You might also like
- Abc Lec NotesDocument5 pagesAbc Lec NoteshanhananicasNo ratings yet
- ARDS (Acute Respiratory Distress Syndrome) : EarlyDocument1 pageARDS (Acute Respiratory Distress Syndrome) : EarlyDora Elena HurtadoNo ratings yet
- Biologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManDocument162 pagesBiologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManLex CatNo ratings yet
- Resp 180214084710Document72 pagesResp 180214084710Karla Geraldine Carhuas VeliNo ratings yet
- Pulmonary First Aid GuideDocument6 pagesPulmonary First Aid GuideMAINo ratings yet
- Mitral StenosisDocument2 pagesMitral StenosisitsmailbbkNo ratings yet
- Acute Respiratory Distress Syndrome by Mr. Ashish RoyDocument45 pagesAcute Respiratory Distress Syndrome by Mr. Ashish RoySyedzulqurnainhussainshah ZulqurnainNo ratings yet
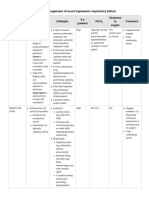
- Acute Respiratory Failure Concept MapDocument1 pageAcute Respiratory Failure Concept Mapjenievysenerez100% (1)
- Notes: Generally, What Is It?Document11 pagesNotes: Generally, What Is It?long gogoNo ratings yet
- Altitude Diving PhysiologyDocument12 pagesAltitude Diving PhysiologyKarin Gandeswari100% (1)
- CN 118 - Lecture ReviewerDocument20 pagesCN 118 - Lecture ReviewerCamille SanguyoNo ratings yet
- Chronic Bronchitis and EmphesemaDocument2 pagesChronic Bronchitis and Emphesemanursing concept maps100% (2)
- Cor Pulmonale PATHOPHYSIOLOGYDocument2 pagesCor Pulmonale PATHOPHYSIOLOGYChloie Marie RosalejosNo ratings yet
- Pathophysiology and Nursing Care Plan for Cor PulmonaleDocument6 pagesPathophysiology and Nursing Care Plan for Cor PulmonaleMonette Abalos MendovaNo ratings yet
- Pathophysiology DyspneaDocument1 pagePathophysiology DyspneaJoseph LimNo ratings yet
- Ass Q ArdsDocument1 pageAss Q ArdsKristine MendozaNo ratings yet
- Hospital Acquired Pneumonia PathophysiologyDocument5 pagesHospital Acquired Pneumonia PathophysiologyKAYCEENo ratings yet
- Toronto Notes Respirology PDFDocument40 pagesToronto Notes Respirology PDFJaya Semara Putra67% (3)
- Asma 1Document8 pagesAsma 1punkgatitNo ratings yet
- 2023 UsDocument10 pages2023 UswisgeorgekwokNo ratings yet
- Diagnostic Diferential Medicina InternaDocument6 pagesDiagnostic Diferential Medicina InternaLary ArNo ratings yet
- High Risk Conditionof of NewbornDocument2 pagesHigh Risk Conditionof of NewbornstephanyNo ratings yet
- NURS 19 Pulmonary Edema, Hemorrhage, Cardiac Arrest Midterm ExamDocument6 pagesNURS 19 Pulmonary Edema, Hemorrhage, Cardiac Arrest Midterm ExamSN BundleNo ratings yet
- Table 17-1 - Indications For Endotracheal Intubation in CriticDocument1 pageTable 17-1 - Indications For Endotracheal Intubation in CriticDragutin PetrićNo ratings yet
- Acute Respiratory FailureDocument2 pagesAcute Respiratory FailureKaja MatovinovicNo ratings yet
- Dyspnea - DR AllenDocument50 pagesDyspnea - DR AllenalmiraerickaiNo ratings yet
- Concept MapDocument5 pagesConcept Mapmild_tea100% (1)
- ACC Jimmy AsafDocument152 pagesACC Jimmy AsafFikriYTNo ratings yet
- Group 1 6 Problem Emergency Medicine Block Monday, 30 Oct 2017Document121 pagesGroup 1 6 Problem Emergency Medicine Block Monday, 30 Oct 2017Jonathan TandajuNo ratings yet
- Myocardial Concept MappingDocument34 pagesMyocardial Concept MappingTHIRD YEARNo ratings yet
- ch28 Notes Part 2Document9 pagesch28 Notes Part 2Monica JubaneNo ratings yet
- It 14 ArdsDocument58 pagesIt 14 ArdsMohamad Fiqih ArrachmanNo ratings yet
- Cute Respiratory Distress Syndrome Ards: Guide - DR - Shiv.S.Sharma - Dr.Y. JamraDocument40 pagesCute Respiratory Distress Syndrome Ards: Guide - DR - Shiv.S.Sharma - Dr.Y. JamraandenaNo ratings yet
- Approach To DyspneaDocument9 pagesApproach To DyspneaMuhammad LukmanNo ratings yet
- RespiratoryDocument161 pagesRespiratoryDanity_Anne_Ba_1326100% (1)
- IADVL Color Atlas of Dermatopathology - BookDocument41 pagesIADVL Color Atlas of Dermatopathology - Book65gkenNo ratings yet
- Road To MEmMedDocument12 pagesRoad To MEmMedWinnie WongNo ratings yet
- Congenital Heart DiseasesDocument1 pageCongenital Heart DiseasesEmily AnnNo ratings yet
- Paediatric Respiratory Assessment Cheat SheetDocument1 pagePaediatric Respiratory Assessment Cheat SheetReihann N. EdresNo ratings yet
- Sindromatologi DyspneuDocument18 pagesSindromatologi DyspneuMeylan TaebenuNo ratings yet
- Community-Acquired PneumoniaDocument22 pagesCommunity-Acquired PneumoniaIMAFDNo ratings yet
- Maternal Cardiac ArrestDocument28 pagesMaternal Cardiac ArrestTruelly ChanantaNo ratings yet
- Assignment#1Document13 pagesAssignment#1Mark Jefferson LunaNo ratings yet
- Pathophysiology of Atrial Septal DefectDocument2 pagesPathophysiology of Atrial Septal Defectbobtaguba50% (2)
- IM-Heart Failure Concept MapDocument16 pagesIM-Heart Failure Concept MapTrisNo ratings yet
- Patent Ductus Arteriosus 6. Aortic Stenosis: Signs and Symptoms: Signs and SymptomsDocument3 pagesPatent Ductus Arteriosus 6. Aortic Stenosis: Signs and Symptoms: Signs and SymptomsKIANA LOUISE ROMANONo ratings yet
- Supplementary Material 1c Acute Respiratory FailureDocument5 pagesSupplementary Material 1c Acute Respiratory FailureJanela Chriselle B. TICARNo ratings yet
- NCM 112-Mod3Document19 pagesNCM 112-Mod3Samantha BolanteNo ratings yet
- Hypoxemia 2Document3 pagesHypoxemia 2ganganakulan.nagavallyNo ratings yet
- M V ICU: Echanical Entilation INDocument82 pagesM V ICU: Echanical Entilation INabhilashreddy45No ratings yet
- Breathlessness: Causes, Evaluation and ManagementDocument10 pagesBreathlessness: Causes, Evaluation and ManagementAckNo ratings yet
- Pathophysiology of PneumoniaDocument1 pagePathophysiology of PneumoniaJeffrey RamosNo ratings yet
- NCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSDocument4 pagesNCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSViviene Faye FombuenaNo ratings yet
- A. WOC Acute Lungs Oedem.: Gangguan Perfusi JaringanDocument1 pageA. WOC Acute Lungs Oedem.: Gangguan Perfusi Jaringanrizki vitaNo ratings yet
- SARS PathophysioDocument2 pagesSARS PathophysioLouise BravoNo ratings yet
- Step 2 CK Uworld Pulmonary NotesDocument42 pagesStep 2 CK Uworld Pulmonary NotesMariyam Nauffer100% (8)
- Asphyxial Death: Yoni SyukrianiDocument30 pagesAsphyxial Death: Yoni SyukrianinrahmaNo ratings yet
- Acute Respiratory Distress SyndromeDocument47 pagesAcute Respiratory Distress Syndromemaeliszxc kimNo ratings yet
- DyspneaDocument21 pagesDyspneaMahboob AlamNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- RAJAL FIX Maret 23Document22 pagesRAJAL FIX Maret 23Julyan ValenzaNo ratings yet
- Bubble CPAP Effectiveness Preterm Neonates RDSDocument4 pagesBubble CPAP Effectiveness Preterm Neonates RDSJulyan ValenzaNo ratings yet
- Aromatherapy's Effect on Nausea in PregnancyDocument9 pagesAromatherapy's Effect on Nausea in PregnancyJulyan ValenzaNo ratings yet
- Kelompok Experimen: FrequenciesDocument13 pagesKelompok Experimen: FrequenciesJulyan ValenzaNo ratings yet
- Page NumberDocument18 pagesPage NumberJulyan ValenzaNo ratings yet
- Page NumberDocument18 pagesPage NumberJulyan ValenzaNo ratings yet
- Chest.126.2.592 MBE EN UCIDocument9 pagesChest.126.2.592 MBE EN UCIJaime RomeroNo ratings yet
- Clincal Case Presentation 5Document32 pagesClincal Case Presentation 5api-635948254No ratings yet
- Federal Democratic Republic of Ethiopia Ministry of HealthDocument43 pagesFederal Democratic Republic of Ethiopia Ministry of HealthdagemNo ratings yet
- Acute Respiratory Distress Syndrome: By: Ben Meron MichalDocument13 pagesAcute Respiratory Distress Syndrome: By: Ben Meron Michalmichal ben meronNo ratings yet
- (Draeger) DYK Infographic - Recruitment Maneuvers (Sustained Inflation - 40 by 40) en (2023)Document1 page(Draeger) DYK Infographic - Recruitment Maneuvers (Sustained Inflation - 40 by 40) en (2023)ConstantineSemenchukNo ratings yet
- N-Acetylcysteine May Improve Lung RecoveryDocument5 pagesN-Acetylcysteine May Improve Lung Recoveryanisa rachmitaNo ratings yet
- Systemic Effects of Perinatal AsphyxiaDocument10 pagesSystemic Effects of Perinatal AsphyxiaJaner Banos100% (1)
- Pronation Therapy: DR Ahmed Abdelhady MD Critical Care ICU ConsultantDocument30 pagesPronation Therapy: DR Ahmed Abdelhady MD Critical Care ICU Consultantlayla alyamiNo ratings yet
- Respi-Nclex QuestionsDocument160 pagesRespi-Nclex QuestionsSophia Rose Delos Santos100% (3)
- Acute Respiratory Distress SyndromeDocument9 pagesAcute Respiratory Distress SyndromeAgnes Jeane EnriquezNo ratings yet
- Mendelson's SyndromeDocument17 pagesMendelson's SyndromeYuvetha IndranNo ratings yet
- Fracturas TraumaDocument8 pagesFracturas Traumajoseaugustorojas9414No ratings yet
- Airway Pressure Release VentilationDocument31 pagesAirway Pressure Release VentilationsakuraleeshaoranNo ratings yet
- Acute Respiratory Failure Lesson PlanDocument6 pagesAcute Respiratory Failure Lesson Planshweta singhNo ratings yet
- Artificial OrgansDocument184 pagesArtificial OrganshemavathyrajasekaranNo ratings yet
- Oxygen Sepsis PDFDocument3 pagesOxygen Sepsis PDFdimas antaraNo ratings yet
- Automation of Mechanical VentilationDocument12 pagesAutomation of Mechanical VentilationjuanNo ratings yet
- Pulmonary and Critical Care MnemonicsDocument10 pagesPulmonary and Critical Care MnemonicsnmahpbooksNo ratings yet
- Ped&neo&mec&ven&khi&2 NDDocument309 pagesPed&neo&mec&ven&khi&2 NDJose CastellonNo ratings yet
- DiagnosisDocument12 pagesDiagnosisHCX dghhqNo ratings yet
- Ecografia Toracica PDFDocument12 pagesEcografia Toracica PDFCristinaLucanNo ratings yet
- Critical Care Nursing Notes 1Document10 pagesCritical Care Nursing Notes 1pauchanmnlNo ratings yet
- Neurological Impact of Coronavirus Disease, Practical Considerations For The Neuroscience CommunityDocument33 pagesNeurological Impact of Coronavirus Disease, Practical Considerations For The Neuroscience CommunityArtur Cordeiro100% (1)
- 2nd Research Proposal March 10 2023 EditDocument22 pages2nd Research Proposal March 10 2023 EditChristly CallenoNo ratings yet
- Journal of Clinical MedicineDocument12 pagesJournal of Clinical MedicineGonzalo Gobbi100% (1)
- 10) Dyspnea Nov 2016 PDFDocument99 pages10) Dyspnea Nov 2016 PDFGopala HariNo ratings yet
- Nutrion in Critical CareDocument264 pagesNutrion in Critical CareQuique RomeroNo ratings yet
- Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryDocument16 pagesGian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryGian Carlo RabagoNo ratings yet
- Critical Care Clinics - Mechanical VentilationDocument218 pagesCritical Care Clinics - Mechanical VentilationMohsin Damudi100% (6)
- Ventilator Management: Introduction To Ventilator Management, Modes of Mechanical Ventilation, Methods of Ventilatory SupportDocument12 pagesVentilator Management: Introduction To Ventilator Management, Modes of Mechanical Ventilation, Methods of Ventilatory SupportDellNo ratings yet