You might also like
- Trees Guidelines For Residents and Arborists Accessible PDF FA3Document10 pagesTrees Guidelines For Residents and Arborists Accessible PDF FA3CaptainBrinebloodNo ratings yet
- Dual Energy CT - Basis and ApplicationsDocument7 pagesDual Energy CT - Basis and Applicationsjturos2003100% (1)
- Critical AppraisalDocument49 pagesCritical AppraisalJyoti GavaliNo ratings yet
- Special SensesDocument56 pagesSpecial SensesKhrystine VenturaNo ratings yet
- Final - Technical - Specifications FAADocument242 pagesFinal - Technical - Specifications FAAkmiqdNo ratings yet
- Nuclear CardiologyDocument34 pagesNuclear CardiologyAmit JoshiNo ratings yet
- Braunwald's Heart Disease 12th - Nuclear CardiologyDocument46 pagesBraunwald's Heart Disease 12th - Nuclear CardiologyNyoman Ririn Chandrika Sari100% (1)
- 3.0 - Occupational Noise v3.1 EnglishDocument22 pages3.0 - Occupational Noise v3.1 Englishkhalid_ghafoor6226No ratings yet
- D 7167 Monitoring Performance of Safety Related Linings PDFDocument7 pagesD 7167 Monitoring Performance of Safety Related Linings PDFImmanuel100% (1)
- # Medison System Passwords: Debug Mode Windows (DOS) Admin Mode Booting Password Product Setup ModeDocument1 page# Medison System Passwords: Debug Mode Windows (DOS) Admin Mode Booting Password Product Setup ModeAwadh100% (3)
- Chesneys Equipment For Student Radiographers by P H Carter PDFDocument5 pagesChesneys Equipment For Student Radiographers by P H Carter PDFAwadhNo ratings yet
- Updates in Vascular Computed TomographyDocument21 pagesUpdates in Vascular Computed TomographyHector Hernandez-SoriaNo ratings yet
- Idose Low KVDocument18 pagesIdose Low KVMurilo AssunçãoNo ratings yet
- Ultra Low Dose Comparative VendorDocument9 pagesUltra Low Dose Comparative Vendoryuda ibnuNo ratings yet
- Perisinakis2018 Article TheEffectOfIodineUptakeOnRadiaDocument8 pagesPerisinakis2018 Article TheEffectOfIodineUptakeOnRadiaJose Mateo Baron RestrepoNo ratings yet
- Diffusion MRIDocument7 pagesDiffusion MRIMoh Hidayat ThahaNo ratings yet
- Dose Reduction in Two Systems New and OldDocument8 pagesDose Reduction in Two Systems New and OldKomalNo ratings yet
- Strategies For Radiation Dose OptimizationDocument10 pagesStrategies For Radiation Dose OptimizationthutaNo ratings yet
- Physics and Imaging in Radiation OncologyDocument6 pagesPhysics and Imaging in Radiation Oncologydarr artNo ratings yet
- European Journal of Radiology: Yuan-Mao Lin, Yi-You Chiou, Mei-Han Wu, Shan-Su Huang, Shu-Huei ShenDocument8 pagesEuropean Journal of Radiology: Yuan-Mao Lin, Yi-You Chiou, Mei-Han Wu, Shan-Su Huang, Shu-Huei ShenKyerohtaronNo ratings yet
- Medical Physics - 2018 - Ommen - Image Quality of Conventional Images of Dual Layer SPECTRAL CT A Phantom StudyDocument13 pagesMedical Physics - 2018 - Ommen - Image Quality of Conventional Images of Dual Layer SPECTRAL CT A Phantom StudyAmril MukminNo ratings yet
- Computed Tomography: Physics Considerations For Quality and DoseDocument75 pagesComputed Tomography: Physics Considerations For Quality and DosedanaNo ratings yet
- Wells2020 Article DoseReductionIsGoodButItIsImagDocument3 pagesWells2020 Article DoseReductionIsGoodButItIsImageltonNo ratings yet
- 10.1007@s00259 020 04746 6Document13 pages10.1007@s00259 020 04746 6Johnny LópezNo ratings yet
- 82Rb PET-CT - Entering A New Area of Myocardial Perfusion ImagingDocument2 pages82Rb PET-CT - Entering A New Area of Myocardial Perfusion ImagingPatyMNNo ratings yet
- CT - Genap 2Document10 pagesCT - Genap 2Kesitaa GraceeNo ratings yet
- Jkps 60 1150Document7 pagesJkps 60 1150Leona PradistyNo ratings yet
- CT Dose IssuesDocument28 pagesCT Dose IssuessanyengereNo ratings yet
- BF 01887304Document4 pagesBF 01887304zuhdi azzyumar dhiniNo ratings yet
- NIH Public Access: Author ManuscriptDocument25 pagesNIH Public Access: Author ManuscriptLaurentiu RadoiNo ratings yet
- Ijri 29 53Document8 pagesIjri 29 53Kelum BuddhikaNo ratings yet
- CT SacnDocument6 pagesCT SacnmartinNo ratings yet
- Feasibility and Safety of Non Contrast Optical Coherence Tomography Imaging Using Hydroxyethyl Starch in Coronary ArteriesDocument12 pagesFeasibility and Safety of Non Contrast Optical Coherence Tomography Imaging Using Hydroxyethyl Starch in Coronary ArteriesLukman SulistiyadiNo ratings yet
- Deriving The Effective Atomic Number With A Dual-Energy Image Set Acquired by The Big Bore CT SimulatorDocument12 pagesDeriving The Effective Atomic Number With A Dual-Energy Image Set Acquired by The Big Bore CT SimulatorFadli SaputroNo ratings yet
- CT GanjilDocument6 pagesCT Ganjilmuhammad erfansyahNo ratings yet
- X-Ray Pulsing Methods For Reduced-Dose Computed Tomography in PET/CT Attenuation CorrectionDocument15 pagesX-Ray Pulsing Methods For Reduced-Dose Computed Tomography in PET/CT Attenuation CorrectionsunlianzhuNo ratings yet
- Reciprocal Communication of Pericoronary Adipose TDocument7 pagesReciprocal Communication of Pericoronary Adipose TeugeniaNo ratings yet
- Pediatric Cardiac-Gated CT Angiography: Assessment of Radiation DoseDocument7 pagesPediatric Cardiac-Gated CT Angiography: Assessment of Radiation DoseDimas PramujaNo ratings yet
- TM 10. CT CARDIAC Artikel 2 PCD-CTDocument13 pagesTM 10. CT CARDIAC Artikel 2 PCD-CTrellvandraaaNo ratings yet
- Kim 2010Document13 pagesKim 2010face bookNo ratings yet
- Quantification of Cross Vendor Variation in ADC MeDocument6 pagesQuantification of Cross Vendor Variation in ADC MedeaNo ratings yet
- Image Texture, Low Contrast Liver Lesion DetectabiDocument9 pagesImage Texture, Low Contrast Liver Lesion DetectabieugeniaNo ratings yet
- A Study of Urinary Tract Abnormalities: Role of Low Dose MDCT UrographyDocument9 pagesA Study of Urinary Tract Abnormalities: Role of Low Dose MDCT UrographyIJAR JOURNALNo ratings yet
- Powerful Employment Techniques in The Physical Exercise Trial For People Using FibromyalgiaxwgalDocument1 pagePowerful Employment Techniques in The Physical Exercise Trial For People Using Fibromyalgiaxwgalcopperborder14No ratings yet
- Heart Rate Detection From Plantar Bioimpedance Measurements: R. González Landaeta, O. Casas, R. Pallàs-ArenyDocument4 pagesHeart Rate Detection From Plantar Bioimpedance Measurements: R. González Landaeta, O. Casas, R. Pallàs-ArenyLowayNo ratings yet
- Intravascular Low-Power Laser Illumination Through Special Fiber DiffusersDocument3 pagesIntravascular Low-Power Laser Illumination Through Special Fiber DiffusersNoura RoseNo ratings yet
- Spectral Detector For Cardiovascular Applications Rajiah2017Document7 pagesSpectral Detector For Cardiovascular Applications Rajiah2017July ArgoNo ratings yet
- Cancer Center: Tomotherapy'S Implementation of Image-Guided Adaptive Radiation TherapyDocument94 pagesCancer Center: Tomotherapy'S Implementation of Image-Guided Adaptive Radiation TherapyMalu Paras LacsonNo ratings yet
- Mahuvava C Et Al. (2022)Document13 pagesMahuvava C Et Al. (2022)Courage MahuvavaNo ratings yet
- Dose-Reduction Experiment During A Cervical Vertebrae ExaminationDocument12 pagesDose-Reduction Experiment During A Cervical Vertebrae ExaminationDesty ArianiNo ratings yet
- Qims 12 01 766Document15 pagesQims 12 01 766Hamza ArjahNo ratings yet
- Proceedings of Spie: A Deep Learning Approach For Dual-Energy CT Imaging Using A Single - Energy CT DataDocument6 pagesProceedings of Spie: A Deep Learning Approach For Dual-Energy CT Imaging Using A Single - Energy CT Datazhaohui zhiNo ratings yet
- Dual-Source CT and The Effect of Tin Filtration On ImageDocument6 pagesDual-Source CT and The Effect of Tin Filtration On Imagemas bejo01No ratings yet
- TAC PeñascoDocument10 pagesTAC PeñascoJose ManuelNo ratings yet
- Dual Energy CTDocument11 pagesDual Energy CTdeadcorpsesNo ratings yet
- ArticleDocument7 pagesArticleHenry MruizNo ratings yet
- Ryct 2021200378Document14 pagesRyct 2021200378Vimal NishadNo ratings yet
- Comparison Between View Summing and Tube Pulsing in Ultra Low Dose CT Acquisitions For PET Attenuation CorrectionDocument15 pagesComparison Between View Summing and Tube Pulsing in Ultra Low Dose CT Acquisitions For PET Attenuation CorrectionHernan PerezNo ratings yet
- Dual-Energy Spectral Computed Tomography To Thoracic Oncology Imaging KJRDocument13 pagesDual-Energy Spectral Computed Tomography To Thoracic Oncology Imaging KJRMANGNo ratings yet
- Evaluation of RT Imaging DevicesDocument7 pagesEvaluation of RT Imaging DevicesKurt Van DelinderNo ratings yet
- Principles of CT and CT Technology : P CT CTT - Goldman 115Document14 pagesPrinciples of CT and CT Technology : P CT CTT - Goldman 115Madalina ConstantinNo ratings yet
- Scoliosis ManagementDocument5 pagesScoliosis ManagementYandriyaneStephanieNo ratings yet
- RevCT Low-Dose JB28027XEDocument5 pagesRevCT Low-Dose JB28027XEAvaneesh SinghNo ratings yet
- Photon Counting Spectral CT Versus Conventional CT: Comparative Evaluation For Breast Imaging ApplicationDocument27 pagesPhoton Counting Spectral CT Versus Conventional CT: Comparative Evaluation For Breast Imaging Applicationcarlos56dbNo ratings yet
- CT Radiation Dose Optimization and Estimation An U PDFDocument11 pagesCT Radiation Dose Optimization and Estimation An U PDFAli HadiNo ratings yet
- 1 s2.0 S0167814022001529 MainDocument6 pages1 s2.0 S0167814022001529 MainnimaelhajjiNo ratings yet
- Duplex and Color Doppler Imaging of the Venous SystemFrom EverandDuplex and Color Doppler Imaging of the Venous SystemGerhard H. MostbeckNo ratings yet
- No Rotation No Integration: Simple FunctionDocument2 pagesNo Rotation No Integration: Simple FunctionAwadhNo ratings yet
- 74 300ma X Ray MachineDocument2 pages74 300ma X Ray MachineAwadhNo ratings yet
- Chemistry OGS ETHOS OGSDocument10 pagesChemistry OGS ETHOS OGSAwadhNo ratings yet
- Resolving Our Uncertainty About Oxygen TherapyDocument7 pagesResolving Our Uncertainty About Oxygen TherapyAwadhNo ratings yet
- What Is EOS X-Ray Imaging?Document2 pagesWhat Is EOS X-Ray Imaging?AwadhNo ratings yet
- Oxygen Concentrators For District Hospitals: Michael B Dobson, John Radcliffe Hospital, Oxford, UKDocument3 pagesOxygen Concentrators For District Hospitals: Michael B Dobson, John Radcliffe Hospital, Oxford, UKAwadhNo ratings yet
- The Epic Arm: Nia Christian, Lindsey Milisits, Jeffrey Nemes, and Dustin SchneiderDocument1 pageThe Epic Arm: Nia Christian, Lindsey Milisits, Jeffrey Nemes, and Dustin SchneiderAwadhNo ratings yet
- The Oxygen Concentrator: DR Roger Eltringham, Consultant Anaesthetist, Gloucestershire Royal Hospital, GloucesterDocument2 pagesThe Oxygen Concentrator: DR Roger Eltringham, Consultant Anaesthetist, Gloucestershire Royal Hospital, GloucesterAwadhNo ratings yet
- CS 3D Scanner Family: CS 3500 & CS 3600: Device Not Recognized After Cumulative Updates On Windows 10Document3 pagesCS 3D Scanner Family: CS 3500 & CS 3600: Device Not Recognized After Cumulative Updates On Windows 10AwadhNo ratings yet
- Resource Manual For Compliance Test Parameters of Diagnostic X Ray Systems (PDF Version) PDFDocument45 pagesResource Manual For Compliance Test Parameters of Diagnostic X Ray Systems (PDF Version) PDFAwadhNo ratings yet
- Hitachi AIRIS II Open Tech SpecsDocument2 pagesHitachi AIRIS II Open Tech SpecsAwadhNo ratings yet
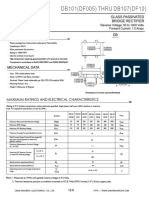
- DB101 (DF005) THRU DB107 (DF10) : Glass Passivated Bridge RectifierDocument2 pagesDB101 (DF005) THRU DB107 (DF10) : Glass Passivated Bridge RectifierAwadhNo ratings yet
- Migration Health Information Sheet Usa Kenya CleanDocument4 pagesMigration Health Information Sheet Usa Kenya Cleanelphas minyatoNo ratings yet
- Chap 6.2 QuestionsDocument4 pagesChap 6.2 QuestionsAnnie NguyenNo ratings yet
- (Reliable Diagnostic Laboratory Nepal Pvt. LTD.) Samakhushi-26, Kathmandu, Nepal, Phone: 014366073 9801612348Document1 page(Reliable Diagnostic Laboratory Nepal Pvt. LTD.) Samakhushi-26, Kathmandu, Nepal, Phone: 014366073 9801612348Abinash MandalNo ratings yet
- Scoring Tables EDSSDocument1 pageScoring Tables EDSSHugo Zúñiga UtorNo ratings yet
- Molecular Biology : Test For COVID-19 RT PCRDocument1 pageMolecular Biology : Test For COVID-19 RT PCRmikekikNo ratings yet
- Forensic Chemistry: Course GuideDocument20 pagesForensic Chemistry: Course GuideEmelie TipayNo ratings yet
- M040GB014A00A-DOC00 - Smart ScreeningDocument11 pagesM040GB014A00A-DOC00 - Smart Screeningrocol.aplicaciones2No ratings yet
- AHIMSWeb 1Document1 pageAHIMSWeb 1rose thomsan thomsan60% (5)
- Normal Control 1 - 0020013900: ENGLISH - Insert Revision 04/2018Document3 pagesNormal Control 1 - 0020013900: ENGLISH - Insert Revision 04/2018Brady AndersonNo ratings yet
- UIBC Liquid: REF Determination of UIBC (Unsaturated Iron-Binding Capacity) (UIBC) in Serum and Plasma IVDDocument2 pagesUIBC Liquid: REF Determination of UIBC (Unsaturated Iron-Binding Capacity) (UIBC) in Serum and Plasma IVDzaraNo ratings yet
- Transport Validation Sample Protocol - Pharmaceutical GuidelinesDocument2 pagesTransport Validation Sample Protocol - Pharmaceutical GuidelinesIrvinn NhutsNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptKondang WarasNo ratings yet
- NEET 2021 Question Paper Tamil O6 PDFDocument32 pagesNEET 2021 Question Paper Tamil O6 PDFmuthurajmsmNo ratings yet
- EURACHEM/CITAC AQA 2021: Assessment of Performance and Uncertainty in Qualitative Tests in The Medical LaboratoryDocument15 pagesEURACHEM/CITAC AQA 2021: Assessment of Performance and Uncertainty in Qualitative Tests in The Medical LaboratoryPaulo PereiraNo ratings yet
- Methods of Collecting DataDocument65 pagesMethods of Collecting DataJhamille CardonaNo ratings yet
- Effectiveness of Mindfulness-Based Colouring For Test Anxiety in AdolescentsDocument22 pagesEffectiveness of Mindfulness-Based Colouring For Test Anxiety in AdolescentsBachtiar Agung LaksonoNo ratings yet
- Kumbahar 2018Document105 pagesKumbahar 2018zdenkaNo ratings yet
- Date Doctor's Order Nursing Responsibilities Patient Reaction/ EvaluationDocument3 pagesDate Doctor's Order Nursing Responsibilities Patient Reaction/ EvaluationLouwella RamosNo ratings yet
- Physiotherapy-Led Functional Exercise Programme After THR 2016Document7 pagesPhysiotherapy-Led Functional Exercise Programme After THR 2016Eshel TachnaiNo ratings yet
- Principles of Haccp: Principle 1 - Conduct A Hazard AnalysisDocument6 pagesPrinciples of Haccp: Principle 1 - Conduct A Hazard AnalysisAttia MunawerNo ratings yet
- Dimensions of Learning Organizations Questionnaire (DLOQ) in A Low-Resource Health Care Setting in NepalDocument8 pagesDimensions of Learning Organizations Questionnaire (DLOQ) in A Low-Resource Health Care Setting in Nepalsapit90No ratings yet
- CLO and GatroDocument2 pagesCLO and Gatropamela_tiffani9221No ratings yet
- Cohen Based SummaryDocument29 pagesCohen Based SummaryMartha Lou Cris PaleroNo ratings yet
- Blood and TSH ReportDocument3 pagesBlood and TSH Reportindrajit sinhaNo ratings yet