You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 2.2 Research 1 SKSKKDocument164 pages2.2 Research 1 SKSKKKaiken DukeNo ratings yet
- 3.1 Research 1Document10 pages3.1 Research 1Kaiken DukeNo ratings yet
- April 2021 - March 2022Document12 pagesApril 2021 - March 2022Kaiken DukeNo ratings yet
- Far Eastern University - Nicanor Reyes Medical Foundation: VISION: 20 - 20 (1C)Document5 pagesFar Eastern University - Nicanor Reyes Medical Foundation: VISION: 20 - 20 (1C)Kaiken DukeNo ratings yet
- Research 1 FinalsDocument81 pagesResearch 1 FinalsKaiken DukeNo ratings yet
- 1.1 Normality PDFDocument2 pages1.1 Normality PDFKaiken DukeNo ratings yet
- Electric Portable Hand MixerDocument1 pageElectric Portable Hand MixerKaiken DukeNo ratings yet
- USMLE DNA RNA VirusesDocument13 pagesUSMLE DNA RNA VirusesKaiken DukeNo ratings yet
- Pt's ECG: Sinus Tachycardia, Left Axis Deviation, Anterolateral Wall IschemiaDocument3 pagesPt's ECG: Sinus Tachycardia, Left Axis Deviation, Anterolateral Wall IschemiaKaiken DukeNo ratings yet
- Community Assessment Tools: A Companion Piece To Communities in ActionDocument12 pagesCommunity Assessment Tools: A Companion Piece To Communities in ActionDranreb Berylle MasangkayNo ratings yet
- General Assessment: Additional Notes: BlueDocument4 pagesGeneral Assessment: Additional Notes: BlueKaiken DukeNo ratings yet
- And Brought Him To An Inn... "Document7 pagesAnd Brought Him To An Inn... "Kaiken DukeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pertussis: PDF, 667kbDocument2 pagesPertussis: PDF, 667kbRaissa DeaNo ratings yet
- TYPHOID FEVER and HEPATITIS ADocument25 pagesTYPHOID FEVER and HEPATITIS AMaelleNo ratings yet
- Makalah SelulitisDocument26 pagesMakalah Selulitisdr WiyogoNo ratings yet
- (PAR) 3.04 Medical Entomology-EduardoDocument12 pages(PAR) 3.04 Medical Entomology-EduardoFerdie Jacinto Goyena100% (1)
- Blood Transfusion FormDocument2 pagesBlood Transfusion FormGMCH LaboratoryNo ratings yet
- Mastermind: WorksheetDocument23 pagesMastermind: WorksheetMilka RahmanNo ratings yet
- LAS Q3-Health8-Week-6-8Document8 pagesLAS Q3-Health8-Week-6-8novem salonoyNo ratings yet
- Acute Flaccid Paralysis Surveillance PDFDocument1 pageAcute Flaccid Paralysis Surveillance PDFMutiara DewiNo ratings yet
- List of Viruses Covered Under NCS-TCPDocument5 pagesList of Viruses Covered Under NCS-TCPmanojbanNo ratings yet
- Data Mentah Pasien CovidDocument280 pagesData Mentah Pasien CovidRizka Yuliana PutriNo ratings yet
- Diseases of ConjunctivaDocument28 pagesDiseases of ConjunctivaHawwi IsmailNo ratings yet
- URI Case (2 Lab Lecture) Patient Presentation: Chief ComplaintDocument2 pagesURI Case (2 Lab Lecture) Patient Presentation: Chief ComplaintMOHANNADNo ratings yet
- Methodological Instructions - Module 2Document60 pagesMethodological Instructions - Module 2Frt TrfNo ratings yet
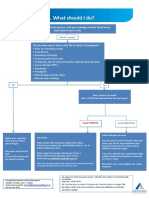
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Hepatitis CDocument15 pagesHepatitis CMohamed IsmailNo ratings yet
- HIV - Global HIV Neurology - A Comprehensive Review - 2018Document2 pagesHIV - Global HIV Neurology - A Comprehensive Review - 2018Juan Salazar PajaresNo ratings yet
- African Swine FeverDocument4 pagesAfrican Swine FeverShean FlorNo ratings yet
- Prak ParuDocument17 pagesPrak Paruhan jisungNo ratings yet
- Candida AurisDocument5 pagesCandida Aurisarunkumar76No ratings yet
- Formative Assessment On Ecologic ModelDocument3 pagesFormative Assessment On Ecologic ModelChezka Orton Swift BolintiamNo ratings yet
- Zika Virus: Emerging Arboviral Threat To BangladeshDocument17 pagesZika Virus: Emerging Arboviral Threat To BangladeshlkokodkodNo ratings yet
- WHOnet Preparation and Antibiogram InterpretationDocument2 pagesWHOnet Preparation and Antibiogram Interpretationarmada thamNo ratings yet
- Position Paper - El SalvadorDocument2 pagesPosition Paper - El SalvadorLily KazemiNo ratings yet
- Reading Guide V 6.0 EUCAST Disk Test 2019Document26 pagesReading Guide V 6.0 EUCAST Disk Test 2019oinkNo ratings yet
- Soal TPS Bahasa InggrisDocument3 pagesSoal TPS Bahasa InggrisMaya Putri EkasariNo ratings yet
- Assess and Classify The Sick Child Age 2 Months Up To 5 YearsDocument76 pagesAssess and Classify The Sick Child Age 2 Months Up To 5 YearsTaniaNo ratings yet
- SSI: Abx Treatment & ManagementDocument26 pagesSSI: Abx Treatment & ManagementSalsabila Al-BasheerNo ratings yet
- DR Dina - SARS-CoV-2 TransmissionDocument11 pagesDR Dina - SARS-CoV-2 TransmissionDina FaizahNo ratings yet
- UcellosisDocument4 pagesUcellosisyandraNo ratings yet
- Blood Flukes: Richelle D. Sales, RMTDocument20 pagesBlood Flukes: Richelle D. Sales, RMTZairah PascuaNo ratings yet