You might also like
- How To Make Your Own Voodoo DollsDocument4 pagesHow To Make Your Own Voodoo DollsJohn Willey100% (2)
- C15 Engine: Electrical Circuit DiagramDocument12 pagesC15 Engine: Electrical Circuit DiagramPhil B.100% (1)
- Tactical Combat Casualty Care November 2009Document262 pagesTactical Combat Casualty Care November 2009samatnadgob0036100% (1)
- 03C Tactical Field Care 100219Document262 pages03C Tactical Field Care 100219Jeremy McKinney100% (2)
- JRNL-Responding To Trauma Your Priorities in The First HourDocument8 pagesJRNL-Responding To Trauma Your Priorities in The First HourArs MoriendiNo ratings yet
- Cardiac Arrest and CPRDocument76 pagesCardiac Arrest and CPRDevi Yulianti100% (2)
- Redbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFDocument323 pagesRedbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFrizka100% (1)
- ATLS Case ScenarioDocument13 pagesATLS Case ScenarioJenny Schneider100% (2)
- Mathematics Stage 7 Sample Paper 1Document14 pagesMathematics Stage 7 Sample Paper 1Gideon Eka Dirgantara50% (2)
- Primary Care in Trauma PatientDocument109 pagesPrimary Care in Trauma PatientSumit AgarwalNo ratings yet
- PolytraumaDocument41 pagesPolytraumaFrederick Mars UntalanNo ratings yet
- Polytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaDocument57 pagesPolytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaAbuhafezbaka100% (1)
- BlastingDocument138 pagesBlastingcklconNo ratings yet
- 200+ TOP RADIOLOGY Online Quiz Questions - Exam Test 2023Document24 pages200+ TOP RADIOLOGY Online Quiz Questions - Exam Test 2023Ayub Alam100% (1)
- CP System For BulletsDocument37 pagesCP System For BulletsAnonymous TBAzJ8Ejd100% (1)
- Trauma OverviewDocument48 pagesTrauma OverviewFrancescoBarbero100% (1)
- Strategies For HarvestDocument86 pagesStrategies For HarvestBeka AsraNo ratings yet
- DV TUD Brochure 2015v2-SecuredDocument16 pagesDV TUD Brochure 2015v2-SecuredJR RZNo ratings yet
- The Space RaceDocument15 pagesThe Space RaceRadu Petrusan100% (1)
- Fabrication of 2 X 1000 MT Capacity Mounded LPG Storage VesselsDocument84 pagesFabrication of 2 X 1000 MT Capacity Mounded LPG Storage VesselsMilan DjumicNo ratings yet
- Basic Life SupportDocument46 pagesBasic Life SupportRuruni Kenchin Batusai50% (2)
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae TumNo ratings yet
- 1007 BLSDocument25 pages1007 BLSZainescu DanNo ratings yet
- Tactical Combat Casualty Care August 2011Document299 pagesTactical Combat Casualty Care August 2011Jared A. Lang100% (1)
- Module 07 - Airway Management in TFC: Speaker NotesDocument7 pagesModule 07 - Airway Management in TFC: Speaker NotesSae TumNo ratings yet
- Module 03 - Care Under Fire: Speaker NotesDocument12 pagesModule 03 - Care Under Fire: Speaker NotesSae TumNo ratings yet
- Module 08: Respiration Assessment and Management: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document24 pagesModule 08: Respiration Assessment and Management: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Luis-alfredo Perez Bolde HernandezNo ratings yet
- Module 01 - SpeakerDocument9 pagesModule 01 - SpeakerRoger RonconiNo ratings yet
- US Army Medical Course MD0569-200 - Chest and Airway ProblemsDocument55 pagesUS Army Medical Course MD0569-200 - Chest and Airway ProblemsGeorgesNo ratings yet
- Asm Course Speaker NotesDocument15 pagesAsm Course Speaker NotesJesse RobertNo ratings yet
- Module 02 - Medical Equipment: Speaker NotesDocument7 pagesModule 02 - Medical Equipment: Speaker NotesDERIL PRASETYONo ratings yet
- Module 02 - Medical Equipment: Speaker NotesDocument7 pagesModule 02 - Medical Equipment: Speaker NotesDERIL PRASETYONo ratings yet
- Emergency Anaesthetic Management To Extensive Thoracic Trauma-Hossam AtefDocument60 pagesEmergency Anaesthetic Management To Extensive Thoracic Trauma-Hossam AtefHossam atefNo ratings yet
- Airway Management in TFC: Skill InstructionsDocument8 pagesAirway Management in TFC: Skill InstructionsSae TumNo ratings yet
- TCCC Cls Didactics Mod 05 - 30 Jun 20Document31 pagesTCCC Cls Didactics Mod 05 - 30 Jun 20Giovanni RossiNo ratings yet
- Water Seal Drainage (WSD) : Entri-Entri BerikutnyaDocument7 pagesWater Seal Drainage (WSD) : Entri-Entri BerikutnyaputridwierlindaNo ratings yet
- Water Seal Drainage (WSD) : Entri-Entri BerikutnyaDocument12 pagesWater Seal Drainage (WSD) : Entri-Entri BerikutnyaputridwierlindaNo ratings yet
- Flail Chest ReportDocument4 pagesFlail Chest ReportMiggsNo ratings yet
- What Are The Ten New Commandments in Severe Polytrauma Management 1Document8 pagesWhat Are The Ten New Commandments in Severe Polytrauma Management 1antonio dengNo ratings yet
- 7 - Airway Management in TFCDocument18 pages7 - Airway Management in TFCCarlos MaravilhaNo ratings yet
- Trauma I - Abcs of Trauma Triage and TransportDocument16 pagesTrauma I - Abcs of Trauma Triage and TransportSamNo ratings yet
- Tactical Combat Casualty Care: SPC OwensDocument31 pagesTactical Combat Casualty Care: SPC OwenstashonowensNo ratings yet
- Lessonplan FinDocument14 pagesLessonplan Finx483xDNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- DR Anil Kumar Assistant Professor Department of Surgical Disciplines All India Institute of Medical SciencesDocument39 pagesDR Anil Kumar Assistant Professor Department of Surgical Disciplines All India Institute of Medical SciencesRiry AmbarsaryNo ratings yet
- Module 04 - Principles and Application of TFC: Speaker NotesDocument7 pagesModule 04 - Principles and Application of TFC: Speaker NotesSae Tum100% (1)
- Trauma and Blast InjuriesDocument22 pagesTrauma and Blast InjuriesHafiz Mahruzza100% (1)
- Chest Trauma: DR - Amr BastawaisiDocument10 pagesChest Trauma: DR - Amr BastawaisiBara FakhryNo ratings yet
- Chest TraumaDocument14 pagesChest TraumaMary Rose BatagaNo ratings yet
- Airway 1Document6 pagesAirway 1Ilyes FerenczNo ratings yet
- Tension PneumothoraxDocument19 pagesTension PneumothoraxRupita SitanggangNo ratings yet
- European Course Trauma CareDocument7 pagesEuropean Course Trauma CareYaclinNo ratings yet
- Management of Chest InjuriesDocument13 pagesManagement of Chest Injuriesana9filimonNo ratings yet
- Blunt Chest TraumaDocument10 pagesBlunt Chest TraumaFortune RubengoNo ratings yet
- Treatment of Thoracic Trauma Lessons From The BatDocument5 pagesTreatment of Thoracic Trauma Lessons From The Batchou youNo ratings yet
- Learning Material 1 Adult CPRDocument10 pagesLearning Material 1 Adult CPR3B ABAN, Daryl Lloyd G.No ratings yet
- Emergency Anaesthetic Management of Extensive Thoracic TraumaDocument7 pagesEmergency Anaesthetic Management of Extensive Thoracic TraumaYoz MpNo ratings yet
- Thoracic TraumaDocument13 pagesThoracic TraumaTony DawaNo ratings yet
- Final Chest Tube CareDocument46 pagesFinal Chest Tube Careوجد عمرNo ratings yet
- Chest Tubes, Pneumonectomy, Lobectomy, PleuralDocument40 pagesChest Tubes, Pneumonectomy, Lobectomy, PleuralMuhammad AliNo ratings yet
- Anesthesia For Thoracic Trauma - OpenAnesthesiaDocument7 pagesAnesthesia For Thoracic Trauma - OpenAnesthesiaReddyNo ratings yet
- ACLS Practice QuizDocument29 pagesACLS Practice Quizezzat salemNo ratings yet
- IntroductionDocument5 pagesIntroductionFarhan YulmiadiNo ratings yet
- ER JournalDocument7 pagesER JournalGab LandazabalNo ratings yet
- KGDDocument7 pagesKGDjihyunyeeNo ratings yet
- Final Chest Tube CareDocument46 pagesFinal Chest Tube Careوجد عمرNo ratings yet
- Go To:: Respiratory ImpairmentDocument18 pagesGo To:: Respiratory ImpairmentNanik LestariNo ratings yet
- 010303A TCCC-MP Tactical Field Care #1 IG 160603Document43 pages010303A TCCC-MP Tactical Field Care #1 IG 160603herralainNo ratings yet
- TraumaDocument12 pagesTraumagibreilNo ratings yet
- Complications of Percutaneous Coronary Intervention: The Survival HandbookFrom EverandComplications of Percutaneous Coronary Intervention: The Survival HandbookAlistair LindsayNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- One-Person Bag Valve Mask (BVM) : MarchDocument1 pageOne-Person Bag Valve Mask (BVM) : MarchSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Head-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedDocument1 pageHead-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationDocument2 pagesSkills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Atbf Ista PDFDocument12 pagesAtbf Ista PDFSae TumNo ratings yet
- One-Person Drag/Carry: Kit or Arm DragDocument5 pagesOne-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationDocument3 pagesSkills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationSae TumNo ratings yet
- Atbf PDFDocument1 pageAtbf PDFSae TumNo ratings yet
- Two-Person Drag/Carry: Kit or Arm DragDocument3 pagesTwo-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
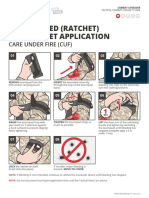
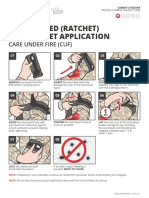
- One-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageOne-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 7: Airway ManagementDocument6 pagesSkills Assessment Checklist: MODULE 7: Airway ManagementSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareDocument1 pageSkills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDocument7 pagesSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- Two-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageTwo-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Analgesia Administration/ Antibiotic Admin: Skill InstructionsDocument3 pagesAnalgesia Administration/ Antibiotic Admin: Skill InstructionsSae TumNo ratings yet
- Evacuation Procedures: Skill InstructionsDocument3 pagesEvacuation Procedures: Skill InstructionsSae TumNo ratings yet
- Eye Injuries: Skill InstructionsDocument3 pagesEye Injuries: Skill InstructionsSae TumNo ratings yet
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae Tum0% (1)
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Module 11 - Hypothermia Prevention: Speaker NotesDocument6 pagesModule 11 - Hypothermia Prevention: Speaker NotesSae TumNo ratings yet
- Airway Management in TFC: Skill InstructionsDocument8 pagesAirway Management in TFC: Skill InstructionsSae TumNo ratings yet
- Module 13 - Eye Injuries: Speaker NotesDocument5 pagesModule 13 - Eye Injuries: Speaker NotesSae TumNo ratings yet
- Bridge Final ProposalDocument14 pagesBridge Final ProposalDr. A B M Amrul KaishNo ratings yet
- History Taking - Cheat SheetDocument2 pagesHistory Taking - Cheat SheetANGELICA CLAIRE BARECUATRONo ratings yet
- Special Project ReportDocument9 pagesSpecial Project ReportSangam PatariNo ratings yet
- Anatomy of A FireworkDocument4 pagesAnatomy of A FireworkMuthu KumarNo ratings yet
- Chapter - I (Electrical Safety)Document30 pagesChapter - I (Electrical Safety)Hunter HarshaNo ratings yet
- Philips HTS3510 PDFDocument66 pagesPhilips HTS3510 PDFJesusNo ratings yet
- Costing of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMDocument3 pagesCosting of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMMohtashim KazmiNo ratings yet
- HVAC Validation 1649296351Document15 pagesHVAC Validation 1649296351jeyapragash RamadassNo ratings yet
- Bradley Sink Verge LVLD2Document4 pagesBradley Sink Verge LVLD2isaacgamezNo ratings yet
- The IMA Volumes in Mathematics and Its Applications: Avner Friedman Willard Miller, JRDocument172 pagesThe IMA Volumes in Mathematics and Its Applications: Avner Friedman Willard Miller, JRPedro PereyraNo ratings yet
- Investigation of Liquid-Liquid Phase Equilibria For Reactive Extraction of Lactic Acid With Organophosphorus SolventsDocument6 pagesInvestigation of Liquid-Liquid Phase Equilibria For Reactive Extraction of Lactic Acid With Organophosphorus Solventskudsiya firdousNo ratings yet
- Served POsDocument21 pagesServed POsYay DumaliNo ratings yet
- Electronic Prepayment Meter6Document4 pagesElectronic Prepayment Meter6Sumitha SudevanNo ratings yet
- Sithkop005 AnswersDocument46 pagesSithkop005 AnswersSid SharmaNo ratings yet
- English 12 Unit 1Document7 pagesEnglish 12 Unit 1Anonymous N6ccr9MVNo ratings yet
- Who Can Learn Diploma CivilDocument19 pagesWho Can Learn Diploma CivilGururaj TavildarNo ratings yet
- Study On Solar Irrigation System in BangladeshDocument61 pagesStudy On Solar Irrigation System in Bangladeshavocadocolor100% (2)
- ME-222-01 (Simple Mechanism)Document32 pagesME-222-01 (Simple Mechanism)Imran TahirNo ratings yet
- Para Jumbles Test-1Document4 pagesPara Jumbles Test-1vennelaNo ratings yet
- Ursina CollisionDocument3 pagesUrsina CollisionGilniro JúniorNo ratings yet