You might also like
- Zabdominal ImrtDocument3 pagesZabdominal Imrtapi-431732695No ratings yet
- 1 StfallevalDocument5 pages1 Stfallevalapi-432489466No ratings yet
- Eval 2Document5 pagesEval 2api-280366843No ratings yet
- Esophagus 2Document5 pagesEsophagus 2api-280366843No ratings yet
- 1 StfallevalDocument5 pages1 Stfallevalapi-432489466No ratings yet
- Zabdominal ImrtDocument3 pagesZabdominal Imrtapi-431732695No ratings yet
- Re IrradiationDocument3 pagesRe Irradiationapi-280366843No ratings yet
- Zabdominal ImrtDocument3 pagesZabdominal Imrtapi-431732695No ratings yet
- Detail 27776 2649257Document3 pagesDetail 27776 2649257api-280366843No ratings yet
- Detail 27776 2649257Document3 pagesDetail 27776 2649257api-280366843No ratings yet
- Zabdominal ImrtDocument3 pagesZabdominal Imrtapi-431732695No ratings yet
- BrachyDocument3 pagesBrachyapi-280366843No ratings yet
- Research Paper Group 2 Summer 2020Document9 pagesResearch Paper Group 2 Summer 2020api-484671344No ratings yet
- Group 2 - Final OutlineDocument7 pagesGroup 2 - Final Outlineapi-280366843No ratings yet
- Service ProjectDocument1 pageService Projectapi-280366843No ratings yet
- ContouringDocument6 pagesContouringapi-280366843No ratings yet
- Prostate With NodesDocument3 pagesProstate With Nodesapi-428652649No ratings yet
- Outline Group 2 Summer2020Document6 pagesOutline Group 2 Summer2020api-484671344No ratings yet
- Electron CompDocument3 pagesElectron Compapi-428652649No ratings yet
- Prostate Plan StudyDocument5 pagesProstate Plan Studyapi-280366843No ratings yet
- Detail 27776 2649283Document3 pagesDetail 27776 2649283api-280366843No ratings yet
- FusionDocument2 pagesFusionapi-505214441No ratings yet
- Research Paper Group 2 Summer 2020Document9 pagesResearch Paper Group 2 Summer 2020api-484671344No ratings yet
- Detail 11504 2548223 2Document5 pagesDetail 11504 2548223 2api-280366843No ratings yet
- Data Collection Timeline Group 2 Summer 2020Document3 pagesData Collection Timeline Group 2 Summer 2020api-484671344No ratings yet
- Detail 11504 2548221 3Document5 pagesDetail 11504 2548221 3api-280366843No ratings yet
- Practice Problems Weeks 3-5Document3 pagesPractice Problems Weeks 3-5api-333668576No ratings yet
- Practice Problems Weeks 1 2 For StudentsDocument1 pagePractice Problems Weeks 1 2 For Studentsapi-337168367No ratings yet
- Emami PDFDocument14 pagesEmami PDFAna Buinac100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Journal of Ethnopharmacology: SciencedirectDocument9 pagesJournal of Ethnopharmacology: SciencedirectJOHNNo ratings yet
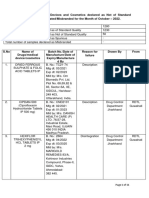
- Drug Alert List of Oct - 2022Document11 pagesDrug Alert List of Oct - 2022Gopal RaoNo ratings yet
- ORGS 1136 - Week 4 Notes ORGS 1136 - Week 4 NotesDocument3 pagesORGS 1136 - Week 4 Notes ORGS 1136 - Week 4 NotesTara FGNo ratings yet
- RN., RM., M.SC (N) ., D.C.A ., (PH.D) Assistant Professor, Dept. of Medical Surgical Nursing, Vmcon, PuducherryDocument30 pagesRN., RM., M.SC (N) ., D.C.A ., (PH.D) Assistant Professor, Dept. of Medical Surgical Nursing, Vmcon, Puducherryjyoti kunduNo ratings yet
- NobelEsthetic Proc&Prod - 2010 - GBDocument116 pagesNobelEsthetic Proc&Prod - 2010 - GBNiaz AhammedNo ratings yet
- Contractor Audit FormDocument2 pagesContractor Audit Formsyamimi balkhis100% (1)
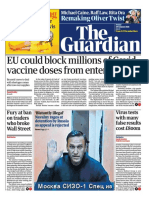
- The Guardian 20210129Document64 pagesThe Guardian 20210129PAULO ROGÉRIO ALENCARNo ratings yet
- TF-CBT and Complex TraumaDocument14 pagesTF-CBT and Complex TraumaDaniel Hidalgo LimaNo ratings yet
- Red Cross Training Content MapDocument2 pagesRed Cross Training Content MapHoward SeibertNo ratings yet
- KS3 Science Revision - Worksheets With AnswersDocument108 pagesKS3 Science Revision - Worksheets With AnswersTony TitanicNo ratings yet
- Unmanned Systems in Support of Future Medical Operations in Dense Urban EnvironmentsDocument28 pagesUnmanned Systems in Support of Future Medical Operations in Dense Urban EnvironmentsEdy JjNo ratings yet
- Brien Et Al - 2012Document21 pagesBrien Et Al - 2012Marzia SmitaNo ratings yet
- Unit IG2: Risk AssessmentDocument22 pagesUnit IG2: Risk Assessmentprijith j100% (6)
- New York Sars-Cov-2 Real-Time Reverse Transcriptase (RT) - PCR Diagnostic PanelDocument27 pagesNew York Sars-Cov-2 Real-Time Reverse Transcriptase (RT) - PCR Diagnostic PanelcassNo ratings yet
- Sex Trafficking in EuropeDocument5 pagesSex Trafficking in EuropeimpunitywatchNo ratings yet
- English 9 Q3 MODULE 1Document10 pagesEnglish 9 Q3 MODULE 1Ri-ann VinculadoNo ratings yet
- USER MANUAL Psoriasis Vitiligo LampDocument50 pagesUSER MANUAL Psoriasis Vitiligo Lamplixo_mail50% (6)
- My Patent Valuation Tool 3Document6 pagesMy Patent Valuation Tool 3nsadnanNo ratings yet
- Client Package Manual (Evic Human Resource MGT., Inc.) - 1Document6 pagesClient Package Manual (Evic Human Resource MGT., Inc.) - 1Shalinur GonzalesNo ratings yet
- Safety ManualDocument21 pagesSafety ManualAli ImamNo ratings yet
- Myotonic Dystrophy PresentationDocument8 pagesMyotonic Dystrophy Presentationapi-318918663No ratings yet
- 3305 Alanya - Gezi - Rehberi 2011 58sDocument58 pages3305 Alanya - Gezi - Rehberi 2011 58sAnıl KaraağaçNo ratings yet
- 016 - Attachment For Full Scale Shear Pads - 01 Mar 11Document54 pages016 - Attachment For Full Scale Shear Pads - 01 Mar 11nadraNo ratings yet
- AP14 - DTC Support Manual - 20160930Document817 pagesAP14 - DTC Support Manual - 20160930tallerr.360No ratings yet
- D-Foot, APADLP & 5th Global 2nd AnnouncementDocument3 pagesD-Foot, APADLP & 5th Global 2nd AnnouncementBun BunNo ratings yet
- Dehlendorf2021 PCC DevelopmentDocument6 pagesDehlendorf2021 PCC Developmentinggar ratnakusumaNo ratings yet
- WDR22 Booklet 1Document74 pagesWDR22 Booklet 1Khánh Hoàng NamNo ratings yet
- Pfe Family PreparednessDocument1 pagePfe Family PreparednessNicole ForrosueloNo ratings yet
- DR Preeti UdaipurDocument19 pagesDR Preeti Udaipurpreeti senthiyaNo ratings yet
- Bellak Tat Sheet2pdfDocument17 pagesBellak Tat Sheet2pdfTalala Usman100% (3)