You might also like
- WJR 5 143Document13 pagesWJR 5 143andre halimNo ratings yet
- Carotid-Cavernous Fistula: Current Concepts in Aetiology, Investigation, and ManagementDocument9 pagesCarotid-Cavernous Fistula: Current Concepts in Aetiology, Investigation, and Managementandre halimNo ratings yet
- Article 56252 PDFDocument9 pagesArticle 56252 PDFandre halimNo ratings yet
- E127 FullDocument7 pagesE127 Fullandre halimNo ratings yet
- Paraneoplastic Syndromes Associated With LaryngealDocument15 pagesParaneoplastic Syndromes Associated With Laryngealandre halimNo ratings yet
- 08 Ijss June Oa 08 - 2019Document5 pages08 Ijss June Oa 08 - 2019andre halimNo ratings yet
- Treating Laryngeal and Hypopharyngeal CancerDocument32 pagesTreating Laryngeal and Hypopharyngeal Cancerandre halimNo ratings yet
- Yang Oteh: Karsinoma LaringDocument8 pagesYang Oteh: Karsinoma Laringandre halimNo ratings yet
- Management of Advanced Laryngeal Cancer: Open AccessDocument12 pagesManagement of Advanced Laryngeal Cancer: Open Accessandre halimNo ratings yet
- Contemporary Management of Advanced Laryngeal CancDocument3 pagesContemporary Management of Advanced Laryngeal Cancandre halimNo ratings yet
- Laryngeal Cancer, Risk Factors, Symptoms and Treatment PDFDocument8 pagesLaryngeal Cancer, Risk Factors, Symptoms and Treatment PDFandre halimNo ratings yet
- It S Not Normal : Toxic RelationshipsDocument10 pagesIt S Not Normal : Toxic Relationshipsandre halimNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Rajasthan - Economy, Infrastructure and Development AnalysisDocument62 pagesRajasthan - Economy, Infrastructure and Development AnalysisbhalakankshaNo ratings yet
- Food Safety Training Agenda-Unika Soegijapranata - 12-16 Juli 2021Document6 pagesFood Safety Training Agenda-Unika Soegijapranata - 12-16 Juli 2021Agustina TasyaNo ratings yet
- Amendment 3 To AIS 156Document7 pagesAmendment 3 To AIS 156pranavNo ratings yet
- Drive Test Sim COF953MM - COMBATBALEREJO Offline Madiun, East Java November 30, 2020Document7 pagesDrive Test Sim COF953MM - COMBATBALEREJO Offline Madiun, East Java November 30, 2020Akhmad Hafid IrawanNo ratings yet
- REGENERATE - How To Reverse COVID Vaxx Related Injuries and Repair Damaged TissueDocument46 pagesREGENERATE - How To Reverse COVID Vaxx Related Injuries and Repair Damaged TissuemihailuicanNo ratings yet
- Recommended Values For Road Rail and BackfillDocument3 pagesRecommended Values For Road Rail and BackfillAnonymous VeDNBhNo ratings yet
- Catalytic Converter Using Nano TechnologyDocument4 pagesCatalytic Converter Using Nano TechnologySwathi PadalaNo ratings yet
- IGCSE Biology NotesDocument21 pagesIGCSE Biology NotesalfaazmcsNo ratings yet
- Biochemistry: Topic-Wise QuestionsDocument11 pagesBiochemistry: Topic-Wise QuestionsvkNo ratings yet
- STANDARD OPERATING PROCEDURE - Preparing Agar Plates - SOP Preparing Agar Plates - v2Document4 pagesSTANDARD OPERATING PROCEDURE - Preparing Agar Plates - SOP Preparing Agar Plates - v2biswasblrNo ratings yet
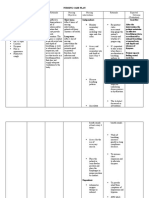
- NCP ScribdDocument3 pagesNCP ScribdAngela AyalaNo ratings yet
- DLP 17Document2 pagesDLP 17Hannisch Anne SakuraNo ratings yet
- Exam Year Questions and AnswersDocument8 pagesExam Year Questions and AnswersArdianto SuhendarNo ratings yet
- Tube-to-Tubesheet Joints - BaherDocument51 pagesTube-to-Tubesheet Joints - BaherNAMO100% (3)
- Bna Swot Analysis ListDocument11 pagesBna Swot Analysis ListBenjie MartinezNo ratings yet
- Ellipsoidal Dished EndsDocument28 pagesEllipsoidal Dished EndsRamakrishnan SrinivasanNo ratings yet
- Drilling Mud CalculationDocument12 pagesDrilling Mud Calculationaditya imansyahNo ratings yet
- Ansoff MatrixDocument26 pagesAnsoff MatrixPulkit MehrotraNo ratings yet
- The Subjunctive Mood in Modern Greek: Na +rima Se Enestota)Document3 pagesThe Subjunctive Mood in Modern Greek: Na +rima Se Enestota)Emmanuel BarabbasNo ratings yet
- Woking Priciple in DCDocument7 pagesWoking Priciple in DCRohit Kumar DasNo ratings yet
- User Manuel - ESCODocument38 pagesUser Manuel - ESCOSerhat YıldırımNo ratings yet
- Basic First Aid 0808Document72 pagesBasic First Aid 0808BS AnilKumarNo ratings yet
- THEENGLISHCLUB AllLessonsDocument62 pagesTHEENGLISHCLUB AllLessonsMaurício RizzoNo ratings yet
- Seiten Aus Final Documentation Nav Gas H8194 - 8195Document5 pagesSeiten Aus Final Documentation Nav Gas H8194 - 8195NorbertoNo ratings yet
- Urea EPC ScheduleDocument45 pagesUrea EPC Schedulevishal_madhukar100% (1)
- Penicillin ActDocument5 pagesPenicillin Actcecile towerNo ratings yet
- Fluid & Electrolite Management in Surgical WardsDocument97 pagesFluid & Electrolite Management in Surgical WardsBishwanath PrasadNo ratings yet
- Medical Marijuana TaxesDocument6 pagesMedical Marijuana TaxesSuresh AsangiNo ratings yet
- Lesson 1 - Basic Principles of PlumbingDocument12 pagesLesson 1 - Basic Principles of PlumbingNicholas Bonn Sing100% (1)
- S2 2016 370885 BibliographyDocument12 pagesS2 2016 370885 BibliographyBen Yudha SatriaNo ratings yet