You might also like
- Internal MedicineDocument1,591 pagesInternal MedicineRina_Fatimah_Nuriila96% (46)
- Cervical Cancer: Dr. Sushma DhakalDocument137 pagesCervical Cancer: Dr. Sushma DhakalBhattarai ShrinkhalaNo ratings yet
- Respiratory PathophysDocument1 pageRespiratory PathophysTori IkeharaNo ratings yet
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocument4 pagesPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaAzria John DemetriNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJesselle LasernaNo ratings yet
- A Concept Map On External OtitisDocument9 pagesA Concept Map On External OtitisJoe RealNo ratings yet
- Communicable DiseaseDocument5 pagesCommunicable DiseaseVinceNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaMaria Cristina100% (1)
- Copd PathoDocument2 pagesCopd PathoAlvin RamirezNo ratings yet
- Dorothea Orem PowerpointDocument35 pagesDorothea Orem Powerpointapi-486954490No ratings yet
- Book Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsDocument7 pagesBook Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsIrish EspinosaNo ratings yet
- B. Diagram: Predisposing Factors: Precipitating Factors EtiologyDocument3 pagesB. Diagram: Predisposing Factors: Precipitating Factors EtiologyKenneth Torres100% (1)
- ErythromycinDocument1 pageErythromycinKenneth Robert Abrantes0% (1)
- Staffing ComputationsDocument24 pagesStaffing ComputationsOliric Acnab Nabcih100% (4)
- LEaflet TBCDocument3 pagesLEaflet TBCatik mayasariNo ratings yet
- CSS TuberkulosisDocument69 pagesCSS TuberkulosisdhaniNo ratings yet
- Predisposing Factors: Precipitating Factors: Contributing FactorsDocument6 pagesPredisposing Factors: Precipitating Factors: Contributing FactorsKen SimonNo ratings yet
- Pathophysiology of Typhoid FeverDocument4 pagesPathophysiology of Typhoid FeverIan ParrochaNo ratings yet
- Pa Tho Physiology of Typhoid Fever Client BasedrtyytyttyDocument3 pagesPa Tho Physiology of Typhoid Fever Client Basedrtyytyttyangeliejoy_1109No ratings yet
- Patient Based PathophysiologyDocument2 pagesPatient Based PathophysiologyDeinielle Magdangal RomeroNo ratings yet
- 1.4 Pathway: MK Kurang PengetahuanDocument2 pages1.4 Pathway: MK Kurang PengetahuanMeiaroh PitrianiNo ratings yet
- Appendicitis PathophysiologyDocument1 pageAppendicitis PathophysiologyPatricia Beatrice Dela CenaNo ratings yet
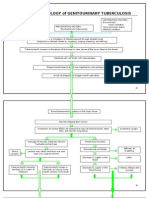
- Pathophysiology of Genitourinary TuberculosisDocument8 pagesPathophysiology of Genitourinary Tuberculosisace_51891No ratings yet
- Pasco Antibiotics PDFDocument7 pagesPasco Antibiotics PDFNicole ObispoNo ratings yet
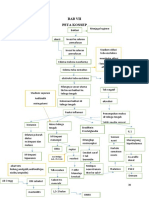
- Bab Vii Peta Konsep: Cuci Telinga H O 3% 3-5hrDocument1 pageBab Vii Peta Konsep: Cuci Telinga H O 3% 3-5hrika nurnailaNo ratings yet
- San Gabriel, GMA, Cavite College of Nursing: Iv. Pathophysiology by The BookDocument2 pagesSan Gabriel, GMA, Cavite College of Nursing: Iv. Pathophysiology by The BookSTEPHANIE LIBO-ONNo ratings yet
- Chart - Respiratory Infections BacteriaDocument4 pagesChart - Respiratory Infections BacteriaRedNo ratings yet
- Predisposing Factors Disease Precipitating Factors: LegendDocument3 pagesPredisposing Factors Disease Precipitating Factors: LegendSOPHIA LOISE TEJANO FULACHENo ratings yet
- NCM 112 Respiratory HandoutDocument7 pagesNCM 112 Respiratory HandoutissaiahnicolleNo ratings yet
- Non-Modifiable Factors Modifiable Factors: (Causative Agent: Respiratory Syncytia Virus)Document3 pagesNon-Modifiable Factors Modifiable Factors: (Causative Agent: Respiratory Syncytia Virus)Venice Joy CelociaNo ratings yet
- Scarlet Fever (Scarlatina) : Bacterial Infection Etiology Oral Manifestations Prevention and ControlDocument16 pagesScarlet Fever (Scarlatina) : Bacterial Infection Etiology Oral Manifestations Prevention and ControlFatima CarlosNo ratings yet
- Final PathophysiologyDocument3 pagesFinal Pathophysiologyemely p. tangoNo ratings yet
- Dr. Mochamad Aleq Sander, M.Kes., SP.B., FINACS: Sertifikasi Dosen: 12107102411578Document31 pagesDr. Mochamad Aleq Sander, M.Kes., SP.B., FINACS: Sertifikasi Dosen: 12107102411578Alif riadiNo ratings yet
- Droplet Infection: Tuberkulosis (TB) ParuDocument2 pagesDroplet Infection: Tuberkulosis (TB) ParuMiiniieNo ratings yet
- StreptococcusDocument2 pagesStreptococcusapi-335483695No ratings yet
- MASTOIDITISDocument1 pageMASTOIDITISJamie MartinezNo ratings yet
- Group 3 BSN3D CapDocument6 pagesGroup 3 BSN3D CapJingky AnquillanoNo ratings yet
- Emed - Pedia 1Document7 pagesEmed - Pedia 1Princess Cate MercadoNo ratings yet
- Person With Silicosis, DM, Post Gastrectomy StateDocument6 pagesPerson With Silicosis, DM, Post Gastrectomy StatekhleeoNo ratings yet
- Non-Modifiable Factors Modifiable Factors: Cellular Destruction of Infected Cells Attracts Nearby Immune Cells (NK Cells)Document2 pagesNon-Modifiable Factors Modifiable Factors: Cellular Destruction of Infected Cells Attracts Nearby Immune Cells (NK Cells)Venice Joy CelociaNo ratings yet
- PATHOPHYSIOLOGY ShortDocument4 pagesPATHOPHYSIOLOGY ShortBSN 2 - Sasis, Rusmaryte C.No ratings yet
- Patient Based PathophysiologyDocument3 pagesPatient Based PathophysiologyJeizel IgnacioNo ratings yet
- Pneumonia Pathophysiology (Book Based) : Non-Modifiable: ModifiableDocument2 pagesPneumonia Pathophysiology (Book Based) : Non-Modifiable: ModifiableYVETTE CLAIRE BORRESNo ratings yet
- Antibiotics PrototypesDocument4 pagesAntibiotics PrototypesbenbengNo ratings yet
- Patho Client DraftDocument2 pagesPatho Client DraftBeverly DatuNo ratings yet
- Medically Important Bacteria Memorisation SheetDocument7 pagesMedically Important Bacteria Memorisation SheetOlivia LimNo ratings yet
- Asthma Pathophysiology: Ixsy Ramirez, MD, MPH Pediatric Pulmonology University of Michigan, C.S. Mott Children's HospitalDocument21 pagesAsthma Pathophysiology: Ixsy Ramirez, MD, MPH Pediatric Pulmonology University of Michigan, C.S. Mott Children's HospitalAru VermaNo ratings yet
- Illustrator File Edit Select Effect View Window HelpDocument8 pagesIllustrator File Edit Select Effect View Window HelpHaizel BieberNo ratings yet
- Sweat Chloride Test: 1. Splenic Rupture 2. Avoid Sports and Physical Activity 3. Atypical LymphocytesDocument7 pagesSweat Chloride Test: 1. Splenic Rupture 2. Avoid Sports and Physical Activity 3. Atypical LymphocytesAnonymous GfqHQ5SNwNo ratings yet
- Chronic Rhinosinusitis and Nasal PolyposisDocument79 pagesChronic Rhinosinusitis and Nasal PolyposisSinewraz PmNo ratings yet
- Pathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionDocument4 pagesPathophysiology of Koch's Disease (Tuberculosis) : Primary InfectionbijelNo ratings yet
- تَـلـخـيـص شَـابـتـر ٢٣?Document10 pagesتَـلـخـيـص شَـابـتـر ٢٣?سلطان محمد فوزي سلمانNo ratings yet
- Patho For Appendicitis With Gen PeritonitisDocument2 pagesPatho For Appendicitis With Gen PeritonitisSydelle GravadorNo ratings yet
- TuberkulosisanakDocument106 pagesTuberkulosisanakUdin NicotinicNo ratings yet
- 4.1 PEDIA-Pneumonia, Tuberculosis, Interstitial Lung Diseases (Dr. Bermejo)Document6 pages4.1 PEDIA-Pneumonia, Tuberculosis, Interstitial Lung Diseases (Dr. Bermejo)Monique BorresNo ratings yet
- ASTHMA CPD FINAL (Autosaved)Document74 pagesASTHMA CPD FINAL (Autosaved)Affri Dian AdiyatnaNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- Streptococcus Pyogens Handout G2Document3 pagesStreptococcus Pyogens Handout G2Raiden EiNo ratings yet
- Infectious DiseasesDocument3 pagesInfectious Diseasesshreyavjha2020No ratings yet
- Immediate Hypersensitivity (Type 1)Document7 pagesImmediate Hypersensitivity (Type 1)Mei LingNo ratings yet
- Diseases Microbiology and ParasitologyDocument3 pagesDiseases Microbiology and Parasitologyarsdef tuanNo ratings yet
- UTI PathophysiologyDocument1 pageUTI PathophysiologyNathaniel SupanNo ratings yet
- Rheumatic Heart DiseaseDocument15 pagesRheumatic Heart DiseaseAica AnisNo ratings yet
- 3.5 Nursing Implementation Name: An.A Age: 1,5 Year Dx. Medis: ARI and OMADocument4 pages3.5 Nursing Implementation Name: An.A Age: 1,5 Year Dx. Medis: ARI and OMARizki ArifNo ratings yet
- Implementasi Bhs Inggris FixDocument5 pagesImplementasi Bhs Inggris FixRizki ArifNo ratings yet
- Intervensi Ispa Dan Oma FixDocument5 pagesIntervensi Ispa Dan Oma FixRizki ArifNo ratings yet
- definisiISPA and OtitisDocument22 pagesdefinisiISPA and OtitisRizki ArifNo ratings yet
- Reading Comprehension 4-DikonversiDocument2 pagesReading Comprehension 4-DikonversiJenifer DoloksaribuNo ratings yet
- Planned Parenthood and Students Knowledge of Contraceptive MethodsDocument10 pagesPlanned Parenthood and Students Knowledge of Contraceptive MethodssncuNo ratings yet
- Community Needs Assessment Form 1. Name of Community/ Institution Being Assessed Mae Kalingang Montalbano 2. Venue or Description of The LocationDocument6 pagesCommunity Needs Assessment Form 1. Name of Community/ Institution Being Assessed Mae Kalingang Montalbano 2. Venue or Description of The Locationriri badgalNo ratings yet
- Laporan Kegiatan Dan Reimbursement Biaya Pengurusan Visa AustraliaDocument5 pagesLaporan Kegiatan Dan Reimbursement Biaya Pengurusan Visa AustraliamemekbecekNo ratings yet
- A QUASI SynopsisDocument9 pagesA QUASI Synopsischaranjit kaurNo ratings yet
- Medical Imaging WebquestDocument8 pagesMedical Imaging Webquestapi-262193618No ratings yet
- Multiple Chemical Sensitivities - Addendum To Biologic Markers in ImmunotoxicologyDocument207 pagesMultiple Chemical Sensitivities - Addendum To Biologic Markers in ImmunotoxicologyCarlos RodriguezNo ratings yet
- Essay 3 Final DraftDocument6 pagesEssay 3 Final Draftapi-360460383No ratings yet
- Daftar Harga VaksinDocument1 pageDaftar Harga VaksinIF RS Surya AsihNo ratings yet
- Part 1 - Curriculum VitaeDocument33 pagesPart 1 - Curriculum VitaeAmriatiNo ratings yet
- Antibiotic Resistance Among Uropathogenic Escherichia ColiDocument13 pagesAntibiotic Resistance Among Uropathogenic Escherichia ColiSyed AmanNo ratings yet
- Feeding Tube Insertion (Gastrostomy)Document5 pagesFeeding Tube Insertion (Gastrostomy)maredithsaludarNo ratings yet
- Slowther and Kleinman - ConfidentialityDocument4 pagesSlowther and Kleinman - ConfidentialitysugarmelodiesNo ratings yet
- Triple Antibiotic PasteDocument5 pagesTriple Antibiotic PasteVinisha Vipin SharmaNo ratings yet
- The Prevention and Management of Pressure UlcerDocument5 pagesThe Prevention and Management of Pressure UlcerrantiNo ratings yet
- Hrvoje Puskaric Danijela Tadic Marija Zahar DjordjevicDocument10 pagesHrvoje Puskaric Danijela Tadic Marija Zahar DjordjevicHom Jyoti AdhikariNo ratings yet
- Day2.2 - Lionberger - GDUFA Regulatory ScienceDocument37 pagesDay2.2 - Lionberger - GDUFA Regulatory ScienceMarkbot1999No ratings yet
- Different Types of TriageDocument28 pagesDifferent Types of Triageanda3003No ratings yet
- NEWBORN CAREPLAN - VEST - FISTULA SurgicalDocument16 pagesNEWBORN CAREPLAN - VEST - FISTULA SurgicalArchana SahuNo ratings yet
- Lesson 2 - Principles of Nutrition TherapyDocument15 pagesLesson 2 - Principles of Nutrition TherapyJoddie LoplopNo ratings yet
- The Cost Conundrum in HealthcareDocument8 pagesThe Cost Conundrum in HealthcarePaul SchumannNo ratings yet
- Multiple pregNANCYDocument83 pagesMultiple pregNANCYDoc RaymondNo ratings yet
- Cardiology BrochureDocument2 pagesCardiology Brochureong251183No ratings yet
- Gonorrhea Case StudyDocument2 pagesGonorrhea Case StudyDonna LLerandi100% (1)
- Post Hand Spa ActivityDocument16 pagesPost Hand Spa Activityma cleah ramos0% (1)