You might also like
- Botanical Medicine From Bench To Bedside PDFDocument237 pagesBotanical Medicine From Bench To Bedside PDFdrzacherg100% (1)
- Card RepertoryDocument6 pagesCard RepertorySuhas IngaleNo ratings yet
- Risk For Falls Aeb Loss of BalanceDocument4 pagesRisk For Falls Aeb Loss of BalanceAlexandrea MayNo ratings yet
- FLUOROURACIL Drug StudyDocument8 pagesFLUOROURACIL Drug StudyAlexandrea MayNo ratings yet
- Gordons Functional Health PatternsDocument12 pagesGordons Functional Health PatternsAlexandrea MayNo ratings yet
- Lower Limb Trauma - 5Document12 pagesLower Limb Trauma - 5Renee RoSeNo ratings yet
- The Pharmacist Guide To Implementing Pharmaceutical Care PDFDocument502 pagesThe Pharmacist Guide To Implementing Pharmaceutical Care PDFLuis SosaNo ratings yet
- Drug study on isoxsuprine, decamethasone, nalbuphineDocument17 pagesDrug study on isoxsuprine, decamethasone, nalbuphineArnold ZamoroNo ratings yet
- Final Adime Note AnemiacasestudyDocument2 pagesFinal Adime Note Anemiacasestudyapi-253526841No ratings yet
- Nutritious Meals for Pregnant and Lactating WomenDocument4 pagesNutritious Meals for Pregnant and Lactating WomenKariza Perdido100% (1)
- Fluorouracil Drug StudyDocument8 pagesFluorouracil Drug StudyAlexandrea MayNo ratings yet
- Drug StudyDocument14 pagesDrug StudyRaff GutierrezNo ratings yet
- Dobutamine Drug StudyDocument5 pagesDobutamine Drug StudyAlexandrea MayNo ratings yet
- Acyclovir (Acycloguanosi Ne) : Systemic Administration History: AllergyDocument3 pagesAcyclovir (Acycloguanosi Ne) : Systemic Administration History: AllergyAnnahNo ratings yet
- A Drug Study On MISOPROSTOLDocument6 pagesA Drug Study On MISOPROSTOLAlexandrea MayNo ratings yet
- NCP EsrfDocument9 pagesNCP EsrfKen RegalaNo ratings yet
- Paracetamol Biogesic Analgesic AntipyreticDocument8 pagesParacetamol Biogesic Analgesic AntipyreticGian Era100% (1)
- Drug StudyDocument3 pagesDrug StudyGena Manimtim100% (1)
- College of Nursing: Rifadin RifampinDocument4 pagesCollege of Nursing: Rifadin RifampinAnika PleñosNo ratings yet
- Drug StudyDocument4 pagesDrug StudyAli Longasa CortezNo ratings yet
- Respiratory Drug Study GuideDocument23 pagesRespiratory Drug Study GuideAdrienne Nicole PaneloNo ratings yet
- Drug Study Ferrous SulfateDocument2 pagesDrug Study Ferrous SulfateBunnie AlphaNo ratings yet
- Drug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument1 pageDrug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesJonna Mae TurquezaNo ratings yet
- Glycerin: (Gli-Ser-In)Document2 pagesGlycerin: (Gli-Ser-In)Aryanto DedyNo ratings yet
- CiprofloxacinDocument2 pagesCiprofloxacinx483xDNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument43 pagesSee Full Prescribing Information For Complete Boxed WarningParishan SaeedNo ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocument4 pagesTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNo ratings yet
- GitDocument302 pagesGitjgcriste100% (7)
- Drug StudyDocument2 pagesDrug Studyunkown userNo ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- GUAIFENESINDocument1 pageGUAIFENESINAngel CatalanNo ratings yet
- Generics Act promotes use of generic drug namesDocument5 pagesGenerics Act promotes use of generic drug namesKatrina Javier BolivarNo ratings yet
- Nursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationMarielle Chua100% (1)
- HES 005 P2 Coverage and Drug Study GuideDocument4 pagesHES 005 P2 Coverage and Drug Study GuideXander Jake Asturias TangcalaganNo ratings yet
- Betahistine Dihydrochloride (Serc) 1aDocument3 pagesBetahistine Dihydrochloride (Serc) 1aGirlie Jane Sevillano RNNo ratings yet
- Physician's Orders for Admission and Treatment of Epigastric PainDocument4 pagesPhysician's Orders for Admission and Treatment of Epigastric PainJerremy LuqueNo ratings yet
- Nutrition Care Process and ModelDocument82 pagesNutrition Care Process and ModelNoci M. FrenkNo ratings yet
- Nursing Process in Community HealthDocument41 pagesNursing Process in Community HealthKim Bok JooNo ratings yet
- PHINMA Nursing Drug StudyDocument2 pagesPHINMA Nursing Drug StudyArianne NicoleNo ratings yet
- Supersize Me by Morgan Spurlock 1Document7 pagesSupersize Me by Morgan Spurlock 1api-317451959No ratings yet
- NCP and Drug Study Forms FINALDocument9 pagesNCP and Drug Study Forms FINALVince Troy AquinoNo ratings yet
- Clinical Medications Worksheets: (Why Med Ordered) Contraindications/warnings/interactionsDocument1 pageClinical Medications Worksheets: (Why Med Ordered) Contraindications/warnings/interactionsENo ratings yet
- Drug Study MetoprololDocument2 pagesDrug Study MetoprololHannah Angelu CabadingNo ratings yet
- High Risk PreschoolerDocument7 pagesHigh Risk PreschoolerAngela Del CastilloNo ratings yet
- ACALKADocument1 pageACALKAErnie LaraNo ratings yet
- OB Drug StudyDocument12 pagesOB Drug StudyCj AttoNo ratings yet
- LRDR ProceduresDocument67 pagesLRDR ProceduresJustJ ThingsNo ratings yet
- Management of Upper GI BleedingDocument55 pagesManagement of Upper GI BleedingNatnaelNo ratings yet
- Bactrim drug info for nursesDocument2 pagesBactrim drug info for nursesMark BarengNo ratings yet
- MotiliumDocument5 pagesMotiliumAkram KhanNo ratings yet
- Mfe, Ferrous Sulfate, Calcium Drug StudyDocument3 pagesMfe, Ferrous Sulfate, Calcium Drug StudyMary Shane MoraldeNo ratings yet
- Celecoxib CelebrexDocument1 pageCelecoxib CelebrexBeverly Ann de LeonNo ratings yet
- Furosemide ChlorthalidoneDocument5 pagesFurosemide ChlorthalidoneLIEZEL GRACE VELAYONo ratings yet
- LansoprazoleDocument3 pagesLansoprazoleJody FelizioNo ratings yet
- NCP Risk InfectionDocument1 pageNCP Risk InfectionEni RahmawatiNo ratings yet
- RevisionDocument17 pagesRevisionMatt RenaudNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJay-ar Batara SorianoNo ratings yet
- Public Health Nurse ProceduresDocument9 pagesPublic Health Nurse ProcedureskzbreakerrNo ratings yet
- Brand Name: Generic Name: Drug ClassificationDocument2 pagesBrand Name: Generic Name: Drug ClassificationChristine Pialan SalimbagatNo ratings yet
- Drug StudyDocument5 pagesDrug StudyRai D. MacapantonNo ratings yet
- Feeding Pregnant and Lactating WomenDocument1 pageFeeding Pregnant and Lactating WomenJOHANNA VENN CASTUERANo ratings yet
- Folic Acid Benefits, Uses, Side EffectsDocument3 pagesFolic Acid Benefits, Uses, Side EffectsDadybooboo2013No ratings yet
- Viii. Pharmacologic Intervention (Drug Study)Document10 pagesViii. Pharmacologic Intervention (Drug Study)Cyril Jane Caanyagan AcutNo ratings yet
- FentanylDocument4 pagesFentanylapi-3797941No ratings yet
- VerA Ok-Prelim Ncm104 (Autosaved) VeraDocument30 pagesVerA Ok-Prelim Ncm104 (Autosaved) Verajesperdomincilbayaua100% (1)
- Zofran (Ondansetron)Document3 pagesZofran (Ondansetron)ENo ratings yet
- Propylthiouracil (PTU) Drug StudyDocument7 pagesPropylthiouracil (PTU) Drug StudyAlexandrea MayNo ratings yet
- Propylthiouracil DSDocument6 pagesPropylthiouracil DSAlexandrea MayNo ratings yet
- Drug Study On PtuDocument4 pagesDrug Study On PtuDizzy BualanNo ratings yet
- Method GDMDocument17 pagesMethod GDMAlexandrea MayNo ratings yet
- Lipitor A Drug Study OnDocument7 pagesLipitor A Drug Study OnAlexandrea MayNo ratings yet
- DS Drug METFORMINDocument4 pagesDS Drug METFORMINAlexandrea MayNo ratings yet
- Lipitor A Drug Study OnDocument8 pagesLipitor A Drug Study OnAlexandrea MayNo ratings yet
- Understanding Loss of Appetite: Causes, Symptoms and Treatment OptionsDocument8 pagesUnderstanding Loss of Appetite: Causes, Symptoms and Treatment OptionsAlexandrea MayNo ratings yet
- A Drug Study On: PhenylephrineDocument6 pagesA Drug Study On: PhenylephrineAlexandrea MayNo ratings yet
- A Nursing Care Plan Presented To The Faculty of The Nursing DepartmentDocument8 pagesA Nursing Care Plan Presented To The Faculty of The Nursing DepartmentAlexandrea MayNo ratings yet
- Risk For Falls As Evidence by Loss of BalanceDocument4 pagesRisk For Falls As Evidence by Loss of BalanceAlexandrea MayNo ratings yet
- Discharge plan for bleeding peptic ulcerDocument5 pagesDischarge plan for bleeding peptic ulcerAlexandrea MayNo ratings yet
- Lipitor Drug Study for Emergency NursingDocument8 pagesLipitor Drug Study for Emergency NursingAlexandrea MayNo ratings yet
- NCM 218 RLE IncompleteDocument30 pagesNCM 218 RLE IncompleteAlexandrea MayNo ratings yet
- Lipitor Drug Study for Emergency NursingDocument8 pagesLipitor Drug Study for Emergency NursingAlexandrea MayNo ratings yet
- Fluorouracil DSDocument7 pagesFluorouracil DSAlexandrea MayNo ratings yet
- Propylthiouracil DSDocument6 pagesPropylthiouracil DSAlexandrea MayNo ratings yet
- Dobutamine DSDocument5 pagesDobutamine DSAlexandrea MayNo ratings yet
- Propylthiouracil (PTU) Drug StudyDocument7 pagesPropylthiouracil (PTU) Drug StudyAlexandrea MayNo ratings yet
- PDFDocument14 pagesPDFmuhammad rustamNo ratings yet
- OVERVIEW Rapid Sequence Intubation (RSI) Is An Airway Management Technique That ProducesDocument7 pagesOVERVIEW Rapid Sequence Intubation (RSI) Is An Airway Management Technique That ProducesOkami PNo ratings yet
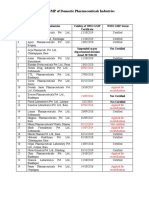
- Status of Nepali Pharma GMP CertificationDocument2 pagesStatus of Nepali Pharma GMP CertificationDapper Yourself100% (1)
- Procedures and Notes for Medical SpecialtiesDocument9 pagesProcedures and Notes for Medical SpecialtiesKeith CoralNo ratings yet
- Discussion and ConclusionDocument4 pagesDiscussion and ConclusionRisma WerdaningsihNo ratings yet
- A Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination ProductsDocument11 pagesA Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination Productsarief hakikiNo ratings yet
- Management of Local Anesthetic Complications: Ross Camiel, Samuel Roh, and Christy LottingerDocument10 pagesManagement of Local Anesthetic Complications: Ross Camiel, Samuel Roh, and Christy LottingerErryskaNo ratings yet
- Medisend 12-12-2023Document31 pagesMedisend 12-12-2023Nafilah SyellaNo ratings yet
- Osteoarthritis and Fibromyalgia: by Tamara MitchellDocument13 pagesOsteoarthritis and Fibromyalgia: by Tamara MitchellmailbabuNo ratings yet
- Essential List On 5th November 2022Document9 pagesEssential List On 5th November 2022AFI FARMANo ratings yet
- Transformations of Morphine Alkaloids by Pseudomonas Putida M10Document5 pagesTransformations of Morphine Alkaloids by Pseudomonas Putida M10Paul SpadesNo ratings yet
- College of Nursing: Pharmacological ManagementDocument3 pagesCollege of Nursing: Pharmacological ManagementAnika PleñosNo ratings yet
- Compound Effervescent Powder FormulaDocument4 pagesCompound Effervescent Powder FormulaJonille EchevarriaNo ratings yet
- Antiplatelet and Anticoagulation GuideDocument31 pagesAntiplatelet and Anticoagulation GuideMarcelliaNo ratings yet
- Pharmacognosy Assignment: 3 Prof. Pharm - D (Evening)Document7 pagesPharmacognosy Assignment: 3 Prof. Pharm - D (Evening)Neha GulfamNo ratings yet
- omeprazole-drug-studyDocument7 pagesomeprazole-drug-studyFedericee AbellanaNo ratings yet
- 2 - AnsDocument21 pages2 - Ansyahomed519No ratings yet
- CTD Table of Contents Secti ON SUB Section Content NumberDocument4 pagesCTD Table of Contents Secti ON SUB Section Content Numberhenrykayode4No ratings yet
- Programme-Wise List of PublicationsDocument15 pagesProgramme-Wise List of PublicationsMikel MillerNo ratings yet
- Ontent Reviewers: ContributorsDocument14 pagesOntent Reviewers: ContributorsAgnes TanicNo ratings yet
- PRICE LIST PT EFFATA FAJAR ANUGERAH 2022Document10 pagesPRICE LIST PT EFFATA FAJAR ANUGERAH 2022malydaNo ratings yet
- Lab Activity #1Document5 pagesLab Activity #1Meg Angela Cirunay-Decena0% (1)
- Maya Biotech Private LimitedDocument21 pagesMaya Biotech Private LimitedRusan PNo ratings yet
- 309 Lab ReportDocument8 pages309 Lab ReportZorina Bi0% (1)
- Prometric ExamsDocument2 pagesPrometric ExamsRam KumarNo ratings yet