You might also like
- Continence and Prostate: A Guide For Men Undergoing Prostate SurgeryDocument7 pagesContinence and Prostate: A Guide For Men Undergoing Prostate Surgeryc223096No ratings yet
- Continence Problems After StrokeDocument8 pagesContinence Problems After StrokeYocha BangunNo ratings yet
- Reversal of IleostomyDocument7 pagesReversal of IleostomyGTL StickersNo ratings yet
- Reduced Bladder EmptyingDocument2 pagesReduced Bladder EmptyingThe Saloniti BabiesNo ratings yet
- Top 17 Questions in Urology: in This Chapter, We'll Go Over Common Health Problems in UrologyDocument13 pagesTop 17 Questions in Urology: in This Chapter, We'll Go Over Common Health Problems in UrologyadenwijayaNo ratings yet
- The Coombe Physiotherapy & Your Pelvic Floor Feb 2021Document20 pagesThe Coombe Physiotherapy & Your Pelvic Floor Feb 2021Andreea ManeaNo ratings yet
- Abdominal Rectopexy Operation: Your Questions AnsweredDocument5 pagesAbdominal Rectopexy Operation: Your Questions AnsweredlakanthNo ratings yet
- Urinary Incontinence Has Sesven TypesDocument55 pagesUrinary Incontinence Has Sesven TypesDhonat Flash100% (1)
- Urinary Incontinence Brochure 2009Document5 pagesUrinary Incontinence Brochure 2009swap2390No ratings yet
- Urodynamic Testing ReportDocument25 pagesUrodynamic Testing Reportzharah180% (1)
- Faecal IncontinenceDocument21 pagesFaecal IncontinenceDee wilsonNo ratings yet
- Bladder Training PDFDocument5 pagesBladder Training PDFDjfnswn UkhtyNo ratings yet
- Pelvic Floor Exercises For MenDocument5 pagesPelvic Floor Exercises For MenGabrielMouraNo ratings yet
- FghikDocument3 pagesFghikfahfahrulNo ratings yet
- Rectal ProlapseDocument9 pagesRectal ProlapseAnjani Putri RetnaninggalihNo ratings yet
- Physiotherapy Before and After Prostate Cancer Surgery PDFDocument8 pagesPhysiotherapy Before and After Prostate Cancer Surgery PDFJohn SterlingNo ratings yet
- 5960 1 Hartmanns ProcedureDocument8 pages5960 1 Hartmanns ProcedurecosmicdaeNo ratings yet
- IncontenenceDocument5 pagesIncontenenceMuhammad Omar KhanNo ratings yet
- Urinary Incontinence: The American College of Obstetricians and GynecologistsDocument3 pagesUrinary Incontinence: The American College of Obstetricians and GynecologistsIzat FuadiNo ratings yet
- After TURP: What to expectDocument2 pagesAfter TURP: What to expectvilla88No ratings yet
- SCI Bladder SurgeryDocument4 pagesSCI Bladder SurgeryKrish NevageNo ratings yet
- Bowel IncontinenceDocument10 pagesBowel Incontinenceibrahim 12No ratings yet
- Pelvic Floor Muscle Exercises and Advice For MenDocument8 pagesPelvic Floor Muscle Exercises and Advice For Mensantjitr679No ratings yet
- Urinary Problems-IfmDocument16 pagesUrinary Problems-Ifmapi-675909478No ratings yet
- Information For You: Pelvic Organ ProlapseDocument8 pagesInformation For You: Pelvic Organ Prolapsesandeepv08No ratings yet
- Pelvic Floor Exercises: A Guide For Men AboutDocument3 pagesPelvic Floor Exercises: A Guide For Men AboutemagooNo ratings yet
- Trans Urethral Resection of The ProstateDocument2 pagesTrans Urethral Resection of The ProstatehypopiaNo ratings yet
- Total Proctocolectomy With IleostomyDocument5 pagesTotal Proctocolectomy With Ileostomyrachelmores12No ratings yet
- What Causes Urinary Retention?Document4 pagesWhat Causes Urinary Retention?darkz_andreaslimNo ratings yet
- Elimination Review: Urinary Function and Nursing CareDocument27 pagesElimination Review: Urinary Function and Nursing Careالموعظة الحسنه chanelNo ratings yet
- Urinary Elimination DisordersDocument42 pagesUrinary Elimination DisordersMara Jon Ocden CasibenNo ratings yet
- Cystoscopy WordDocument4 pagesCystoscopy WordMon ManguilinNo ratings yet
- PS-27238-Spotlightguide-Pelvic Floor Excercises A5 JCDocument4 pagesPS-27238-Spotlightguide-Pelvic Floor Excercises A5 JCKishor KumarNo ratings yet
- Cystoscopy OSCEDocument5 pagesCystoscopy OSCEKevin TangNo ratings yet
- Comprehensive Overview of Constipation: William E. Whitehead, PHD Center Co-DirectorDocument3 pagesComprehensive Overview of Constipation: William E. Whitehead, PHD Center Co-DirectornehaNo ratings yet
- Urinary Incontinence: 2 PathophysiologyDocument8 pagesUrinary Incontinence: 2 PathophysiologyZiedTrikiNo ratings yet
- Pelvic Floor Exercises For Men Info SheetDocument3 pagesPelvic Floor Exercises For Men Info SheetTracey BrownNo ratings yet
- HOLEP-info-sheetDocument9 pagesHOLEP-info-sheetcjmrioNo ratings yet
- INCONTINENCE3Document12 pagesINCONTINENCE3allthingali217No ratings yet
- The Rules of Dating - Penelope WardDocument16 pagesThe Rules of Dating - Penelope WardRichard CortezNo ratings yet
- Clinical ReasoningDocument2 pagesClinical ReasoningJOHN PEARL FERNANDEZNo ratings yet
- Overactive BladderDocument4 pagesOveractive BladderRanda Hayudha SNo ratings yet
- 5960 1 Hartmanns ProcedureDocument8 pages5960 1 Hartmanns ProcedureZakiNo ratings yet
- Prostatectomy Procedures and Risks ExplainedDocument11 pagesProstatectomy Procedures and Risks ExplainedPhyan HyunNo ratings yet
- Anal Sphincter Exercises for LeakageDocument6 pagesAnal Sphincter Exercises for LeakageNicolae NedeaNo ratings yet
- Urinary RetentionDocument6 pagesUrinary RetentiongradnurseNo ratings yet
- Transobturator Midurethral SlingDocument32 pagesTransobturator Midurethral SlingclaudiuNo ratings yet
- Fecal ImpactionDocument5 pagesFecal Impactioncharie2No ratings yet
- A Guide To The Pelvic Floor Muscles - Men: Oxford University HospitalsDocument8 pagesA Guide To The Pelvic Floor Muscles - Men: Oxford University HospitalsshamsulNo ratings yet
- Pelvic Floor Exercises For WomenDocument3 pagesPelvic Floor Exercises For Womenreza.7868910100% (2)
- Anorectal MalformationDocument19 pagesAnorectal MalformationRahma Dewi RadhewNo ratings yet
- Accidental Bowel Leakage: The American College of Obstetricians and GynecologistsDocument4 pagesAccidental Bowel Leakage: The American College of Obstetricians and GynecologistsPaulNo ratings yet
- The Pelvic Floor Muscles - A Guide For WomenDocument12 pagesThe Pelvic Floor Muscles - A Guide For WomenQORI KARUNIA WANTINo ratings yet
- Prostate, Functions, Diseases A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandProstate, Functions, Diseases A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Skills LabDocument20 pagesSkills LabJei JayNo ratings yet
- Nephrectomy: The Advantages of Laparoscopic Surgery IncludeDocument5 pagesNephrectomy: The Advantages of Laparoscopic Surgery IncludeLouie ParillaNo ratings yet
- Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop: Why Do I Need This Surgery?Document6 pagesUrinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop: Why Do I Need This Surgery?Panji SetyawanNo ratings yet
- Cystocele, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCystocele, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Urinary Retention, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandUrinary Retention, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 1 out of 5 stars1/5 (1)
- A Simple Guide to Disorders of Pelvic Floor Organs, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Disorders of Pelvic Floor Organs, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Bener 016Document7 pagesBener 016Yosalfa Adhista KurniawanNo ratings yet
- Grabbe 2016Document12 pagesGrabbe 2016Yosalfa Adhista KurniawanNo ratings yet
- Zelio Timer Relays - RUZC2MDocument3 pagesZelio Timer Relays - RUZC2MYosalfa Adhista KurniawanNo ratings yet
- Paulownia Tree Potential Alternative Raw Material for Pencil ManufacturingDocument8 pagesPaulownia Tree Potential Alternative Raw Material for Pencil ManufacturingYosalfa Adhista KurniawanNo ratings yet
- COVID 19 Coding Icd10Document4 pagesCOVID 19 Coding Icd10Yosalfa Adhista KurniawanNo ratings yet
- Ijer v2Document13 pagesIjer v2Yosalfa Adhista KurniawanNo ratings yet
- Accepted Manuscript: Accident Analysis and PreventionDocument25 pagesAccepted Manuscript: Accident Analysis and PreventionYosalfa Adhista KurniawanNo ratings yet
- Cum Cultivi Paulownia, Culturi Intercalate71235Document74 pagesCum Cultivi Paulownia, Culturi Intercalate71235Dragos Ranca100% (1)
- WHO 2019 nCoV SARI - Toolkit 2020.1 Eng PDFDocument196 pagesWHO 2019 nCoV SARI - Toolkit 2020.1 Eng PDFbeny nurjaman100% (1)
- 0Document2 pages0Yosalfa Adhista KurniawanNo ratings yet
- 0921Document12 pages0921Yosalfa Adhista KurniawanNo ratings yet
- Mankir 209Document10 pagesMankir 209Yosalfa Adhista KurniawanNo ratings yet
- Rosadi 219Document20 pagesRosadi 219Yosalfa Adhista KurniawanNo ratings yet
- Jaya 215Document10 pagesJaya 215Yosalfa Adhista KurniawanNo ratings yet
- Anemia During PregnancyDocument8 pagesAnemia During Pregnancyekaseptiani312No ratings yet
- An OCT Study of Anterior Nodular Episcleritis and PDFDocument4 pagesAn OCT Study of Anterior Nodular Episcleritis and PDFYosalfa Adhista KurniawanNo ratings yet
- 0Document2 pages0Yosalfa Adhista KurniawanNo ratings yet
- DepthDocument12 pagesDepthYosalfa Adhista KurniawanNo ratings yet
- 0Document2 pages0Yosalfa Adhista KurniawanNo ratings yet
- Penaloza 2018Document7 pagesPenaloza 2018Yosalfa Adhista KurniawanNo ratings yet
- 0Document2 pages0Yosalfa Adhista KurniawanNo ratings yet
- 0Document2 pages0Yosalfa Adhista KurniawanNo ratings yet
- Alinco DR-135T DR-135E Instruction - Manual PDFDocument47 pagesAlinco DR-135T DR-135E Instruction - Manual PDFYosalfa Adhista KurniawanNo ratings yet
- Discrete POWER & Signal TechnologiesDocument4 pagesDiscrete POWER & Signal TechnologiesArief SaladdinNo ratings yet
- Koljonen 2012Document7 pagesKoljonen 2012Yosalfa Adhista KurniawanNo ratings yet
- NSFWDocument3 pagesNSFWYosalfa Adhista KurniawanNo ratings yet
- N-Channel - Depletion: Semiconductor Technical DataDocument4 pagesN-Channel - Depletion: Semiconductor Technical DataLaAngelitaOropezaNo ratings yet
- Accepted Manuscript: Accident Analysis and PreventionDocument25 pagesAccepted Manuscript: Accident Analysis and PreventionYosalfa Adhista KurniawanNo ratings yet
- A Novel Neurotrophic Drug For Cognitive Enhancement and Alzheimer's DiseaseDocument17 pagesA Novel Neurotrophic Drug For Cognitive Enhancement and Alzheimer's DiseaseYosalfa Adhista KurniawanNo ratings yet
- Parviz I 2003Document13 pagesParviz I 2003Yosalfa Adhista KurniawanNo ratings yet
- Business Analysis FoundationsDocument39 pagesBusiness Analysis FoundationsPriyankaNo ratings yet
- Variables in Language Teaching - The Role of The TeacherDocument34 pagesVariables in Language Teaching - The Role of The TeacherFatin AqilahNo ratings yet
- Internal Peripherals of Avr McusDocument2 pagesInternal Peripherals of Avr McusKuldeep JashanNo ratings yet
- MECHANICAL PROPERTIES OF SOLIDSDocument39 pagesMECHANICAL PROPERTIES OF SOLIDSAbdul Musavir100% (1)
- Hisar CFC - Approved DPRDocument126 pagesHisar CFC - Approved DPRSATYAM KUMARNo ratings yet
- X RayDocument16 pagesX RayMedical Physics2124No ratings yet
- Electrical Design Report For Mixed Use 2B+G+7Hotel BuildingDocument20 pagesElectrical Design Report For Mixed Use 2B+G+7Hotel BuildingEyerusNo ratings yet
- SeparatorDocument2 pagesSeparatormmk111No ratings yet
- Kltdensito2 PDFDocument6 pagesKltdensito2 PDFPutuWijayaKusumaNo ratings yet
- Final - WPS PQR 86Document4 pagesFinal - WPS PQR 86Parag WadekarNo ratings yet
- Digital Water Monitoring and Turbidity Quality System Using MicrocontrollerDocument8 pagesDigital Water Monitoring and Turbidity Quality System Using MicrocontrollerIrin DwiNo ratings yet
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- 19 Unpriced BOM, Project & Manpower Plan, CompliancesDocument324 pages19 Unpriced BOM, Project & Manpower Plan, CompliancesAbhay MishraNo ratings yet
- Mechanical Engineer with Experience in Heavy Mining Machinery MaintenanceDocument1 pageMechanical Engineer with Experience in Heavy Mining Machinery MaintenanceCertified Rabbits LoverNo ratings yet
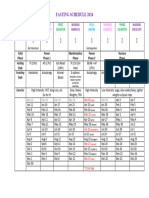
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Ahu, Chiller, Fcu Technical Bid TabulationDocument15 pagesAhu, Chiller, Fcu Technical Bid TabulationJohn Henry AsuncionNo ratings yet
- L Williams ResumeDocument2 pagesL Williams Resumeapi-555629186No ratings yet
- Sia Mock+Test 1 Csat Updated CompressedDocument216 pagesSia Mock+Test 1 Csat Updated Compressedpooja bhatiNo ratings yet
- 5.a Personal Diet Consultant For Healthy MealDocument5 pages5.a Personal Diet Consultant For Healthy MealKishore SahaNo ratings yet
- Design ThinkingDocument16 pagesDesign ThinkingbhattanitanNo ratings yet
- Advanced Presentation Skills: Creating Effective Presentations with Visuals, Simplicity and ClarityDocument15 pagesAdvanced Presentation Skills: Creating Effective Presentations with Visuals, Simplicity and ClarityGilbert TamayoNo ratings yet
- TILE FIXING GUIDEDocument1 pageTILE FIXING GUIDEStavros ApostolidisNo ratings yet
- Week 4 Gen EconDocument10 pagesWeek 4 Gen EconGenner RazNo ratings yet
- EST I - Literacy Test I (Language)Document20 pagesEST I - Literacy Test I (Language)Mohammed Abdallah100% (1)
- ClientsDocument7 pagesClientsLiane PanahacNo ratings yet
- Serendipity - A Sociological NoteDocument2 pagesSerendipity - A Sociological NoteAmlan BaruahNo ratings yet
- English Extra Conversation Club International Women's DayDocument2 pagesEnglish Extra Conversation Club International Women's Dayevagloria11No ratings yet
- 13Document47 pages13Rohan TirmakheNo ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- European Business in China Position Paper 2017 2018 (English Version)Document408 pagesEuropean Business in China Position Paper 2017 2018 (English Version)Prasanth RajuNo ratings yet