagulation strategies for COVID-19 patients at BMCDocument1 pageAnticoagulation strategies for COVID-19 patients at BMCAvinash KumbharNo ratings yet
- Nitrates andDocument61 pagesNitrates andMrunalini DandamudiNo ratings yet
- Atrial Fibrillation TDDocument6 pagesAtrial Fibrillation TDapi-594366475No ratings yet
- COVID-19 Protocol by EVMSDocument13 pagesCOVID-19 Protocol by EVMSKrishnamurthi CG100% (1)
- EVMS Critical Care COVID-19 ProtocolDocument17 pagesEVMS Critical Care COVID-19 ProtocolInternos YopalNo ratings yet
- Medication Administration PolicyDocument76 pagesMedication Administration PolicyJully GaciasNo ratings yet
- Treatment Protocol Covid-19Document4 pagesTreatment Protocol Covid-19Shiv singhNo ratings yet
- Mild Moderate Severe Clinical Criteria: Covid ProtocolDocument4 pagesMild Moderate Severe Clinical Criteria: Covid ProtocolSiaNo ratings yet
- Acls Algorithms 2012Document12 pagesAcls Algorithms 2012kivuNo ratings yet
- LBL DoneDocument6 pagesLBL DoneShoaib KhatikNo ratings yet
- Drugs in PregnancyDocument40 pagesDrugs in PregnancyhkkanhaNo ratings yet
- Hypertensive Urgency EmergencyDocument5 pagesHypertensive Urgency Emergencydamondouglas100% (3)
- Master Drug ChartDocument22 pagesMaster Drug ChartMahadhir AkmalNo ratings yet
- CMSCN R IgevDocument2 pagesCMSCN R Igevdiana8827534No ratings yet
- Drugs Study Neh Jai2xDocument10 pagesDrugs Study Neh Jai2xjai2xNo ratings yet
- Icu Adult and PaedsDocument2 pagesIcu Adult and PaedsPrashin RocharamNo ratings yet
- Drugs requiring loading dosesDocument1 pageDrugs requiring loading dosesandirio7486No ratings yet
- Suspected COVID-19 Cases Management in Triage HospitalsDocument6 pagesSuspected COVID-19 Cases Management in Triage HospitalsMuhamed RamadanNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- Medad TeamDocument18 pagesMedad TeamAxmed MaxamedNo ratings yet
- Routine Anesthesia Set UpDocument4 pagesRoutine Anesthesia Set UpSteve Johnstone100% (2)
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Pediatric Dosage CalculationsDocument5 pagesPediatric Dosage CalculationsLovely Anjenell MacalingaNo ratings yet
- Finding A Good Essay QuestionDocument1 pageFinding A Good Essay QuestionelasticemperorNo ratings yet
- Live Within Your Window of ToleranceDocument19 pagesLive Within Your Window of Toleranceelasticemperor0% (1)
- Call For Papers 2019-2020 PDFDocument5 pagesCall For Papers 2019-2020 PDFelasticemperorNo ratings yet
- Planning Toolkit for Gendered Violence PreventionDocument14 pagesPlanning Toolkit for Gendered Violence PreventionelasticemperorNo ratings yet
- The 22 Convention Make Women Great Again™ PDFDocument1 pageThe 22 Convention Make Women Great Again™ PDFelasticemperorNo ratings yet
- FREEZEABLE MEALS UNDER 40 CHARACTERSDocument20 pagesFREEZEABLE MEALS UNDER 40 CHARACTERSelasticemperorNo ratings yet
- Exeter Learning Environment: Getting Started WithDocument32 pagesExeter Learning Environment: Getting Started WithelasticemperorNo ratings yet
- Coronavirus - Fight for Socialist Alternative and Workers' RightsDocument2 pagesCoronavirus - Fight for Socialist Alternative and Workers' RightselasticemperorNo ratings yet
- small axe journal explores caribbean thoughtDocument16 pagessmall axe journal explores caribbean thoughtelasticemperorNo ratings yet
- Pay As Little As: Savings ProgramDocument1 pagePay As Little As: Savings ProgramelasticemperorNo ratings yet
- 2020 Strike Handbook For UCU ActivistsDocument32 pages2020 Strike Handbook For UCU ActivistselasticemperorNo ratings yet
- FREEZEABLE MEALS UNDER 40 CHARACTERSDocument20 pagesFREEZEABLE MEALS UNDER 40 CHARACTERSelasticemperorNo ratings yet
- Mari Fitness Home Guide PDFDocument30 pagesMari Fitness Home Guide PDFviva100% (1)
- Live Within Your Window of ToleranceDocument19 pagesLive Within Your Window of Toleranceelasticemperor0% (1)
- Yoga London Pose NotesDocument19 pagesYoga London Pose NoteselasticemperorNo ratings yet
- Planning Toolkit for Gendered Violence PreventionDocument14 pagesPlanning Toolkit for Gendered Violence PreventionelasticemperorNo ratings yet
- Coding deCoding class insightsDocument18 pagesCoding deCoding class insightsShalabh Vikram SahuNo ratings yet
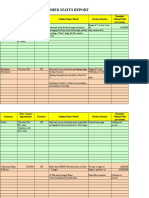
- Customer Status Update Report 27th January 2015 ColourDocument20 pagesCustomer Status Update Report 27th January 2015 ColourmaryNo ratings yet
- Sap GlossaryDocument324 pagesSap GlossaryNikos TataliasNo ratings yet
- 04powertrain 1010Document8 pages04powertrain 1010francis_15inNo ratings yet
- The DriversDocument277 pagesThe DriversADENIKE JOHNSONNo ratings yet
- CIE Master 2022 (New Master Programme) ENDocument171 pagesCIE Master 2022 (New Master Programme) ENZar MaghustNo ratings yet
- Loveology: God. Love. Marriage. Sex. and The Never-Ending Story of Male and Female. by John Mark Comer, SamplerDocument32 pagesLoveology: God. Love. Marriage. Sex. and The Never-Ending Story of Male and Female. by John Mark Comer, SamplerZondervan40% (5)
- Budha Dal Aarti Aarta FULLDocument1 pageBudha Dal Aarti Aarta FULLVishal Singh100% (1)
- Important Characteristics of an Ideal InductorDocument4 pagesImportant Characteristics of an Ideal Inductorsreekantha reddyNo ratings yet
- Colossians 1Document1 pageColossians 1aries john mendrezNo ratings yet
- Mental Health Awareness and PFA Training ReportDocument4 pagesMental Health Awareness and PFA Training ReportSHEILA MAE PERTIMOS100% (14)
- NES 362 Type and Production Testing of Mechanical Equipment Category 3Document36 pagesNES 362 Type and Production Testing of Mechanical Equipment Category 3JEORJENo ratings yet
- Early strength predicts long-term performance of asphalt cold mixesDocument7 pagesEarly strength predicts long-term performance of asphalt cold mixesMonu GhadwalNo ratings yet
- Palm Kernel Reinforced Composites for Brake Pad ApplicationsDocument18 pagesPalm Kernel Reinforced Composites for Brake Pad ApplicationsSachin SukumaranNo ratings yet
- Solar/Wind/Diesel Hybrid Energy System With Battery Storage For Rural ElectrificationDocument15 pagesSolar/Wind/Diesel Hybrid Energy System With Battery Storage For Rural ElectrificationWelde AynaleNo ratings yet
- Siemens: Building A Structure To Drive Performance and Responsibility - CaseDocument6 pagesSiemens: Building A Structure To Drive Performance and Responsibility - CaseBitopan SonowalNo ratings yet
- Logistic Growth Rate Functions Blumberg1968Document3 pagesLogistic Growth Rate Functions Blumberg1968Jonnathan RamirezNo ratings yet
- Galloway 1989 Genetic Stratigraphic Sequence Basin Analysis IDocument18 pagesGalloway 1989 Genetic Stratigraphic Sequence Basin Analysis IMitreNo ratings yet
- Energy Performance of Hot, DryDocument128 pagesEnergy Performance of Hot, DrySrinu ReddyNo ratings yet
- Macalloy Corporate Brochure September 2018 LR PDFDocument12 pagesMacalloy Corporate Brochure September 2018 LR PDFsampathkumarNo ratings yet
- PHL Ad 17 01 Operationalguidance 2017 Eng Ops Manual Adolescent Health Development ProgramDocument111 pagesPHL Ad 17 01 Operationalguidance 2017 Eng Ops Manual Adolescent Health Development ProgramJoanne G Haw GetidaNo ratings yet
- Mystic Mystique Face Reading-IIDocument10 pagesMystic Mystique Face Reading-IIVijay KumarNo ratings yet
- Acc Gr11 May 2009 PaperDocument13 pagesAcc Gr11 May 2009 PaperSam ChristieNo ratings yet
- Akali NihangsDocument19 pagesAkali NihangsAngad YuvrajNo ratings yet
- 2Tafseer2019Sep4 17 24oc1 8 29nov5 262020jan7 21F11 18 25Document96 pages2Tafseer2019Sep4 17 24oc1 8 29nov5 262020jan7 21F11 18 25Aroob YaseenNo ratings yet
- JuliadatascienceDocument214 pagesJuliadatascienceFulvio JoséNo ratings yet
- Philippine School Action Plan for Scouting ProgramDocument1 pagePhilippine School Action Plan for Scouting ProgramLaira Joy Salvador - ViernesNo ratings yet
- Cbs BookDocument294 pagesCbs Bookadmiralninja100% (1)
- Mechanics of Solids by Sadhu Singhpdf Ebook and Ma PDFDocument1 pageMechanics of Solids by Sadhu Singhpdf Ebook and Ma PDFNeeraj Janghu0% (2)
- Physics Universe ModelsDocument14 pagesPhysics Universe ModelsTracy zorca50% (2)