You might also like
- 2.3 - EnterobacteriaceaeDocument39 pages2.3 - Enterobacteriaceaesajad abasNo ratings yet
- E.coli, Klebsiella Microbiology LectureDocument53 pagesE.coli, Klebsiella Microbiology LecturejwalantkbhattNo ratings yet
- EnterobacteriaceaeDocument98 pagesEnterobacteriaceaeAurora Mae AmoresNo ratings yet
- E. Coli, K. PneumoniaeDocument21 pagesE. Coli, K. Pneumoniaesajad abasNo ratings yet
- PDF Document 2Document313 pagesPDF Document 2nasarcedaNo ratings yet
- لقطة شاشة ٢٠٢٢-٠٦-٠٧ في ٨.١٢.٢٦ مDocument31 pagesلقطة شاشة ٢٠٢٢-٠٦-٠٧ في ٨.١٢.٢٦ مHutheifa SabbarNo ratings yet
- Enterobacteriaceae_2020 Nov_pDocument23 pagesEnterobacteriaceae_2020 Nov_pHUỲNH QUỐC KHÁNHNo ratings yet
- EnterobacteriaDocument127 pagesEnterobacteriaAnton BelyaevNo ratings yet
- Enterobacteriaceae Rev 2013Document46 pagesEnterobacteriaceae Rev 2013MOCHILNo ratings yet
- Lect 2 E.coliDocument49 pagesLect 2 E.coliSumit Sharma Poudel100% (2)
- Enterics Family GuideDocument50 pagesEnterics Family GuideNano FelipeNo ratings yet
- Gram-Negative Rods Related To The Enteric Tract The EnterobacteriaceaeDocument47 pagesGram-Negative Rods Related To The Enteric Tract The EnterobacteriaceaeShattered SoulNo ratings yet
- Lecture 1 - Enterics 15 ShortlyDocument82 pagesLecture 1 - Enterics 15 ShortlyIsak Isak IsakNo ratings yet
- ENTEROBACTERIACEAEDocument13 pagesENTEROBACTERIACEAEStephen Jao Ayala Ujano100% (1)
- Extra Cellular Microbes: DR - Amithbabu.C.B Mscd-EndoDocument35 pagesExtra Cellular Microbes: DR - Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Faculty of Science and Technology Applied Biosciences and BiotechnologyDocument5 pagesFaculty of Science and Technology Applied Biosciences and BiotechnologyAubrey TawandaNo ratings yet
- Enterobacteriacea: Key Characters of The Family EnterobacteriaceaeDocument6 pagesEnterobacteriacea: Key Characters of The Family EnterobacteriaceaetabonNo ratings yet
- Jurnal Infeksi Saluran PencernaanDocument22 pagesJurnal Infeksi Saluran PencernaanDini Okta PutriNo ratings yet
- Classification Identification 2020Document30 pagesClassification Identification 2020sanaaNo ratings yet
- Escherichia ColiDocument31 pagesEscherichia ColiLizzie Fizzie100% (1)
- Basic MicrobiologyDocument53 pagesBasic MicrobiologyJohn NirmalNo ratings yet
- EnterobacteriaceaeDocument3 pagesEnterobacteriaceaeErnie G. Bautista II, RN, MDNo ratings yet
- STREPTOCOCCUSDocument24 pagesSTREPTOCOCCUSTUSHAR MORESHWARNo ratings yet
- EnterobakterDocument36 pagesEnterobakterUttari DalemNo ratings yet
- E ColiDocument104 pagesE Colidrbvramana0% (1)
- Staphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyDocument26 pagesStaphylococcus: Zeinab Abd Elkhalek Prof. of Medical Microbiology & ImmunologyMustafa SaßerNo ratings yet
- Enterobact 2Document23 pagesEnterobact 2Razan J NaealiNo ratings yet
- GI Tract Infections Caused by PathogensDocument66 pagesGI Tract Infections Caused by PathogensAjay IyerNo ratings yet
- EnterobacteriaceaeDocument11 pagesEnterobacteriaceaeAlanah JaneNo ratings yet
- E. ColiDocument17 pagesE. ColiDiksha DahalNo ratings yet
- Micro by DR - Hesham (GIT)Document65 pagesMicro by DR - Hesham (GIT)abcde990075No ratings yet
- EnterobacteriaceaeDocument67 pagesEnterobacteriaceaevaidyamNo ratings yet
- 1classification of Microorganisms Original and Bacterisl StructureDocument76 pages1classification of Microorganisms Original and Bacterisl Structureندى القحطانيNo ratings yet
- ENTEROBACTERIACEAEDocument23 pagesENTEROBACTERIACEAEapi-19916399No ratings yet
- Microbiology: Presented by Alyazeed Hussein, BSCDocument64 pagesMicrobiology: Presented by Alyazeed Hussein, BSCT N100% (1)
- (Medbook4u.com) Microbiology PDFDocument762 pages(Medbook4u.com) Microbiology PDFjohn smithNo ratings yet
- Santos Enterics: Colony MorphologyDocument2 pagesSantos Enterics: Colony MorphologyCarlo SantosNo ratings yet
- EntrobacteriaceaDocument41 pagesEntrobacteriaceaamanuelfeleke0469No ratings yet
- Microorganism Causing Fever: DR - Dedeh Kurniasih Laboratorium Mikrobiologi FK UMPDocument36 pagesMicroorganism Causing Fever: DR - Dedeh Kurniasih Laboratorium Mikrobiologi FK UMPAyuNo ratings yet
- L3 - Enterobactericiae SPPDocument23 pagesL3 - Enterobactericiae SPPbujalkanNo ratings yet
- S. AureusDocument39 pagesS. AureusRajkishor YadavNo ratings yet
- Microbiology Medical MicrobiologyDocument40 pagesMicrobiology Medical MicrobiologyAngelic khanNo ratings yet
- Gram Negative Rods GuideDocument8 pagesGram Negative Rods GuideRuel Maddawin100% (1)
- Rotavirus structural proteins & causes diarrheaDocument4 pagesRotavirus structural proteins & causes diarrheayusrinastitiNo ratings yet
- Family Micrococcaceae and StreptococcaceaeDocument114 pagesFamily Micrococcaceae and StreptococcaceaeAshwani Mathur, Ma-306No ratings yet
- Enterobacteriaceae (Upload)Document48 pagesEnterobacteriaceae (Upload)Ibn Ubaidullah100% (1)
- 5 Gram Negative BacteriaDocument79 pages5 Gram Negative BacteriaSamson NigussieNo ratings yet
- Pyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Document14 pagesPyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Ab AbNo ratings yet
- 9th Lec. Enterobacteriaceae Part 2 and Pseudo2023.Document30 pages9th Lec. Enterobacteriaceae Part 2 and Pseudo2023.Alex AlexNo ratings yet
- Pathogenic Cocci Classification and CharacteristicsDocument72 pagesPathogenic Cocci Classification and CharacteristicsManisanthosh KumarNo ratings yet
- Piogenic Cocci: Ania Kurniawati PD, Dr. MkesDocument58 pagesPiogenic Cocci: Ania Kurniawati PD, Dr. MkesSilmi Zhillan Nur RahmanNo ratings yet
- Enteric Gram-Negative Rods (Enterobacteriaceae) : Prepared by Assistant Professor Dr. Khawaja Shakeel AhmedDocument26 pagesEnteric Gram-Negative Rods (Enterobacteriaceae) : Prepared by Assistant Professor Dr. Khawaja Shakeel AhmedZheemo ArshavinNo ratings yet
- 6 Overview of Enterobacteria. CoprocultureDocument16 pages6 Overview of Enterobacteria. CoprocultureMahmoud IdlbiNo ratings yet
- Microbiology - Overview Reports and IntepretationDocument9 pagesMicrobiology - Overview Reports and IntepretationRo RyNo ratings yet
- Gastrointestinal Infections Due To Enterobacteriaceae: Diarrheogenic E. Coli, Shigellosis, Nontyphoidal Salmonellosis, YersiniosisDocument39 pagesGastrointestinal Infections Due To Enterobacteriaceae: Diarrheogenic E. Coli, Shigellosis, Nontyphoidal Salmonellosis, YersiniosisHyny P'gallaNo ratings yet
- Staphylococcal Food PoisoningDocument18 pagesStaphylococcal Food PoisoningMuhammad Hafidz Bin HasanNo ratings yet
- 402 - Unit-1Document4 pages402 - Unit-1Divyeshkumar GanvitNo ratings yet
- MicrobiologyDocument13 pagesMicrobiologymekuriawNo ratings yet
- Pathogenic SpirillaDocument7 pagesPathogenic SpirillaHamidreza RahmaniNo ratings yet
- Drug Group: Pharmacology and Clinical UseDocument1 pageDrug Group: Pharmacology and Clinical UseYeshaa MiraniNo ratings yet
- Stimulants of M ReceptorsDocument4 pagesStimulants of M ReceptorsYeshaa MiraniNo ratings yet
- Bacterial characteristics, species, diseases and treatmentsDocument27 pagesBacterial characteristics, species, diseases and treatmentsYeshaa MiraniNo ratings yet
- MBBS Pharmacology PDFDocument20 pagesMBBS Pharmacology PDFYeshaa Mirani100% (1)
- Antihypertensive DrugsDocument62 pagesAntihypertensive DrugsYeshaa MiraniNo ratings yet
- RNA VirusesDocument11 pagesRNA VirusesKate Alyssa CatonNo ratings yet
- Autacoids (Local Hormones) and Their Pharmacolo-Gical ModulationDocument75 pagesAutacoids (Local Hormones) and Their Pharmacolo-Gical ModulationAgung PutraNo ratings yet
- Anti Secretary, Antacid and Anti Ulcer Drugs: SolutionDocument2 pagesAnti Secretary, Antacid and Anti Ulcer Drugs: SolutionYeshaa MiraniNo ratings yet
- Sulfonamides and Their Mechanism of ActionDocument61 pagesSulfonamides and Their Mechanism of ActionYeshaa MiraniNo ratings yet
- Internal Med QDocument2 pagesInternal Med QYeshaa MiraniNo ratings yet
- Dna Viruses: Herpes Simplex VirusDocument3 pagesDna Viruses: Herpes Simplex VirusYeshaa MiraniNo ratings yet
- Rna Viruses: EnterovirusDocument4 pagesRna Viruses: EnterovirusYeshaa MiraniNo ratings yet
- Adverse Reactions - EDocument92 pagesAdverse Reactions - EYeshaa MiraniNo ratings yet
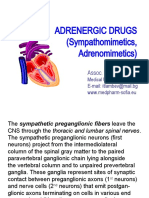
- Adrenergic Drugs (Sympathomimetics, Adrenomimetics) : Assoc. Prof. I. LambevDocument43 pagesAdrenergic Drugs (Sympathomimetics, Adrenomimetics) : Assoc. Prof. I. LambevYeshaa MiraniNo ratings yet
- Auditory-Vestibular Sensory System Anatomy and PhysiologyDocument45 pagesAuditory-Vestibular Sensory System Anatomy and PhysiologyYeshaa MiraniNo ratings yet
- Bacterial GeneticsDocument26 pagesBacterial GeneticsYeshaa MiraniNo ratings yet
- 04 - Trinucleotide Repeat Disorders and Congenital CT DefectsDocument100 pages04 - Trinucleotide Repeat Disorders and Congenital CT DefectsYeshaa MiraniNo ratings yet
- Heart MurmursDocument7 pagesHeart MurmursYeshaa MiraniNo ratings yet
- Anthelmintic Drugs - EDocument24 pagesAnthelmintic Drugs - EYeshaa MiraniNo ratings yet
- Drugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuDocument38 pagesDrugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuYeshaa MiraniNo ratings yet
- USMLE Road Map Pharmacology PDFDocument497 pagesUSMLE Road Map Pharmacology PDFYeshaa Mirani100% (1)
- Pathophysiology Final 1Document162 pagesPathophysiology Final 1Yeshaa Mirani100% (1)
- Sulfonamides and Their Mechanism of ActionDocument61 pagesSulfonamides and Their Mechanism of ActionYeshaa MiraniNo ratings yet
- LungDocument6 pagesLungYeshaa MiraniNo ratings yet
- Pathophysiology Final 3Document148 pagesPathophysiology Final 3Yeshaa MiraniNo ratings yet
- Pathophysiology Final 4Document240 pagesPathophysiology Final 4Yeshaa MiraniNo ratings yet
- Clinical Methods of Examining of Patient With Gall Bladder and Biliary Tract DiseasesDocument2 pagesClinical Methods of Examining of Patient With Gall Bladder and Biliary Tract DiseasesYeshaa MiraniNo ratings yet
- Internal Med QDocument2 pagesInternal Med QYeshaa MiraniNo ratings yet
- Hyperthyroidism, Hypothyroidism, Cushing's Syndrome, Addison's Disease and Gout GuideDocument4 pagesHyperthyroidism, Hypothyroidism, Cushing's Syndrome, Addison's Disease and Gout GuideYeshaa MiraniNo ratings yet
- Or DR Nclex FormsDocument6 pagesOr DR Nclex FormsClarence MangíoNo ratings yet
- Fuller AlbrightDocument4 pagesFuller AlbrightTenri AshariNo ratings yet
- Bowel Training Guide for Constipation, Diarrhea and IrregularityDocument2 pagesBowel Training Guide for Constipation, Diarrhea and Irregularitydickie.gdrNo ratings yet
- Improve Circulation and Oxygenation During CPR with CPVDocument8 pagesImprove Circulation and Oxygenation During CPR with CPVCode ValmirNo ratings yet
- Daftar Peralatan Elektromedik Menurut Ecri Dan WhoDocument4 pagesDaftar Peralatan Elektromedik Menurut Ecri Dan WhoAulia ArthaNo ratings yet
- Guidance For Industry: Clinical Pharmacology Data To Support A Demonstration of Biosimilarity To A Reference ProductDocument18 pagesGuidance For Industry: Clinical Pharmacology Data To Support A Demonstration of Biosimilarity To A Reference ProductBrian WilliamsNo ratings yet
- Cerebro Lys inDocument18 pagesCerebro Lys inKathleen PalomariaNo ratings yet
- Alata SaminaMCQsDocument132 pagesAlata SaminaMCQsmintahmeshackbenjaminNo ratings yet
- X. Comprehensive Pathophysiology and Management of Ovarian CancerDocument3 pagesX. Comprehensive Pathophysiology and Management of Ovarian CancerlieselannjacobNo ratings yet
- 3 MKD PEDIA QUICK NOTESDocument37 pages3 MKD PEDIA QUICK NOTESkaerickaericNo ratings yet
- Orthopedic AssessmentDocument4 pagesOrthopedic Assessmentkrissh20No ratings yet
- Follow The Instructions For R.I.C.EDocument2 pagesFollow The Instructions For R.I.C.Eayatolla ayatollaTMNo ratings yet
- Asbestosis StatPearls NCBIBookshelfDocument11 pagesAsbestosis StatPearls NCBIBookshelfAjeng RahmawatiNo ratings yet
- Case StudyDocument9 pagesCase StudyHenriettaNo ratings yet
- DoctorsClinic Schedule March2023Document4 pagesDoctorsClinic Schedule March2023third IIINo ratings yet
- Nocardia: Gram-Positive Bacteria Found in SoilDocument3 pagesNocardia: Gram-Positive Bacteria Found in Soilsujithas0% (1)
- Nurse Practitioner VS Physical TherapistsDocument5 pagesNurse Practitioner VS Physical Therapistspdet1No ratings yet
- Difference Between COPD & AsthmaDocument9 pagesDifference Between COPD & AsthmaArya UplapNo ratings yet
- Scars PDFDocument9 pagesScars PDFMichaely NataliNo ratings yet
- The Vaccine Adverse Event Reporting System (VAERS)Document356 pagesThe Vaccine Adverse Event Reporting System (VAERS)Josh SingerNo ratings yet
- Pulse RaiserDocument1 pagePulse Raisershaya xoNo ratings yet
- Merck Manual: Professional VersionDocument25 pagesMerck Manual: Professional VersionDwina Wiranti PutriNo ratings yet
- Oral Revalida Round 2Document63 pagesOral Revalida Round 2Mercy Anne EcatNo ratings yet
- Eyelids, Conjunctiva, Cornea & ScleraDocument20 pagesEyelids, Conjunctiva, Cornea & ScleraFemale calm100% (1)
- Chief Complaint FormatDocument3 pagesChief Complaint Formatkazniels100% (1)
- MCQs NeuroDocument2 pagesMCQs NeuroBagadi Suneel100% (2)
- Revisiting Structural Family TherapyDocument2 pagesRevisiting Structural Family TherapyKim ScottNo ratings yet
- Delivery Room (Functions and Responsibilities)Document12 pagesDelivery Room (Functions and Responsibilities)Louis Gabriel AdayaNo ratings yet
- 8feeding The Preterm InfantDocument5 pages8feeding The Preterm InfanttephaniNo ratings yet