You might also like
- Final Nursing Physiology 1 BookDocument46 pagesFinal Nursing Physiology 1 BooklolNo ratings yet
- BloodDocument32 pagesBloodPushpa AdhikariNo ratings yet
- Blood HBDocument31 pagesBlood HBBHUWAN BASKOTANo ratings yet
- 11 Blood BiochemistryDocument98 pages11 Blood Biochemistryfeby ary annasNo ratings yet
- BLG111Document7 pagesBLG111Manasseh LawrenceNo ratings yet
- Physiology Lec 1Document6 pagesPhysiology Lec 1Hussein AlaNo ratings yet
- Fisiologi DARAHDocument31 pagesFisiologi DARAHTririn RinantiNo ratings yet
- Functions of Blood in 40 CharactersDocument29 pagesFunctions of Blood in 40 CharactersShobhit GajbhiyeNo ratings yet
- Hematology - A - RBCsDocument27 pagesHematology - A - RBCsAhmed Hassan KabarNo ratings yet
- Blood Physiology: Functions, Components and RegulationDocument97 pagesBlood Physiology: Functions, Components and Regulationbelete psychiatry100% (5)
- The Circulatory System:: BloodDocument101 pagesThe Circulatory System:: BloodAntonio MihaiNo ratings yet
- DR Samar Word Lecture 1 Blood Elalamein For Students 2021-22Document5 pagesDR Samar Word Lecture 1 Blood Elalamein For Students 2021-22AhmedNo ratings yet
- Chapter-4 Blood and Circulatory SystemDocument94 pagesChapter-4 Blood and Circulatory SystemjarssooNo ratings yet
- Ematology: MLT Department 2 - Stage Theoretical Part/ Lecture No. 1 by Dilgeer Ahmed KalariDocument24 pagesEmatology: MLT Department 2 - Stage Theoretical Part/ Lecture No. 1 by Dilgeer Ahmed Kalariphotocopy beshaNo ratings yet
- HematopoiesisDocument32 pagesHematopoiesisRenad AlharbiNo ratings yet
- The Circulatory System:: BloodDocument122 pagesThe Circulatory System:: BloodYahya RhamadanNo ratings yet
- Blood 2022Document49 pagesBlood 2022Fady FadyNo ratings yet
- Plasma Physiology (1-2020) by DR Khaled A AbulfadleDocument9 pagesPlasma Physiology (1-2020) by DR Khaled A AbulfadleUzama Binu AliNo ratings yet
- The Significance of Blood: A Concise Look at its Composition and FunctionsDocument10 pagesThe Significance of Blood: A Concise Look at its Composition and FunctionsMaqbul AlamNo ratings yet
- Introduction To HematologyDocument95 pagesIntroduction To HematologyAhmad Farhan Hassan0% (1)
- Lecture 11. Blood Biochemistry. Erythrocytes Metabolism. HemoglobinDocument27 pagesLecture 11. Blood Biochemistry. Erythrocytes Metabolism. HemoglobinВіталій Михайлович НечипорукNo ratings yet
- PHYSIOLOGY OF BLOOD CELLS AND FUNCTIONSDocument70 pagesPHYSIOLOGY OF BLOOD CELLS AND FUNCTIONSSultan AhimedNo ratings yet
- Anatomy and Physiology of BloodDocument10 pagesAnatomy and Physiology of Bloodaoi_rachelle100% (1)
- Lecture 9 Physiology of BloodDocument125 pagesLecture 9 Physiology of BloodAhmed MohammedNo ratings yet
- Plasma ProteinDocument79 pagesPlasma ProteinnadieNo ratings yet
- Lec1 Sem1 Year1 BMwk1 2012 01 27Document10 pagesLec1 Sem1 Year1 BMwk1 2012 01 27sehrish_salamNo ratings yet
- LGIS.. Protein ClassificationDocument29 pagesLGIS.. Protein Classificationhasaanmushtaq98765No ratings yet
- Body Fluids and Blood - HUMAN PHYSIOLOGYDocument29 pagesBody Fluids and Blood - HUMAN PHYSIOLOGYSodeinde SimeonNo ratings yet
- Selective B2-Adrenergic Agonists:: Mode of ActionDocument9 pagesSelective B2-Adrenergic Agonists:: Mode of ActionAda JoraimiNo ratings yet
- Chapter 4 Blood Coagulation and Coagulation Disorders _32f6d4d0c67589df3863ad91f445f357Document27 pagesChapter 4 Blood Coagulation and Coagulation Disorders _32f6d4d0c67589df3863ad91f445f357daisysintszwaiNo ratings yet
- Questions From Exam 08.09.22Document12 pagesQuestions From Exam 08.09.22Ismo SNo ratings yet
- Functions of Blood: Transport, Regulation, ProtectionDocument52 pagesFunctions of Blood: Transport, Regulation, ProtectionNestor BalboaNo ratings yet
- Blood Performs A Number of Functions Dealing WithDocument52 pagesBlood Performs A Number of Functions Dealing WithCLEMENTNo ratings yet
- Biomedic Ii Cardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirDocument55 pagesBiomedic Ii Cardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirZurezki Yuana YafieNo ratings yet
- General Function of The BloodDocument25 pagesGeneral Function of The BloodMsKizzyNo ratings yet
- Group 9 (Module 23)Document26 pagesGroup 9 (Module 23)maba.zuniga.sjcNo ratings yet
- Hemeostasis 1Document52 pagesHemeostasis 1Abdo HaiderNo ratings yet
- Written Report Copy BloodDocument29 pagesWritten Report Copy BloodNathalieCaracaNo ratings yet
- Blood CirculatoryDocument5 pagesBlood CirculatoryRekesh SaeedNo ratings yet
- Blood: - Enzymes, E.G. Certain Clotting FactorsDocument14 pagesBlood: - Enzymes, E.G. Certain Clotting FactorsDerrick kinyaNo ratings yet
- Cardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirDocument68 pagesCardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirikhyNo ratings yet
- Chapter 5a - Blood PhysiologyDocument102 pagesChapter 5a - Blood PhysiologyAbera AberaNo ratings yet
- AnaemiasDocument60 pagesAnaemiasbvkjtzrvnyNo ratings yet
- Plasma Proteins and Their FunctionsDocument71 pagesPlasma Proteins and Their FunctionsIdenyi Daniel EwaNo ratings yet
- Blood ReviewDocument13 pagesBlood ReviewDeleted AccountNo ratings yet
- Plasma Proteins, Immunoglobulins and Blood CoagulationDocument45 pagesPlasma Proteins, Immunoglobulins and Blood CoagulationKurnia SaptaNo ratings yet
- BIOCHEMICAL ASPECT OF BLOOD-aDocument78 pagesBIOCHEMICAL ASPECT OF BLOOD-aSofie Hanafiah NuruddhuhaNo ratings yet
- 4 Blood physiologyDocument79 pages4 Blood physiologysefiw.amareNo ratings yet
- Endocrine System Module: Blood and PlasmaDocument179 pagesEndocrine System Module: Blood and PlasmaƯớc Của BếttingNo ratings yet
- Blood PhysiologyyDocument142 pagesBlood PhysiologyylemmademewakeneNo ratings yet
- Blood Cells and The Hematopoetic SystemDocument53 pagesBlood Cells and The Hematopoetic SystemMeet RandhawaNo ratings yet
- BLOOD Update-1Document56 pagesBLOOD Update-1ahmadfadi343No ratings yet
- Lec-1 Hematopoiesis and RBCsDocument38 pagesLec-1 Hematopoiesis and RBCsMuna MNo ratings yet
- Red Blood Cells, Anemia, and PolycythemiaDocument7 pagesRed Blood Cells, Anemia, and PolycythemiaShi no Me100% (1)
- Nurs 107 Blood Physiology Lecture 4Document46 pagesNurs 107 Blood Physiology Lecture 4Ann AgyeiwaaNo ratings yet
- LSM3212 - Lecture 2-4 BloodDocument59 pagesLSM3212 - Lecture 2-4 BloodAbraham KangNo ratings yet
- Biokimia Sistem Hematologi EnglishDocument46 pagesBiokimia Sistem Hematologi EnglishIrham KhairiNo ratings yet
- MODULE 23 BLOOD and URINEDocument31 pagesMODULE 23 BLOOD and URINECrystal ManguneNo ratings yet
- Lec 4 P 2Document3 pagesLec 4 P 2Mustafa SaßerNo ratings yet
- Recent Advances in Pulp Capping Materials: An Overview: Abst TDocument6 pagesRecent Advances in Pulp Capping Materials: An Overview: Abst TMustafa SaßerNo ratings yet
- Grade BreakdownDocument1 pageGrade BreakdownMustafa SaßerNo ratings yet
- Crown 2 QB: Put T&F. and Correct The False StatementDocument17 pagesCrown 2 QB: Put T&F. and Correct The False StatementMustafa SaßerNo ratings yet
- Oral Lec3p2Document3 pagesOral Lec3p2Mustafa SaßerNo ratings yet
- Oral Lec3Document7 pagesOral Lec3Mustafa SaßerNo ratings yet
- 231 Fall2009 MidtermDocument1 page231 Fall2009 MidtermMustafa SaßerNo ratings yet
- Lec4 p1Document5 pagesLec4 p1Mustafa SaßerNo ratings yet
- Crown 2 QB: Put T&F. and Correct The False StatementDocument24 pagesCrown 2 QB: Put T&F. and Correct The False StatementMustafa SaßerNo ratings yet
- Oral Path 2Document6 pagesOral Path 2Mustafa SaßerNo ratings yet
- Radiographically: They Will Appear As UnilocularDocument1 pageRadiographically: They Will Appear As UnilocularMustafa SaßerNo ratings yet
- Lec 5Document6 pagesLec 5Mustafa SaßerNo ratings yet
- Working Cast Die 1Document64 pagesWorking Cast Die 1Mustafa SaßerNo ratings yet
- RES411 Group: A1: ID Name TopicDocument3 pagesRES411 Group: A1: ID Name TopicMustafa SaßerNo ratings yet
- Oral Lec3Document7 pagesOral Lec3Mustafa SaßerNo ratings yet
- Oral Pathology Signs and SyndromesDocument6 pagesOral Pathology Signs and SyndromesMustafa SaßerNo ratings yet
- Classified Past ExamsDocument4 pagesClassified Past ExamsMustafa SaßerNo ratings yet
- Classified Past ExamsDocument4 pagesClassified Past ExamsMustafa SaßerNo ratings yet
- Revision On Lect. 1 and 2Document6 pagesRevision On Lect. 1 and 2Mustafa SaßerNo ratings yet
- Opthalmology (Hazem)Document9 pagesOpthalmology (Hazem)Mustafa SaßerNo ratings yet
- Oral Lec3p2Document3 pagesOral Lec3p2Mustafa SaßerNo ratings yet
- Classified Past ExamsDocument4 pagesClassified Past ExamsMustafa SaßerNo ratings yet
- Carboxylic acid derivatives lectureDocument19 pagesCarboxylic acid derivatives lectureMustafa SaßerNo ratings yet
- Revision 4Document7 pagesRevision 4Mustafa SaßerNo ratings yet
- NUTRITION GUIDELINES SUMMARYDocument6 pagesNUTRITION GUIDELINES SUMMARYMustafa SaßerNo ratings yet
- Revision 4Document7 pagesRevision 4Mustafa SaßerNo ratings yet
- Revision On Lect. 1 and 2Document6 pagesRevision On Lect. 1 and 2Mustafa SaßerNo ratings yet
- Revision 4Document7 pagesRevision 4Mustafa SaßerNo ratings yet
- Nut 200Document3 pagesNut 200Mustafa SaßerNo ratings yet
- Revision Quiz Organic ChemistryDocument6 pagesRevision Quiz Organic ChemistryMustafa SaßerNo ratings yet
- RTR Piping Inspection GuideDocument17 pagesRTR Piping Inspection GuideFlorante NoblezaNo ratings yet
- Computer ViruesDocument19 pagesComputer ViruesMuhammad Adeel AnsariNo ratings yet
- CellphoneBill PDFDocument6 pagesCellphoneBill PDFRaza KhanNo ratings yet
- Parts of The Analog MultitesterDocument4 pagesParts of The Analog MultitesterDestiny Marasigan CanacanNo ratings yet
- Fellowship in OncotherapeutDocument3 pagesFellowship in OncotherapeutNayan ChaudhariNo ratings yet
- An Introduction To Log ShootingDocument10 pagesAn Introduction To Log ShootingSorin GociuNo ratings yet
- Cengage Eco Dev Chapter 13 - The Environment and Sustainable Development in AsiaDocument32 pagesCengage Eco Dev Chapter 13 - The Environment and Sustainable Development in AsiaArcy LeeNo ratings yet
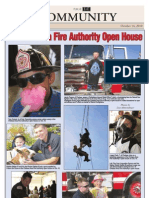
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- 7 - NIBL - G.R. No. L-15380 Wan V Kim - DigestDocument1 page7 - NIBL - G.R. No. L-15380 Wan V Kim - DigestOjie SantillanNo ratings yet
- Reprocessing Guide: Shaver Handpiece TrayDocument198 pagesReprocessing Guide: Shaver Handpiece TrayAnne Stephany ZambranoNo ratings yet
- Huang V Tesla State of Calif 20190430Document20 pagesHuang V Tesla State of Calif 20190430jonathan_skillings100% (1)
- Basketball 2011: Johnson CountyDocument25 pagesBasketball 2011: Johnson CountyctrnewsNo ratings yet
- Inspection and Test Plan Steel Sheet Pile DriDocument6 pagesInspection and Test Plan Steel Sheet Pile DriSofda Imela100% (1)
- Qcs 2010 Section 13 Part 3 Accessories PDFDocument3 pagesQcs 2010 Section 13 Part 3 Accessories PDFbryanpastor106No ratings yet
- Power System Analysis and Design, SI EditionDocument5 pagesPower System Analysis and Design, SI EditionAkimeNo ratings yet
- If Sentences Type 1 First Type Conditionals Grammar Drills - 119169Document2 pagesIf Sentences Type 1 First Type Conditionals Grammar Drills - 119169Ivanciu DanNo ratings yet
- Ch10 Stress in Simple WordsDocument7 pagesCh10 Stress in Simple Wordsmanaar munthirNo ratings yet
- Intermediate Accounting 2 - CL NCL Lecture NotesDocument2 pagesIntermediate Accounting 2 - CL NCL Lecture NotesRacheel SollezaNo ratings yet
- MCQs on PharmacologyDocument101 pagesMCQs on PharmacologyMohammad Rashid88% (8)
- IGNOU MBA MS-11 Solved AssignmentDocument5 pagesIGNOU MBA MS-11 Solved AssignmenttobinsNo ratings yet
- 01 - PV - RESCO 1d Workshop - S1 PDFDocument61 pages01 - PV - RESCO 1d Workshop - S1 PDFDeasy KurniawatiNo ratings yet
- 2008-14-03Document6 pages2008-14-03RAMON CALDERONNo ratings yet
- 2 Both Texts, and Then Answer Question 1 On The Question Paper. Text A: Esports in The Olympic Games?Document2 pages2 Both Texts, and Then Answer Question 1 On The Question Paper. Text A: Esports in The Olympic Games?...No ratings yet
- Engr2227 Apr03Document10 pagesEngr2227 Apr03Mohamed AlqaisiNo ratings yet
- WISECO 2011 Complete CatalogDocument131 pagesWISECO 2011 Complete CatalogfishuenntNo ratings yet
- FSRE SS AppendixGlossariesDocument27 pagesFSRE SS AppendixGlossariessachinchem020No ratings yet
- Chapter 6 Managing Quality (Sesi 3)Document68 pagesChapter 6 Managing Quality (Sesi 3)Nurmala SariNo ratings yet
- Science MELCsDocument42 pagesScience MELCsRanjell Allain TorresNo ratings yet
- A Generation of Contradictions-Unlocking Gen Z 2022 China FocusDocument25 pagesA Generation of Contradictions-Unlocking Gen Z 2022 China FocusCindy Xidan XiaoNo ratings yet
- Unit 7 Noun ClauseDocument101 pagesUnit 7 Noun ClauseMs. Yvonne Campbell0% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)