You might also like
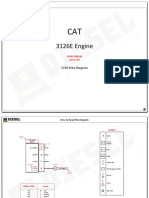
- CAT - 3126E.3126E With Prefix LEFDocument11 pagesCAT - 3126E.3126E With Prefix LEFPhil B.No ratings yet
- Critical Path Method FormularsDocument2 pagesCritical Path Method FormularsGimKonsultNo ratings yet
- 9 - ATPL Questions MeteorologyDocument99 pages9 - ATPL Questions MeteorologyRitwik Chowdhury100% (1)
- Service Manual Cat G3416eDocument753 pagesService Manual Cat G3416eUsaha MandiriNo ratings yet
- 3-Pharmacy, Its Organization and PersonnelDocument27 pages3-Pharmacy, Its Organization and PersonnelHaseeba Khan100% (4)
- Genes Associated With Alzheimer's Disease: An Overview and Current StatusDocument17 pagesGenes Associated With Alzheimer's Disease: An Overview and Current StatusHaseeba KhanNo ratings yet
- Reappraisal of The Autoclave Expansion TestDocument26 pagesReappraisal of The Autoclave Expansion TestCristián JiménezNo ratings yet
- 1998 Framingham - Prediction Coronary Hearth Disease Using Risk Factor CategoriesDocument12 pages1998 Framingham - Prediction Coronary Hearth Disease Using Risk Factor CategoriesJenny PinillaNo ratings yet
- 384.full With Cover Page v2Document14 pages384.full With Cover Page v2Tinh NguyenNo ratings yet
- Risk Factors, Mortality, and Cardiovascular Outcomes in Patients With Type 2 DiabetesDocument12 pagesRisk Factors, Mortality, and Cardiovascular Outcomes in Patients With Type 2 DiabetesAnnisa FujiantiNo ratings yet
- Larsson, SC 2016Document7 pagesLarsson, SC 2016Nicolás MurilloNo ratings yet
- NIH Public Access: Author ManuscriptDocument24 pagesNIH Public Access: Author ManuscriptireneaureliaNo ratings yet
- Letters: R. S. Lindsay, J. A. Little, A. J. Jaap, P. L. Padfield, J. D. Walker, K. J. HardyDocument1 pageLetters: R. S. Lindsay, J. A. Little, A. J. Jaap, P. L. Padfield, J. D. Walker, K. J. HardyPaul AsturbiarisNo ratings yet
- Novel Loci Associated With Increased Risk of Sudden Cardiac Death in The Context of Coronary Artery DiseaseDocument7 pagesNovel Loci Associated With Increased Risk of Sudden Cardiac Death in The Context of Coronary Artery Diseasejustin_saneNo ratings yet
- Poststroke EpilepsyDocument5 pagesPoststroke EpilepsyDian Isti AngrainiNo ratings yet
- Impaired Microvascular Dilatation and Capillary Rarefaction in Young Adults With A Predisposition To High Blood PressureDocument7 pagesImpaired Microvascular Dilatation and Capillary Rarefaction in Young Adults With A Predisposition To High Blood Pressureawad doradoNo ratings yet
- Sinnett1973 New GuineeaDocument26 pagesSinnett1973 New GuineeaVlad GubernatNo ratings yet
- The Incidence of Congestive Heart Failure in Type 2 DiabetesDocument6 pagesThe Incidence of Congestive Heart Failure in Type 2 DiabetesFini Riski Aulia SagalaNo ratings yet
- JAH3 7 E009890Document20 pagesJAH3 7 E009890Ganda AgylNo ratings yet
- 2010 Is Emotional Stress Always The CulpritDocument1 page2010 Is Emotional Stress Always The CulpritNguyễn Tiến HồngNo ratings yet
- Familial Clustering of Hypertensive Target Organ Damage in The CommunityDocument8 pagesFamilial Clustering of Hypertensive Target Organ Damage in The CommunityAnisa Iswari Pombaile-NgurawanNo ratings yet
- How Lifestyle Contributes To CHDDocument3 pagesHow Lifestyle Contributes To CHDchloe a tNo ratings yet
- Treatment of Depression in Elderly Patients With Cardiovascular Disease: Research Data and Future ProspectsDocument11 pagesTreatment of Depression in Elderly Patients With Cardiovascular Disease: Research Data and Future ProspectsGoran KalimNo ratings yet
- Diabetes, Glucose Level, and Risk of Sudden Cardiac DeathDocument6 pagesDiabetes, Glucose Level, and Risk of Sudden Cardiac DeathDino DanielNo ratings yet
- Clin Diabetes 2002 Wittlesey 101 2Document4 pagesClin Diabetes 2002 Wittlesey 101 2Diah Kris AyuNo ratings yet
- Association of Carbamoyl Phosphate Synthase-1 Polymorphism (RS1047891) With Primary Hypertension Among Hypertensives in Ibadan South-West NigeriaDocument16 pagesAssociation of Carbamoyl Phosphate Synthase-1 Polymorphism (RS1047891) With Primary Hypertension Among Hypertensives in Ibadan South-West NigeriaCentral Asian StudiesNo ratings yet
- Coutinho 1999Document8 pagesCoutinho 1999DR VENKATARAMANA MurthyNo ratings yet
- Congenital Heart Disease: Causes, Diagnosis, Symptoms, and TreatmentsDocument4 pagesCongenital Heart Disease: Causes, Diagnosis, Symptoms, and TreatmentsAzis YunalNo ratings yet
- Journal NeurologiDocument9 pagesJournal NeurologiBetari DhiraNo ratings yet
- Lacunar Strokes in Patients With Diabetes Mellitus: Risk Factors, Infarct Location, and PrognosisDocument6 pagesLacunar Strokes in Patients With Diabetes Mellitus: Risk Factors, Infarct Location, and PrognosisNicole Carolina Quintero RomeroNo ratings yet
- 302 Cardiovascular Risk: AssessmentDocument1 page302 Cardiovascular Risk: AssessmentLêHữuHoàiNo ratings yet
- Joc80109 2142 2152aDocument11 pagesJoc80109 2142 2152aDajana LalovicNo ratings yet
- Articulo 6Document6 pagesArticulo 6Gina GuisamanoNo ratings yet
- Characteristics and Prognosis in Women and Men With Type 1 Diabetes Undergoing Coronary Angiography: A Nationwide Registry ReportDocument8 pagesCharacteristics and Prognosis in Women and Men With Type 1 Diabetes Undergoing Coronary Angiography: A Nationwide Registry ReportMike SihombingNo ratings yet
- Article 4 NL RatioDocument4 pagesArticle 4 NL RatioPrateek Kumar PandaNo ratings yet
- Analisis de EC Grupo XDocument10 pagesAnalisis de EC Grupo XMarcelo MaldonadoNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofAssifa RidzkiNo ratings yet
- Captura de Pantalla 2021-08-02 A La(s) 1.24.53 P. M.Document6 pagesCaptura de Pantalla 2021-08-02 A La(s) 1.24.53 P. M.Andres Felipe Quimbayo CifuentesNo ratings yet
- Colchicina Enfermedad Coronaria. NEJM 2022Document10 pagesColchicina Enfermedad Coronaria. NEJM 2022Carlos Alberto Cardenas degolladoNo ratings yet
- Congenital HDDocument4 pagesCongenital HDTampu RajaNiapulNo ratings yet
- LCA ADM Novembre MED6Document6 pagesLCA ADM Novembre MED6capucine.hnkNo ratings yet
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesDocument12 pagesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesAntonella Angulo CruzadoNo ratings yet
- Content ServerDocument11 pagesContent Server沈尚諭No ratings yet
- Article Sciemce90.fullDocument2 pagesArticle Sciemce90.fullHshdhdNo ratings yet
- Premature Cardiovascular Disease and Brain Health in MidlifeDocument11 pagesPremature Cardiovascular Disease and Brain Health in Midlifeveerraju tvNo ratings yet
- TMP AE98Document5 pagesTMP AE98FrontiersNo ratings yet
- Anemia in Young Patients With Ischaemic Stroke2015Document6 pagesAnemia in Young Patients With Ischaemic Stroke2015Nicolas RodriguezNo ratings yet
- Distinct HLA Associations by Stroke Subtype in Children With Sickle Cell AnemiaDocument5 pagesDistinct HLA Associations by Stroke Subtype in Children With Sickle Cell AnemiaLarissa Rodrigues MichalskyNo ratings yet
- Enfermedad Arterial Coronaria en Pacientes DiabéticosDocument10 pagesEnfermedad Arterial Coronaria en Pacientes DiabéticosmacrisgabelaNo ratings yet
- Aldosterone Does Not Predict Cardiovascular Events Following Acute Coronary Syndrome in Patients Initially Without Heart FailureDocument8 pagesAldosterone Does Not Predict Cardiovascular Events Following Acute Coronary Syndrome in Patients Initially Without Heart FailureAbdulkafi tashaniNo ratings yet
- AnginaDocument8 pagesAnginabagusindra1111No ratings yet
- NasirDocument4 pagesNasirMuhammad aliNo ratings yet
- 8931 26614 2 PB PDFDocument7 pages8931 26614 2 PB PDFMaferNo ratings yet
- Resistance Atherosclerosis Study (IRAS) Chronic Subclinical Inflammation As Part of The Insulin Resistance Syndrome: The InsulinDocument7 pagesResistance Atherosclerosis Study (IRAS) Chronic Subclinical Inflammation As Part of The Insulin Resistance Syndrome: The InsulinIngsukiniNo ratings yet
- 2140 FullDocument8 pages2140 FullShukr Wesman BlbasNo ratings yet
- Postgradmedj 96 525Document5 pagesPostgradmedj 96 525Huda TrisenaNo ratings yet
- Rayner 2006Document5 pagesRayner 2006Novita ApramadhaNo ratings yet
- The Association Between Serum Uric Acid Level and Coronary Artery DiseaseDocument8 pagesThe Association Between Serum Uric Acid Level and Coronary Artery DiseasemikeNo ratings yet
- Degludec Vs GlargineDocument10 pagesDegludec Vs GlargineJessica ElizabethNo ratings yet
- 2359 4802 Ijcs 34 05 s01 0012.x98175Document10 pages2359 4802 Ijcs 34 05 s01 0012.x98175Suryati HusinNo ratings yet
- Apneea CPIDocument6 pagesApneea CPINatalia BuruianNo ratings yet
- Glycosylated ProteinsDocument5 pagesGlycosylated ProteinsRonyNo ratings yet
- Ioi 80563Document7 pagesIoi 80563patricia osei-owusuNo ratings yet
- DZ 11Document5 pagesDZ 11licenteNo ratings yet
- Jende 2019 Oi 190203Document12 pagesJende 2019 Oi 190203Eric LimaNo ratings yet
- Hypothyroidism and Atherosclerosis: Anne R. Cappola Paul W. LadensonDocument7 pagesHypothyroidism and Atherosclerosis: Anne R. Cappola Paul W. LadensonLock ThecodeNo ratings yet
- Clinical Approach to Sudden Cardiac Death SyndromesFrom EverandClinical Approach to Sudden Cardiac Death SyndromesRamon BrugadaNo ratings yet
- Epidemiology of Preventable Drug-Related Problems (DRPS) Among Hospitalized Children at Kamc-Jeddah: A Single-Institution Observation StudyDocument9 pagesEpidemiology of Preventable Drug-Related Problems (DRPS) Among Hospitalized Children at Kamc-Jeddah: A Single-Institution Observation StudyHaseeba KhanNo ratings yet
- Winkler 1998Document13 pagesWinkler 1998Haseeba KhanNo ratings yet
- Siegfried 1993Document2 pagesSiegfried 1993Haseeba KhanNo ratings yet
- Clinical Pharmacists' Role in Paediatric Patients' Medical CareDocument5 pagesClinical Pharmacists' Role in Paediatric Patients' Medical CareHaseeba KhanNo ratings yet
- Terry 2003Document7 pagesTerry 2003Haseeba KhanNo ratings yet
- Letters To The EditorDocument12 pagesLetters To The EditorHaseeba KhanNo ratings yet
- The Cholinergic Hypothesis of Neuropsychiatric Symptoms Alzheimer's DiseaseDocument15 pagesThe Cholinergic Hypothesis of Neuropsychiatric Symptoms Alzheimer's DiseaseHaseeba KhanNo ratings yet
- Minimum Standard For Hospital PharmacyDocument15 pagesMinimum Standard For Hospital PharmacyHaseeba Khan100% (2)
- Fotiou 2015Document7 pagesFotiou 2015Haseeba KhanNo ratings yet
- Pharmacy and Therapeutics CommitteeDocument28 pagesPharmacy and Therapeutics CommitteeHaseeba KhanNo ratings yet
- 1-Introduction To Hospital Pharmacy (Updated)Document30 pages1-Introduction To Hospital Pharmacy (Updated)Haseeba KhanNo ratings yet
- Etiology and Pathogenesis of Alzheimer's Disease: AbstractDocument6 pagesEtiology and Pathogenesis of Alzheimer's Disease: AbstractHaseeba KhanNo ratings yet
- Free Radical Theory of Aging: Alzheimer'S Disease PathogenesisDocument23 pagesFree Radical Theory of Aging: Alzheimer'S Disease PathogenesisHaseeba KhanNo ratings yet
- Alzheimer's Disease Pathogenesis: Role of AgingDocument7 pagesAlzheimer's Disease Pathogenesis: Role of AgingHaseeba KhanNo ratings yet
- Does The Mitochondrial Genome Play A Role in The Etiology of Alzheimer's Disease?Document14 pagesDoes The Mitochondrial Genome Play A Role in The Etiology of Alzheimer's Disease?Haseeba KhanNo ratings yet
- Can Angiotensin Receptor-Blocking Drugs Perhaps Be Harmful in The COVID-19 Pandemic?Document2 pagesCan Angiotensin Receptor-Blocking Drugs Perhaps Be Harmful in The COVID-19 Pandemic?Haseeba KhanNo ratings yet
- Software Download ManualDocument10 pagesSoftware Download Manualcidcam100% (2)
- Neet 2023 Question PaperDocument46 pagesNeet 2023 Question Paperhinot95530No ratings yet
- Hood Vents InstallationDocument12 pagesHood Vents Installationapi-26140644No ratings yet
- PVGIS-5 GridConnectedPV 46.047 14.545 Undefined Crystsi 0.6kWp 15 90deg 0deg-1Document1 pagePVGIS-5 GridConnectedPV 46.047 14.545 Undefined Crystsi 0.6kWp 15 90deg 0deg-1FinanceNo ratings yet
- Electrochemistry Short Answers Type Questions PDFDocument7 pagesElectrochemistry Short Answers Type Questions PDFAKSHAT KUMARNo ratings yet
- 2018 Math QuizDocument15 pages2018 Math Quizmaria arliza torioNo ratings yet
- ProjectDocument10 pagesProjectMUHAMMAD RASHIDNo ratings yet
- Handouts General MathematicsDocument70 pagesHandouts General Mathematicskhalid4vuNo ratings yet
- Chandigarh University Department of Electronics & Communication Engineering Assignment # 01Document6 pagesChandigarh University Department of Electronics & Communication Engineering Assignment # 01Jaspreet KaurNo ratings yet
- Ee701-N Interconnected Power SystemDocument4 pagesEe701-N Interconnected Power Systemayan PatelNo ratings yet
- Internship ReportDocument29 pagesInternship ReportPooja koreNo ratings yet
- Combustion in Diesel EngineDocument108 pagesCombustion in Diesel EngineAmanpreet Singh100% (2)
- LinPro PrintingDocument9 pagesLinPro PrintingtresspasseeNo ratings yet
- StewartCalcET8 13 01Document19 pagesStewartCalcET8 13 01OhoodKAlesayiNo ratings yet
- TBA 1013 Assignment 1 SEM 2 2010/2011Document3 pagesTBA 1013 Assignment 1 SEM 2 2010/2011Zafiera ZukriNo ratings yet
- HMT SKDocument60 pagesHMT SKsunilkewat11390No ratings yet
- Abstracts About WeldingDocument9 pagesAbstracts About WeldingVinayak BhustalimathNo ratings yet
- Workman 2017 A Review of Calibration Transfer Practices and Instrument Differences in SpectrosDocument26 pagesWorkman 2017 A Review of Calibration Transfer Practices and Instrument Differences in SpectrosoalegionNo ratings yet
- MU 4080 English Version 1.0.0Document43 pagesMU 4080 English Version 1.0.0Matz100% (1)
- Fast and Reliable: Handheld TympanometerDocument4 pagesFast and Reliable: Handheld TympanometerKothapalli ChiranjeeviNo ratings yet
- 05 iPASO LCT Training Manual (Ethernnet) Dec2012-2Document105 pages05 iPASO LCT Training Manual (Ethernnet) Dec2012-2Wubie NegaNo ratings yet
- Vector Worksheet 10 AnsDocument13 pagesVector Worksheet 10 AnsMegan GohNo ratings yet
- Smart Technologies For Sustainable DevelopmentDocument420 pagesSmart Technologies For Sustainable DevelopmentMaria Rafaela Bezerra de Macêdo RibeiroNo ratings yet
- Theory of Computation Guidelines and Practical List - TutorialsDuniyaDocument2 pagesTheory of Computation Guidelines and Practical List - TutorialsDuniyaPapaNo ratings yet