You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Day Study Schedule For USMLE Step 1 LecturioDocument12 pagesDay Study Schedule For USMLE Step 1 LecturioDany Paulbaby100% (1)
- A Drug For IntDocument58 pagesA Drug For IntVajirawit PetchsriNo ratings yet
- Recognizing Free AirDocument12 pagesRecognizing Free AirVajirawit PetchsriNo ratings yet
- Recognizing PneumothoraxDocument32 pagesRecognizing PneumothoraxVajirawit PetchsriNo ratings yet
- Screening TestsDocument16 pagesScreening TestsVajirawit PetchsriNo ratings yet
- Recognizing Tube and LineDocument57 pagesRecognizing Tube and LineVajirawit PetchsriNo ratings yet
- Recognizing Opacified HemithoraxDocument15 pagesRecognizing Opacified HemithoraxVajirawit PetchsriNo ratings yet
- Back PainDocument16 pagesBack PainVajirawit PetchsriNo ratings yet
- GI BleedDocument12 pagesGI BleedVajirawit PetchsriNo ratings yet
- Anemia PDFDocument14 pagesAnemia PDFVajirawit PetchsriNo ratings yet
- DiarrheaDocument13 pagesDiarrheaVajirawit PetchsriNo ratings yet
- Abdominal PainDocument23 pagesAbdominal PainVajirawit PetchsriNo ratings yet
- AnemiaDocument14 pagesAnemiaVajirawit PetchsriNo ratings yet
- VentilatorDocument5 pagesVentilatorVajirawit PetchsriNo ratings yet
- Common Drug Use in Adult For ExternDocument5 pagesCommon Drug Use in Adult For ExternVajirawit PetchsriNo ratings yet
- 10 - Histology Lecture, Structure of Muscular TissueDocument37 pages10 - Histology Lecture, Structure of Muscular TissueAMIRA HELAYELNo ratings yet
- Lec6 - Circulatory SystemDocument4 pagesLec6 - Circulatory SystemEloisa Trina GenerosoNo ratings yet
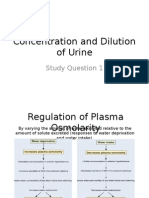
- Regulation of Urine Concentration and DilutionDocument20 pagesRegulation of Urine Concentration and DilutionNeil Alcantara SantiNo ratings yet
- 3.4 Process of Absorption and Transportation of Digested Food and DefecationDocument13 pages3.4 Process of Absorption and Transportation of Digested Food and DefecationAthirah SulaimanNo ratings yet
- Hypothyroidism and Hyperthyroidism TreatmentDocument6 pagesHypothyroidism and Hyperthyroidism TreatmentMaria MushtaqueNo ratings yet
- MS System SummaryDocument16 pagesMS System SummaryChelo Jan GeronimoNo ratings yet
- Newborn Care Guide: Assessment, Feeding, Development & MoreDocument73 pagesNewborn Care Guide: Assessment, Feeding, Development & MoreKarjana183No ratings yet
- Sleep and The BrainDocument32 pagesSleep and The Brainneb atairpacNo ratings yet
- Submandibular Region AnatomyDocument32 pagesSubmandibular Region AnatomyDrRj SameenNo ratings yet
- Contoh EBLDocument4 pagesContoh EBLsalsabila fabianca alsaidNo ratings yet
- 2021 Article 605Document17 pages2021 Article 605Flor VelasquezNo ratings yet
- Anatomy Central Nervous SystemDocument87 pagesAnatomy Central Nervous SystemMusfira KhalidNo ratings yet
- Anatomy and Physiology OverviewDocument44 pagesAnatomy and Physiology OverviewKRISTIAN DRAZEN MIRANDANo ratings yet
- Module in Scie 6 - 2nd QuarterDocument13 pagesModule in Scie 6 - 2nd QuarterCarla AnnabellanaNo ratings yet
- Endocrine System NotesDocument8 pagesEndocrine System NotesShiela Mae SagayoNo ratings yet
- 10 - 40 - Sensory and Motor Areas of The Cerebral Cortex IDocument22 pages10 - 40 - Sensory and Motor Areas of The Cerebral Cortex IAhmed TarekNo ratings yet
- Abnormal LFTsDocument2 pagesAbnormal LFTsRenu RosyNo ratings yet
- Sense Organs and Their FunctionsDocument2 pagesSense Organs and Their FunctionsMario Miguel FlorNo ratings yet
- 1st Lecture On Histology of Nervous Tissue by Dr. RoomiDocument14 pages1st Lecture On Histology of Nervous Tissue by Dr. RoomiMudassar RoomiNo ratings yet
- Gladys Cheing RS3030 CNN Introduction To Neuroscience Note 2021Document73 pagesGladys Cheing RS3030 CNN Introduction To Neuroscience Note 2021Tsang AmyNo ratings yet
- Medical AstrologyDocument49 pagesMedical AstrologyVicaas VS100% (1)
- Science10 Q3 SLM4Document15 pagesScience10 Q3 SLM4Jomelyn Arzaga100% (2)
- Electrocardiography: Prepared by A.Devasena, Associate Professor, Dhanalakshmi College of Engineering, Chennai 1Document25 pagesElectrocardiography: Prepared by A.Devasena, Associate Professor, Dhanalakshmi College of Engineering, Chennai 1Sebastin SureshNo ratings yet
- Digestive System Workshop For Kids by SlidesgoDocument16 pagesDigestive System Workshop For Kids by Slidesgoapi-649419165No ratings yet
- Human Histo and Embryo Module 2Document7 pagesHuman Histo and Embryo Module 2KynazNo ratings yet
- 03 Life Processes Chapter Wise Important QuestionsDocument17 pages03 Life Processes Chapter Wise Important Questionsmm8871100% (1)
- GIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiDocument41 pagesGIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiMudassar Roomi86% (14)
- Abdomen: Radiology RevisionDocument11 pagesAbdomen: Radiology RevisionhimaniNo ratings yet