You might also like
- Care of Iugr and Low Birth Weight BabiesDocument30 pagesCare of Iugr and Low Birth Weight BabiesjessyNo ratings yet
- Review UNIT XI High Risk NewbornDocument20 pagesReview UNIT XI High Risk NewbornShehana ShihabNo ratings yet
- Low Birth Weight NoteDocument9 pagesLow Birth Weight Notesushma shrestha100% (1)
- High Risk NewbornDocument19 pagesHigh Risk Newbornsantosh s u100% (1)
- Anthropometric MeasurementsDocument3 pagesAnthropometric Measurementssabao kizuiteNo ratings yet
- MCN FinalsDocument40 pagesMCN Finalsmolderoirish600No ratings yet
- MCNDocument12 pagesMCNIan CarodanNo ratings yet
- High Risk Newborn 1Document101 pagesHigh Risk Newborn 1f8kcznbdqjNo ratings yet
- 5 Idol Ko Si Nanay Module 5Document48 pages5 Idol Ko Si Nanay Module 5Mash JumahariNo ratings yet
- Breast FeedingDocument33 pagesBreast Feedingjulie kisku100% (1)
- Unciano Colleges Inc. Sta. Mesa ManilaDocument14 pagesUnciano Colleges Inc. Sta. Mesa Manilanaman24No ratings yet
- WelcomeDocument103 pagesWelcomeLyka BernalNo ratings yet
- Baby at Risk - Koros E.k-1-1-1-1Document132 pagesBaby at Risk - Koros E.k-1-1-1-1victorNo ratings yet
- Post Mature Newborn: Gervacio, Jonah Micah NDocument20 pagesPost Mature Newborn: Gervacio, Jonah Micah NJessa BorreNo ratings yet
- PrematurityDocument66 pagesPrematurityJolmajas JoharNo ratings yet
- Hesi Review For MaternityDocument29 pagesHesi Review For MaternitySteam Lc86% (21)
- MCN LECTURE Final Coaching 2223Document37 pagesMCN LECTURE Final Coaching 22239tfvnv4ghzNo ratings yet
- High-Risk Newborn: Complications Associated With Gestational Age and DevelopmentDocument97 pagesHigh-Risk Newborn: Complications Associated With Gestational Age and DevelopmentALYSSA NICOLE GINESNo ratings yet
- My Paediatric NotesDocument14 pagesMy Paediatric NotesTicky TomNo ratings yet
- Nursing Care of Low Birth Weight BabiesDocument10 pagesNursing Care of Low Birth Weight BabiesAnnisa Yusuf80% (5)
- EincDocument14 pagesEincmendoza jhamNo ratings yet
- Week 9 NCM 109 LectureDocument63 pagesWeek 9 NCM 109 LecturePolicarpio AprilNo ratings yet
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- Maternity and Newborn Nursing ReviewerDocument20 pagesMaternity and Newborn Nursing ReviewerNick RealinoNo ratings yet
- NICU Protocol 100Document76 pagesNICU Protocol 100Catherine Lee100% (1)
- PCBF KpjrawangDocument48 pagesPCBF KpjrawangDr Puteri Nur Sabrina Binti Mohd HanapiNo ratings yet
- MCN Reviewer: Basic ConceptsDocument22 pagesMCN Reviewer: Basic ConceptsPanJan BalNo ratings yet
- BreastfeedingDocument26 pagesBreastfeedingDee SarajanNo ratings yet
- Preterm Infant: Case StudyDocument39 pagesPreterm Infant: Case StudyRey De LunaNo ratings yet
- Assessment Scientific Basis Plan of Care Intervention With Rationale Evaluation Subjective: IndependentDocument16 pagesAssessment Scientific Basis Plan of Care Intervention With Rationale Evaluation Subjective: IndependentAbdullah Mascardo BarabagNo ratings yet
- Maternity and Newborn Nursing ReviewerDocument40 pagesMaternity and Newborn Nursing Reviewerrahkel08No ratings yet
- Pengelolaan Bayi Baru LahirDocument19 pagesPengelolaan Bayi Baru LahirekaNo ratings yet
- Baby at Risk (NBU) NotesDocument131 pagesBaby at Risk (NBU) NotesMercy KeruboNo ratings yet
- Immediate Newborn Care. BlanksDocument11 pagesImmediate Newborn Care. BlanksMay Princes Torregosa Abucejo100% (1)
- Activity 4 NCM 109Document10 pagesActivity 4 NCM 109Angelica BernalesNo ratings yet
- Maternal and Child Health Nursing.Document32 pagesMaternal and Child Health Nursing.Ace FabrigasNo ratings yet
- Pengelolaan Bayi Baru LahirDocument19 pagesPengelolaan Bayi Baru LahirekaNo ratings yet
- Post Partum PeriodDocument31 pagesPost Partum PeriodMay CaballeroNo ratings yet
- High-Risk Newborns and Child During Illness and Hospitalization - Pediatric NursingDocument200 pagesHigh-Risk Newborns and Child During Illness and Hospitalization - Pediatric Nursingjaggermeister20100% (8)
- General Guides To Daily Nicu Practice: Birth Weight (GM) Age To Start Feeding (Day)Document75 pagesGeneral Guides To Daily Nicu Practice: Birth Weight (GM) Age To Start Feeding (Day)Humayun NasserNo ratings yet
- Care of New BornDocument14 pagesCare of New Bornshubham vermaNo ratings yet
- Newborn1Document68 pagesNewborn1Michelle FactoNo ratings yet
- Nursing Care of Newborn and FamilyDocument38 pagesNursing Care of Newborn and FamilyLady Jane CaguladaNo ratings yet
- Case Study (Summer)Document30 pagesCase Study (Summer)dave del rosarioNo ratings yet
- Postpartum Physical AssessmentDocument60 pagesPostpartum Physical AssessmentJhgrace Mary Pacaña Gallo100% (1)
- 2020 Immediate Care of The Newborn 3Document56 pages2020 Immediate Care of The Newborn 3Ellah PerenioNo ratings yet
- Care of Preterm Babies: Chinchu.MDocument59 pagesCare of Preterm Babies: Chinchu.MChinchu MohanNo ratings yet
- Nicu Case StudyDocument4 pagesNicu Case Studyapi-508102663No ratings yet
- NewbornDocument193 pagesNewbornKenneth Myro Garcia100% (1)
- Phototherapy: Presented byDocument49 pagesPhototherapy: Presented byKevin RaiyaniNo ratings yet
- Maternal Nursing BulletDocument37 pagesMaternal Nursing BulletShane ArroyoNo ratings yet
- PEDIAPrelims - 2. Care of The Newborn 1 (First 24 Hours To Vital Signs)Document7 pagesPEDIAPrelims - 2. Care of The Newborn 1 (First 24 Hours To Vital Signs)RenatoCosmeGalvanJuniorNo ratings yet
- Postpartum Physical AssessmentDocument60 pagesPostpartum Physical Assessmentalmyr_rimandoNo ratings yet
- Pedia 2Document30 pagesPedia 2regNo ratings yet
- A. Cardiovascular System: Physiological Effects of Labor On A MotherDocument4 pagesA. Cardiovascular System: Physiological Effects of Labor On A MotherStudent NurseNo ratings yet
- LBWDocument39 pagesLBWJOSLINNo ratings yet
- The Care and Feeding of Children A Catechism for the Use of Mothers and Children's NursesFrom EverandThe Care and Feeding of Children A Catechism for the Use of Mothers and Children's NursesNo ratings yet
- "Nurturing Beginnings: A Comprehensive Guide to Breastfeeding Success"From Everand"Nurturing Beginnings: A Comprehensive Guide to Breastfeeding Success"No ratings yet
- Standing Order SheetDocument1 pageStanding Order SheetLouwella RamosNo ratings yet
- Ramos, LF - 2BN - LFDDocument1 pageRamos, LF - 2BN - LFDLouwella RamosNo ratings yet
- Bryan Beran: Barangay Captain, RizalDocument1 pageBryan Beran: Barangay Captain, RizalLouwella RamosNo ratings yet
- Project ProposalDocument5 pagesProject ProposalLouwella RamosNo ratings yet
- RAMOS, LOUWELLA 2 BN International Health Information Regulatory BodiesDocument2 pagesRAMOS, LOUWELLA 2 BN International Health Information Regulatory BodiesLouwella RamosNo ratings yet
- Program Proposal FinalDocument5 pagesProgram Proposal FinalLouwella RamosNo ratings yet
- Survey Questionnaire Pacheckk 4444Document11 pagesSurvey Questionnaire Pacheckk 4444Louwella RamosNo ratings yet
- COPAR Chapter 10Document2 pagesCOPAR Chapter 10Louwella RamosNo ratings yet
- Ramos - Cervical-DysplasiaDocument1 pageRamos - Cervical-DysplasiaLouwella RamosNo ratings yet
- Ramos - Pathophysiology PCOSDocument1 pageRamos - Pathophysiology PCOSLouwella RamosNo ratings yet
- Coahs Medical Center: Date/Tim E Focus Data, Action, ResponseDocument4 pagesCoahs Medical Center: Date/Tim E Focus Data, Action, ResponseLouwella RamosNo ratings yet
- Copar Ii BN Survey 2Document4 pagesCopar Ii BN Survey 2Louwella RamosNo ratings yet
- Coahs Medical Center: Date/Time Focus Data, Action, ResponseDocument4 pagesCoahs Medical Center: Date/Time Focus Data, Action, ResponseLouwella RamosNo ratings yet
- Adequate InadequateDocument6 pagesAdequate InadequateLouwella RamosNo ratings yet
- Cycling: Ramos, Louwella Faith M. 2-BNDocument7 pagesCycling: Ramos, Louwella Faith M. 2-BNLouwella RamosNo ratings yet
- Copar Ii BN SurveyDocument4 pagesCopar Ii BN SurveyLouwella RamosNo ratings yet
- Drug Name Mechanism of Action Indication Side Effects/ Adverse Reaction Contraindication Nursing ConsiderationsDocument2 pagesDrug Name Mechanism of Action Indication Side Effects/ Adverse Reaction Contraindication Nursing ConsiderationsLouwella RamosNo ratings yet
- Cues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationDocument3 pagesCues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationLouwella RamosNo ratings yet
- Coahs Medical Center: Date/Time Focus Data, Action, ResponseDocument2 pagesCoahs Medical Center: Date/Time Focus Data, Action, ResponseLouwella RamosNo ratings yet
- Medical ManagementDocument2 pagesMedical ManagementLouwella RamosNo ratings yet
- Medical ManagementDocument2 pagesMedical ManagementLouwella RamosNo ratings yet
- LOUWELLA FAITH RAMOS - FIRST QUIZ MARCH 12 MCN QuestionnareDocument3 pagesLOUWELLA FAITH RAMOS - FIRST QUIZ MARCH 12 MCN QuestionnareLouwella RamosNo ratings yet
- Melo, Moinca T. Case Reading Vaginal Bleeding Causes Patient Dysfunctional Uterine BleedingDocument2 pagesMelo, Moinca T. Case Reading Vaginal Bleeding Causes Patient Dysfunctional Uterine BleedingMonica Melo HernandezNo ratings yet
- Theriogenology: S. Fierro, C. Vi Noles, J. Olivera-MuzanteDocument5 pagesTheriogenology: S. Fierro, C. Vi Noles, J. Olivera-MuzanteViviana CarrilloNo ratings yet
- Neonatal and Pediatric Patient Assessment (Study Guide)Document17 pagesNeonatal and Pediatric Patient Assessment (Study Guide)Fatima Sherrisa SaliNo ratings yet
- Small Group Discussion #4: A Case of A 22-Yr Old Nullipara Who Consulted For Left Lower Quadrant PainDocument36 pagesSmall Group Discussion #4: A Case of A 22-Yr Old Nullipara Who Consulted For Left Lower Quadrant PainRose Ann RaquizaNo ratings yet
- Introduction To Educational PyschologyDocument38 pagesIntroduction To Educational PyschologyCarabNo ratings yet
- Health Teaching During PergnancyDocument4 pagesHealth Teaching During PergnancyAnuradha MauryaNo ratings yet
- Lab Report 24 HormonesDocument3 pagesLab Report 24 HormonesLyka ElenaNo ratings yet
- Flink TeenagePregancyDocument1 pageFlink TeenagePregancyAnabel BaticanNo ratings yet
- Kea-Med Medical College 22 Campus: Title: Family Planning Project Work Surgical Contraceptive Individual AssignmentDocument13 pagesKea-Med Medical College 22 Campus: Title: Family Planning Project Work Surgical Contraceptive Individual AssignmentlahmetoNo ratings yet
- Science 5 DLP 1 - Human Reproductive SystemDocument12 pagesScience 5 DLP 1 - Human Reproductive SystemMark Cua89% (35)
- The Sympto-Thermal Method - Ten Years of Change PDFDocument18 pagesThe Sympto-Thermal Method - Ten Years of Change PDFFabian GuardaNo ratings yet
- Ectopic Pregnancy - PathophysiologyDocument1 pageEctopic Pregnancy - PathophysiologyMarimiel PagulayanNo ratings yet
- Science Paper Sec 2Document37 pagesScience Paper Sec 2JOSHI ARNAV ALANKAR Student2020No ratings yet
- Concept of Ovulation in AyurvedaDocument6 pagesConcept of Ovulation in Ayurvedasan MunNo ratings yet
- Clinical Notes 2 ETT-Ped Taping Pre-TermDocument3 pagesClinical Notes 2 ETT-Ped Taping Pre-TermchristinaNo ratings yet
- Fiqh Al Mustajiddaat (Modern Medicine)Document22 pagesFiqh Al Mustajiddaat (Modern Medicine)tisuchiNo ratings yet
- Topographic Anatomy of The Pelvis PDFDocument23 pagesTopographic Anatomy of The Pelvis PDFEl SpinnerNo ratings yet
- Epilepsy and Oral Hormonal Contraception-Indian Perspective: Review ArticleDocument6 pagesEpilepsy and Oral Hormonal Contraception-Indian Perspective: Review ArticleKirubakaranNo ratings yet
- Prime TechDocument32 pagesPrime Techmohd_ikrayemNo ratings yet
- Celulares y Efectos Motirces en El EmbarazoDocument12 pagesCelulares y Efectos Motirces en El EmbarazoNataly GantierNo ratings yet
- Assessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsDocument9 pagesAssessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsLawrence MungaNo ratings yet
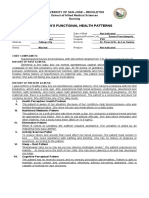
- Gordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingDocument2 pagesGordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- Case Study Presentation: Group 2Document12 pagesCase Study Presentation: Group 2Anna Marie Donaire0% (1)
- Surrogacy in IndiaDocument40 pagesSurrogacy in IndiaAnkita ThakurNo ratings yet
- Integrated Process - CaringDocument23 pagesIntegrated Process - CaringDonaJeanNo ratings yet
- Breast Cancer Case StudyDocument29 pagesBreast Cancer Case StudyAbdelmar Susulan100% (1)
- J Paediatrics Child Health - 2017 - Halliday - The Fascinating Story of SurfactantDocument6 pagesJ Paediatrics Child Health - 2017 - Halliday - The Fascinating Story of SurfactantTin TomašićNo ratings yet
- EBook - ICSE - 10 - MockPaper - 9 Subjects 2023 PDFDocument37 pagesEBook - ICSE - 10 - MockPaper - 9 Subjects 2023 PDFSiddhesh SrikantNo ratings yet
- The First Omen - ScribdDocument1 pageThe First Omen - ScribdazelikoNo ratings yet
- The Nursing Health History (NHH) : NCM 101-A: Health AssessmentDocument7 pagesThe Nursing Health History (NHH) : NCM 101-A: Health Assessmentthe someoneNo ratings yet