You might also like
- It 14 ArdsDocument58 pagesIt 14 ArdsMohamad Fiqih ArrachmanNo ratings yet
- Notes SC RSDocument5 pagesNotes SC RS202213No ratings yet
- Resp 180214084710Document72 pagesResp 180214084710Karla Geraldine Carhuas VeliNo ratings yet
- Respiratory EmergenciesDocument21 pagesRespiratory EmergenciesMohamed Anas SayedNo ratings yet
- Sindromatologi DyspneuDocument18 pagesSindromatologi DyspneuMeylan TaebenuNo ratings yet
- Respiratory PathologyDocument42 pagesRespiratory PathologyMorgan PeggNo ratings yet
- Acute Respiratory Distress SyndromeDocument47 pagesAcute Respiratory Distress Syndromemaeliszxc kimNo ratings yet
- Acute Respiratory Failure Concept MapDocument1 pageAcute Respiratory Failure Concept Mapjenievysenerez100% (1)
- COPD: Chronic Obstructive Pulmonary Disease ExplainedDocument15 pagesCOPD: Chronic Obstructive Pulmonary Disease ExplainedMary Grace AgataNo ratings yet
- M V ICU: Echanical Entilation INDocument82 pagesM V ICU: Echanical Entilation INabhilashreddy45No ratings yet
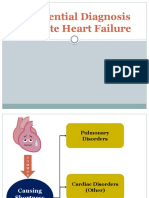
- LI 8 - Differential Diagnosis of Acute Heart FailureDocument11 pagesLI 8 - Differential Diagnosis of Acute Heart Failure19-034 Jefry Junaidi PurbaNo ratings yet
- Articulo Parcial 1 Urgencias Respiratorias Perros y GatosDocument23 pagesArticulo Parcial 1 Urgencias Respiratorias Perros y GatosYara Valentina Toledo ManriqueNo ratings yet
- Anestesia y Analgesia BSAVA-319-341Document23 pagesAnestesia y Analgesia BSAVA-319-341angel.mendozaNo ratings yet
- ACUTE RESPIRATORY DISTRESS SYNDROME by Dr. Monday ZaccheausDocument59 pagesACUTE RESPIRATORY DISTRESS SYNDROME by Dr. Monday ZaccheausDr. Amb. Monday ZaccheausNo ratings yet
- Respiratory Failure: by Amera GumamaDocument26 pagesRespiratory Failure: by Amera GumamaGumama AmeiyrhaNo ratings yet
- Progressive Dyspnea and A Persistentwheeze A Subtle Presentation of Pulmonary Embolism in A 64 Year 6856Document3 pagesProgressive Dyspnea and A Persistentwheeze A Subtle Presentation of Pulmonary Embolism in A 64 Year 6856Sophia RoseNo ratings yet
- RespiratoryDocument161 pagesRespiratoryDanity_Anne_Ba_1326100% (1)
- Medical Emergencies FlashcardsDocument109 pagesMedical Emergencies Flashcardsmkct111No ratings yet
- ARDSDocument24 pagesARDSMuhammad NurmanNo ratings yet
- NCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSDocument4 pagesNCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSViviene Faye FombuenaNo ratings yet
- Respiratory Disorders & TB in Children (Part I and Ii) - Dr. MendozaDocument17 pagesRespiratory Disorders & TB in Children (Part I and Ii) - Dr. MendozaRea Dominique CabanillaNo ratings yet
- Maternal Cardiac ArrestDocument28 pagesMaternal Cardiac ArrestTruelly ChanantaNo ratings yet
- Respiratory Pathology: Dr. Okon MRCSDocument38 pagesRespiratory Pathology: Dr. Okon MRCSEdwin OkonNo ratings yet
- The System: RespiDocument219 pagesThe System: Respilalaine22dale100% (1)
- Neonatal respiratory distress causesDocument4 pagesNeonatal respiratory distress causesseno adiNo ratings yet
- Differentiating Bronchiolitis and PneumoniaDocument17 pagesDifferentiating Bronchiolitis and PneumoniaRizky DarmawanNo ratings yet
- Management of Respiratory EmergencyDocument17 pagesManagement of Respiratory EmergencyVictor BeranNo ratings yet
- Pulmonary Edema: Moderator - Asso Prof DR Arun Kumar Presentor - DR Kannan GDocument39 pagesPulmonary Edema: Moderator - Asso Prof DR Arun Kumar Presentor - DR Kannan GGrace JasminNo ratings yet
- Approach To A Child With Cough and Difficulty in BreathingDocument23 pagesApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Cor Pulmonale An Overview 2003Document12 pagesCor Pulmonale An Overview 2003Ade Cahyo IslamiNo ratings yet
- Ventilatory Assistance Study GuideDocument9 pagesVentilatory Assistance Study GuideBrianna RorickNo ratings yet
- Cute Respiratory Distress Syndrome Ards: Guide - DR - Shiv.S.Sharma - Dr.Y. JamraDocument40 pagesCute Respiratory Distress Syndrome Ards: Guide - DR - Shiv.S.Sharma - Dr.Y. JamraandenaNo ratings yet
- Thorax MedDocument3 pagesThorax Medangela mamauagNo ratings yet
- Pulmonary ConditionsDocument42 pagesPulmonary ConditionsMinetteNo ratings yet
- Toronto Notes Respirology PDFDocument40 pagesToronto Notes Respirology PDFJaya Semara Putra67% (3)
- Lung Scintigraphy in Various Lung PathologiesDocument50 pagesLung Scintigraphy in Various Lung PathologiesAnonymous RqEtRdNo ratings yet
- Armando Hasudungan: AuthorsDocument1 pageArmando Hasudungan: AuthorsShubham TarapureNo ratings yet
- Understanding Respiratory Failure: Causes, Symptoms, Diagnosis and TreatmentDocument49 pagesUnderstanding Respiratory Failure: Causes, Symptoms, Diagnosis and TreatmentimaderadityaNo ratings yet
- Clinical Physiology of Respiration: Dr. M Qathar RF TDocument76 pagesClinical Physiology of Respiration: Dr. M Qathar RF TTiwi Lestari TiwiNo ratings yet
- Acute Respiratory FailureDocument2 pagesAcute Respiratory FailureKaja MatovinovicNo ratings yet
- Acute Respiratory Failure (ARF): Causes, Symptoms and TreatmentDocument41 pagesAcute Respiratory Failure (ARF): Causes, Symptoms and TreatmentNozanin MahmadalievaNo ratings yet
- Neonatal EmergenciesDocument21 pagesNeonatal EmergenciesRNo ratings yet
- Pathophysiology:: Symptoms Mechanism and PathophysiologyDocument7 pagesPathophysiology:: Symptoms Mechanism and PathophysiologyRaidis PangilinanNo ratings yet
- 13 - Lung PathologyDocument38 pages13 - Lung PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- DyspnoeaDocument1 pageDyspnoeaShubham TarapureNo ratings yet
- Patho RevDocument21 pagesPatho RevJo CastilloNo ratings yet
- Past Year RespiDocument5 pagesPast Year RespiThulasi tootsieNo ratings yet
- Subject Seminar ON Approach To StridorDocument68 pagesSubject Seminar ON Approach To StridorAimhigh_PPMNo ratings yet
- RES Thoracic Trauma + Pulmonary ContusionDocument33 pagesRES Thoracic Trauma + Pulmonary ContusiondewiswahyuNo ratings yet
- Pedia Cardio Lecture AidDocument5 pagesPedia Cardio Lecture AidStephanie Pearl AldaNo ratings yet
- Cough: by Dr. Meghana Patil (Intern Batch 2016)Document24 pagesCough: by Dr. Meghana Patil (Intern Batch 2016)Meghana PatilNo ratings yet
- NCP PneumoniaDocument2 pagesNCP Pneumoniajulz_otso6359No ratings yet
- Etiologi & Mekanisme HiperkapnikDocument3 pagesEtiologi & Mekanisme HiperkapniksukiyantoNo ratings yet
- Respiratory Tract Pathology New LectureDocument63 pagesRespiratory Tract Pathology New Lectureabenezer isayasNo ratings yet
- NOTES FOR 2ND LECTURE (DRAFT)Document3 pagesNOTES FOR 2ND LECTURE (DRAFT)Mae Arra Lecobu-anNo ratings yet
- Laryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDocument44 pagesLaryngitis, Laryngeal Paralysis, DDX of Stridor, StertorDurand S. KhadkaNo ratings yet
- PneumoniaDocument21 pagesPneumoniaZunaira RaheenNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- James Notes - Volume 1 EDITEDDocument284 pagesJames Notes - Volume 1 EDITEDsuggaplumNo ratings yet
- HypogimpotenceDocument1 pageHypogimpotencewisgeorgekwokNo ratings yet
- Afac 157Document9 pagesAfac 157wisgeorgekwokNo ratings yet
- KDIGO AKI Guideline DownloadDocument141 pagesKDIGO AKI Guideline DownloadSandi AuliaNo ratings yet
- CGA KongDocument36 pagesCGA KongwisgeorgekwokNo ratings yet
- Kundu 2016Document10 pagesKundu 2016wisgeorgekwokNo ratings yet
- Initial Recommended Doses NarrowDocument1 pageInitial Recommended Doses NarrowwisgeorgekwokNo ratings yet
- Atropine Ineffective Transcutaneous PacingDocument1 pageAtropine Ineffective Transcutaneous PacingwisgeorgekwokNo ratings yet
- Newest - Immunotherapy in Lung CancerDocument31 pagesNewest - Immunotherapy in Lung CancerwisgeorgekwokNo ratings yet
- Aldosterone Blocker Used Patients Therapeutic Doses Acei Beta PDFDocument1 pageAldosterone Blocker Used Patients Therapeutic Doses Acei Beta PDFwisgeorgekwokNo ratings yet
- pb520 PDFDocument142 pagespb520 PDFwisgeorgekwokNo ratings yet
- 345 FullDocument8 pages345 FullwisgeorgekwokNo ratings yet
- Count To Ten Allowing YourselfDocument1 pageCount To Ten Allowing YourselfwisgeorgekwokNo ratings yet
- Hourly BP Pulse Resp RateDocument1 pageHourly BP Pulse Resp RatewisgeorgekwokNo ratings yet
- Thrombosis Thrombosis Hypovolemia Hypoxia PDFDocument1 pageThrombosis Thrombosis Hypovolemia Hypoxia PDFwisgeorgekwokNo ratings yet
- Determine Unresponsiveness Call For HelpDocument1 pageDetermine Unresponsiveness Call For HelpwisgeorgekwokNo ratings yet
- 1mg 10 ML of 1 Per 10000 SolutionDocument1 page1mg 10 ML of 1 Per 10000 SolutionwisgeorgekwokNo ratings yet
- Pulmonary Function Testing Case Questions and Answers: Interpretations and Flow Volume LoopsDocument23 pagesPulmonary Function Testing Case Questions and Answers: Interpretations and Flow Volume LoopswisgeorgekwokNo ratings yet
- Good Idea of The Likely DiagnosisDocument1 pageGood Idea of The Likely DiagnosiswisgeorgekwokNo ratings yet
- VSD in The Membranous Interventricular SeptumDocument1 pageVSD in The Membranous Interventricular SeptumwisgeorgekwokNo ratings yet
- A Useful Mnemonic For Any ExaminationDocument1 pageA Useful Mnemonic For Any ExaminationwisgeorgekwokNo ratings yet
- Classification of Stroke SubtypeDocument9 pagesClassification of Stroke SubtypeDedi SutiaNo ratings yet
- Chance of Ascertaining A Sign Are IncreasedDocument1 pageChance of Ascertaining A Sign Are IncreasedwisgeorgekwokNo ratings yet
- YgolorhpenDocument175 pagesYgolorhpenwisgeorgekwokNo ratings yet
- Switching Betwn Insulins PDFDocument4 pagesSwitching Betwn Insulins PDFholaNo ratings yet
- Pulmonary Function Testing Case Questions and Answers: Interpretations and Flow Volume LoopsDocument23 pagesPulmonary Function Testing Case Questions and Answers: Interpretations and Flow Volume LoopswisgeorgekwokNo ratings yet
- BirdbrainDocument1 pageBirdbrainplastoneNo ratings yet
- Happy Birthday Jazz arrangedDocument11 pagesHappy Birthday Jazz arrangedwisgeorgekwok100% (1)
- Brahms Violin Concerto Op 77Document17 pagesBrahms Violin Concerto Op 77wisgeorgekwokNo ratings yet
- Cardiology 1Document1 pageCardiology 1wisgeorgekwokNo ratings yet
- CFPC 99 Topics Starter Study DocumentDocument372 pagesCFPC 99 Topics Starter Study DocumentaayceeNo ratings yet
- Discharge SampleDocument2 pagesDischarge SampleJUDYNo ratings yet
- VAWC Act Protects Women and Children from ViolenceDocument9 pagesVAWC Act Protects Women and Children from ViolenceRames Ely GJNo ratings yet
- SYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Document15 pagesSYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Aaditya GadhviNo ratings yet
- RA. PresentationDocument25 pagesRA. Presentationkhairulsani yusofNo ratings yet
- Endo Part - 5 (Chronic Complication) Without AnswerDocument9 pagesEndo Part - 5 (Chronic Complication) Without AnswerPrachi ChaturvediNo ratings yet
- Internal Medicine I (Junior)Document6 pagesInternal Medicine I (Junior)Joseph RishmawiNo ratings yet
- PJT Confrence December 5th - FixDocument27 pagesPJT Confrence December 5th - Fixmaya_rosmariaNo ratings yet
- Handout For PatientsDocument1 pageHandout For Patientsapi-640781324No ratings yet
- Internal Medicine - 84 - 110Document7 pagesInternal Medicine - 84 - 110Lorenz L. Llamas IIINo ratings yet
- Physical Therapist Skills ChecklistDocument2 pagesPhysical Therapist Skills ChecklistMohamed EssmatNo ratings yet
- Dr. Weny Rinawati - Important and Novel Biomarker For HepatitisDocument24 pagesDr. Weny Rinawati - Important and Novel Biomarker For Hepatitisiq_dianaNo ratings yet
- Post Intensive Care Syndrome A Necessary Harm 1Document6 pagesPost Intensive Care Syndrome A Necessary Harm 1Ronny Araya AbarcaNo ratings yet
- Abcde ApproachDocument3 pagesAbcde ApproachHala BahaaNo ratings yet
- Ear Nose and Throat EmergenciesDocument3 pagesEar Nose and Throat EmergenciesHeribertus AribawaNo ratings yet
- HEALTH Grade 6Document63 pagesHEALTH Grade 6Jetron Cambronero100% (1)
- AnorexiaDocument9 pagesAnorexiaPirandelloNo ratings yet
- Las drogas: Life can take you higher than any kind of drugDocument2 pagesLas drogas: Life can take you higher than any kind of drugAngel RobertoNo ratings yet
- Cerebral Toxoplasmosis in Aids PatientDocument15 pagesCerebral Toxoplasmosis in Aids PatientnoniclaraNo ratings yet
- Prinsip OnkologiDocument20 pagesPrinsip OnkologiTitaPuspitasariNo ratings yet
- Bmi 2022 2023 BaselineDocument2 pagesBmi 2022 2023 BaselineGurla LusHNo ratings yet
- INBDEBooster Oral Medicine NotesDocument52 pagesINBDEBooster Oral Medicine NotesHelena Kalmat100% (1)
- Sarcoma SpecialistDocument5 pagesSarcoma SpecialistaminudinrahmanNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval C - Reactive Protein: CommentDocument6 pagesLaboratory Test Report: Test Name Result Biological Reference Interval C - Reactive Protein: Commentsingh omkeshNo ratings yet
- SMS Medical College, Jaipur Department of UrologyDocument29 pagesSMS Medical College, Jaipur Department of UrologyNarendraNo ratings yet
- Short Report: G. Catimel, F. Chauvin, J. P. Guastalla, P. Rebattu, P. B I R o N M. ClavelDocument3 pagesShort Report: G. Catimel, F. Chauvin, J. P. Guastalla, P. Rebattu, P. B I R o N M. ClavelApril NNo ratings yet
- Class 7 Literature Three Men in A Boat Chapter 6Document3 pagesClass 7 Literature Three Men in A Boat Chapter 6NinjamightyytNo ratings yet
- Chapter 11 GastrointestinalDocument9 pagesChapter 11 GastrointestinalChyNo ratings yet
- Biology InvestigatoryDocument19 pagesBiology InvestigatoryKritika Chavan100% (2)
- Chronic multifactorial autoimmune dermatitisDocument1 pageChronic multifactorial autoimmune dermatitisEran Mark RojasNo ratings yet