You might also like
- Adiel Joy P. Calsa Drug Study March 9, 2022Document5 pagesAdiel Joy P. Calsa Drug Study March 9, 2022Adiel CalsaNo ratings yet
- Fascinating Facts About Phytonutrients in Spices and Healthy Food: Scientifically Proven FactsFrom EverandFascinating Facts About Phytonutrients in Spices and Healthy Food: Scientifically Proven FactsNo ratings yet
- Psychotropic Drug Study in Psychiatry As A Nursing SpecialtyDocument4 pagesPsychotropic Drug Study in Psychiatry As A Nursing SpecialtyRoland YusteNo ratings yet
- Salazar Medsurg Drug StudyDocument2 pagesSalazar Medsurg Drug StudyAlyssa Marie PepitoNo ratings yet
- Salazar Medsurg Drug StudyDocument26 pagesSalazar Medsurg Drug StudyAlyssa Marie PepitoNo ratings yet
- Valproic Acid Drug Study PDFDocument4 pagesValproic Acid Drug Study PDFLiza Marie IgnacioNo ratings yet
- Drug Study: Atropine: RecommendedDocument6 pagesDrug Study: Atropine: RecommendedShara Lailanie A. AzisNo ratings yet
- Drug Study - Magnesium SulfateDocument6 pagesDrug Study - Magnesium SulfatePrincess Alane MorenoNo ratings yet
- AcetaminophenDocument3 pagesAcetaminophenShaira Tan100% (1)
- Valproic Acid Drug StudyDocument4 pagesValproic Acid Drug StudyJeyser T. Gamutia100% (1)
- Drug Study ParacetamolDocument2 pagesDrug Study ParacetamolDannah BulliandayNo ratings yet
- Drug Study 5Document4 pagesDrug Study 5Butts McgeeNo ratings yet
- PharmacologyDocument10 pagesPharmacologyPrince Mark Badillo100% (2)
- Magnesium SulfateDocument6 pagesMagnesium SulfatePrincess Alane MorenoNo ratings yet
- Belarmino Drugstudy2Document7 pagesBelarmino Drugstudy2KakaiNo ratings yet
- Medication Sheet TMDocument4 pagesMedication Sheet TMapi-544317178No ratings yet
- Kineme Case StudyDocument8 pagesKineme Case Studyislafab25No ratings yet
- Hydralazine.1 3Document1 pageHydralazine.1 3SNo ratings yet
- Drug Study MetoclopramideDocument2 pagesDrug Study Metoclopramiderica sebabillones100% (1)
- Drug Study: Nursing DepartmentDocument2 pagesDrug Study: Nursing Departmentrica sebabillones100% (1)
- Propofol Drug StudyDocument3 pagesPropofol Drug StudyAngelica shane Navarro100% (2)
- DRUG STUDY - FurosemideDocument2 pagesDRUG STUDY - FurosemideVANESSA PAULA ALGADORNo ratings yet
- Santiago, Gwyneth Julia B. - Drug MonographDocument1 pageSantiago, Gwyneth Julia B. - Drug MonographGwyneth SantiagoNo ratings yet
- Drug Study: Batangas State UniversityDocument8 pagesDrug Study: Batangas State UniversityFreya Janina ReyesNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- DRUG-STUDY TramadolDocument2 pagesDRUG-STUDY TramadolkitsimonmondinNo ratings yet
- Drug Study SertralineDocument5 pagesDrug Study SertralineJose Luis Hernandez50% (2)
- Case Study (20%) : Know Your MedicineDocument11 pagesCase Study (20%) : Know Your MedicineMOHD MU'IZZ BIN MOHD SHUKRINo ratings yet
- I. Drug Study: Drug Mechanism of Action Indications Contraindication Side Effects Nursing ConsiderationsDocument3 pagesI. Drug Study: Drug Mechanism of Action Indications Contraindication Side Effects Nursing Considerationscyn yana0723No ratings yet
- Ca PharmacologyDocument5 pagesCa Pharmacology88annemariNo ratings yet
- Exam 1 Drug ResumeDocument8 pagesExam 1 Drug Resumecpmv0410No ratings yet
- Bumetanide MIMSDocument2 pagesBumetanide MIMSIndri WahyuniNo ratings yet
- MisoprostolDocument5 pagesMisoprostolkristenerika100% (2)
- Generic Name: Brand Name: Pharmacologic Class: Action: CNS: DizzinessDocument8 pagesGeneric Name: Brand Name: Pharmacologic Class: Action: CNS: DizzinessMaricon BautistaNo ratings yet
- Medication Generic/Brand Classification Nursing Implications (3) Dosage Route Schedule /time Desired Effect Side Effects (3) TeachingDocument5 pagesMedication Generic/Brand Classification Nursing Implications (3) Dosage Route Schedule /time Desired Effect Side Effects (3) TeachingrunnermnNo ratings yet
- RanitidineDocument3 pagesRanitidineJoshua PenggeleNo ratings yet
- LabetalolDocument3 pagesLabetalolTri Purma Sari50% (2)
- Drug Study of TBDocument7 pagesDrug Study of TBMarc AntonioNo ratings yet
- Nausea and Vomiting Nausea and VomitingDocument6 pagesNausea and Vomiting Nausea and VomitingTHERESA CLAIRE ENCINARESNo ratings yet
- 4 SeizuresDocument11 pages4 SeizuresApple MaeNo ratings yet
- 7endocrine DrugsDocument2 pages7endocrine DrugsSOFIA ALYSSA MARIE ABUDENo ratings yet
- Metocloprramide HydrochlorideDocument2 pagesMetocloprramide HydrochlorideBeatrizz P GellaNo ratings yet
- Medications: Medication Name Generic/Trade Classification Pregnancy CategoryDocument8 pagesMedications: Medication Name Generic/Trade Classification Pregnancy CategoryapalestiNo ratings yet
- Elbert A. Mutuc Drug Study BSN III - 1 Group 2Document4 pagesElbert A. Mutuc Drug Study BSN III - 1 Group 2Elbert Aquitania Mutuc RNNo ratings yet
- Pomr Mik SK 4 NeewwDocument4 pagesPomr Mik SK 4 NeewwDewi Ayu CahyaningrumNo ratings yet
- Drug StudyDocument6 pagesDrug StudyRosemarie CarpioNo ratings yet
- Drug Study: Aspirin (Asa)Document5 pagesDrug Study: Aspirin (Asa)Shara Lailanie A. AzisNo ratings yet
- Drugs Study Post VaricocoelectomyDocument2 pagesDrugs Study Post VaricocoelectomyIris CaberteNo ratings yet
- MetoclopramideDocument1 pageMetoclopramideIvanne Hisoler89% (27)
- Improper Administration Silent Culprit of Drug Therapy ProblemsDocument6 pagesImproper Administration Silent Culprit of Drug Therapy Problemsadern-07huepfendNo ratings yet
- Drug Study SurgeryDocument1 pageDrug Study SurgerygorgeazNo ratings yet
- Brand Name: Generic Name: Drug ClassificationDocument2 pagesBrand Name: Generic Name: Drug ClassificationChristine Pialan SalimbagatNo ratings yet
- DRUG STUDYxNCP - WEEK2 - ST - VICTORIADocument8 pagesDRUG STUDYxNCP - WEEK2 - ST - VICTORIAKent Martin AmorosoNo ratings yet
- J.H. Cerilles State CollegeDocument27 pagesJ.H. Cerilles State CollegeJonna JuntillaNo ratings yet
- Vii. Drug Study: Parkinsonis M. Pheochrom Ocytoma (Risk of Hypertensiv e Crisis)Document5 pagesVii. Drug Study: Parkinsonis M. Pheochrom Ocytoma (Risk of Hypertensiv e Crisis)Darwin AndalNo ratings yet
- Risperidone Drug StudyDocument2 pagesRisperidone Drug StudyLanzen DragneelNo ratings yet
- DRUG Study PiyaliDocument10 pagesDRUG Study PiyaliPiyali SahaNo ratings yet
- Generic Name: Ordered: Indications: Contraindications BeforeDocument3 pagesGeneric Name: Ordered: Indications: Contraindications BeforeChenime Añana0% (1)
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale Evaluation Short Term Goal Independent: Short Term GoalDocument5 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale Evaluation Short Term Goal Independent: Short Term GoalJobelle AcenaNo ratings yet
- Date/Schedule Activities Expected Output Verified/Checked by Area in ChargeDocument2 pagesDate/Schedule Activities Expected Output Verified/Checked by Area in ChargeJobelle AcenaNo ratings yet
- GC ncp1 and 2Document4 pagesGC ncp1 and 2Jobelle AcenaNo ratings yet
- Case StudyDocument10 pagesCase StudyJobelle AcenaNo ratings yet
- NCM 107 Leadership and Management RLEDocument4 pagesNCM 107 Leadership and Management RLEJobelle AcenaNo ratings yet
- Geriatric Case StudyDocument15 pagesGeriatric Case StudyJobelle AcenaNo ratings yet
- Pediatric Case StudyDocument21 pagesPediatric Case StudyJobelle AcenaNo ratings yet
- NCM 107 SY 2020-2021: Legal and Ethical Consideration of Euthanasia in India: A Choice Between Life and DeathDocument8 pagesNCM 107 SY 2020-2021: Legal and Ethical Consideration of Euthanasia in India: A Choice Between Life and DeathJobelle AcenaNo ratings yet
- Union Christian College School of Health and Sciences City of San Fernando La UnionDocument11 pagesUnion Christian College School of Health and Sciences City of San Fernando La UnionJobelle AcenaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (2)
- GC ncp1Document2 pagesGC ncp1Jobelle AcenaNo ratings yet
- NCPsDocument11 pagesNCPsJobelle AcenaNo ratings yet
- Case Study (ACS)Document12 pagesCase Study (ACS)Kristel Joy Cabarrubias Acena100% (1)
- Case Study (Lung Cancer)Document17 pagesCase Study (Lung Cancer)Jobelle Acena100% (1)
- DRUG STUDY (Lung Cancer)Document10 pagesDRUG STUDY (Lung Cancer)Jobelle AcenaNo ratings yet
- Subjective: Ventilation AssistanceDocument3 pagesSubjective: Ventilation AssistanceJobelle Acena100% (2)
- Er Drugs StudyDocument80 pagesEr Drugs StudyJobelle AcenaNo ratings yet
- ER Protocols in The PhilippinesDocument9 pagesER Protocols in The PhilippinesJobelle Acena100% (1)
- Diagnostic Tests PDFDocument2 pagesDiagnostic Tests PDFBenedict AlvarezNo ratings yet
- Normal Cell GrowthDocument5 pagesNormal Cell GrowthJobelle AcenaNo ratings yet
- Difference Between Mechanism of Action of Cell Mediated Immune System and Humoral Mediated Immune SystemDocument4 pagesDifference Between Mechanism of Action of Cell Mediated Immune System and Humoral Mediated Immune SystemJobelle AcenaNo ratings yet
- Online LectureDocument9 pagesOnline LectureJobelle AcenaNo ratings yet
- SummaryDocument1 pageSummaryJobelle AcenaNo ratings yet
- Bioethics in Nursing Practice PDFDocument5 pagesBioethics in Nursing Practice PDFVhinny Macabontoc100% (1)
- Anti Psychotic DrugsDocument2 pagesAnti Psychotic DrugscalfornianursingacadNo ratings yet
- Nursing: Core Values of NursingDocument14 pagesNursing: Core Values of NursingJobelle AcenaNo ratings yet
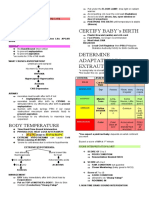
- Certify Baby'S Birth: Body TemperatureDocument9 pagesCertify Baby'S Birth: Body TemperatureJobelle Acena100% (1)
- Psychiatric Nursing Michael Jimenez, PENTAGON Slovin'S Formula: N 1 + NeDocument10 pagesPsychiatric Nursing Michael Jimenez, PENTAGON Slovin'S Formula: N 1 + NeJobelle AcenaNo ratings yet
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Document22 pagesNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
- The Unified Parkinson's Disease Rating Scale (UPDRS) : Status and RecommendationsDocument13 pagesThe Unified Parkinson's Disease Rating Scale (UPDRS) : Status and RecommendationscaisarNo ratings yet
- CHC33015-AC-HACC-Subject 4-AWB-F-v2.5Document45 pagesCHC33015-AC-HACC-Subject 4-AWB-F-v2.5Ashesh Basnet100% (6)
- Diagnosis and Treatment of Parkinson Disease A ReviewDocument13 pagesDiagnosis and Treatment of Parkinson Disease A ReviewTarcisioNo ratings yet
- 2.1 Cognitive and Degenerative DisordersDocument73 pages2.1 Cognitive and Degenerative DisordersAbanoub AwadallaNo ratings yet
- Parkinson Disease SlidesDocument21 pagesParkinson Disease Slidessarah morley100% (1)
- Movement Disorders: Prof. DR Taha Kamel Alloush MD NeurologyDocument68 pagesMovement Disorders: Prof. DR Taha Kamel Alloush MD NeurologyKhaled OssamaNo ratings yet
- Management of Patients With Oncologic or Degenerative Neurologic DisordersDocument84 pagesManagement of Patients With Oncologic or Degenerative Neurologic DisordersDwiKrismaPratabaNo ratings yet
- List of DiseasesDocument13 pagesList of DiseasesHans Siegfred SaynoNo ratings yet
- Neurogenic Disorders of The LarynxDocument37 pagesNeurogenic Disorders of The LarynxSyaffira SalsabilaNo ratings yet
- PHARMACY MCQ Quiz 1Document18 pagesPHARMACY MCQ Quiz 1Noah MrjNo ratings yet
- CNS Notes: By: Dr. Abdullah NouhDocument40 pagesCNS Notes: By: Dr. Abdullah NouhHythem HashimNo ratings yet
- Antiparkinsonian DrugsDocument4 pagesAntiparkinsonian DrugsnurseoncervixNo ratings yet
- Neurological NCLEX Points PDFDocument17 pagesNeurological NCLEX Points PDFLillianNo ratings yet
- ParkinsonDocument3 pagesParkinsonRJean TumalaNo ratings yet
- 3.current Pharmaceutical Treatments and Alternative Therapies ofDocument17 pages3.current Pharmaceutical Treatments and Alternative Therapies ofPaula Betancor MontesdeocaNo ratings yet
- Group 1 Parkinsons Pre TestDocument4 pagesGroup 1 Parkinsons Pre TestAyman NabilNo ratings yet
- DR A.A.Ayu Meidiary, SPS: Department of Neurology, Sanglah General Hospital, Udayana University DenpasarDocument47 pagesDR A.A.Ayu Meidiary, SPS: Department of Neurology, Sanglah General Hospital, Udayana University DenpasarKertiasihwayanNo ratings yet
- Parkinson's DiseaseDocument28 pagesParkinson's DiseaseJan Michael CorpuzNo ratings yet
- Parkinson DiseaseDocument10 pagesParkinson DiseaseparthibaneNo ratings yet
- Pyramid & Extrapyramidal DisordersDocument5 pagesPyramid & Extrapyramidal Disordersjoelh9No ratings yet
- Check - August - Unit 552 - Neurology PDFDocument32 pagesCheck - August - Unit 552 - Neurology PDFdragon66No ratings yet
- Proprioception, Vestibular & CoordinationDocument28 pagesProprioception, Vestibular & Coordinationzm2h8hpsq8No ratings yet
- LSVT LOUD and LSVT BIG PDFDocument12 pagesLSVT LOUD and LSVT BIG PDFRicardo Villagra AstudilloNo ratings yet
- Basal GangliaDocument6 pagesBasal Ganglia381a53c99bNo ratings yet
- BSN3A Summative Test (Prelim)Document16 pagesBSN3A Summative Test (Prelim)Emuelle GanNo ratings yet
- Neurology Past Years Before EhsanDocument345 pagesNeurology Past Years Before EhsanMohammad AlrefaiNo ratings yet
- STN GPi RematchDocument4 pagesSTN GPi Rematchberna chuaNo ratings yet
- Anatomía Funcional de Los Ganglios Basales: M. Merello, A. CammarotaDocument6 pagesAnatomía Funcional de Los Ganglios Basales: M. Merello, A. CammarotaIván DelgadoNo ratings yet
- Reporter: Degenerative Diseases of The Central Nervous System (CNS) Parkinson's DiseaseDocument6 pagesReporter: Degenerative Diseases of The Central Nervous System (CNS) Parkinson's DiseaseMelody B. MiguelNo ratings yet
- Parkinson S DiseaseDocument91 pagesParkinson S DiseaseTrisha TolentinoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)