You might also like
- Radiographic Pathology For Technologists 6th Edition Kowalczyk Test BankDocument6 pagesRadiographic Pathology For Technologists 6th Edition Kowalczyk Test Bankbeatrixkhuyen9rm100% (29)
- Anatomy and Physiology CH 1 To 3 Flash CardsDocument14 pagesAnatomy and Physiology CH 1 To 3 Flash Cardsmalenya1100% (1)
- MCQ Oral Histology (Textbook)Document33 pagesMCQ Oral Histology (Textbook)Magnet Shot100% (5)
- Anatomical Landmarks of Maxillary and Mandibular CastDocument73 pagesAnatomical Landmarks of Maxillary and Mandibular Castvarsha ammu80% (5)
- Anatomy & Physiology CH 17 Marieb & Hoehn LectureDocument148 pagesAnatomy & Physiology CH 17 Marieb & Hoehn LectureCocoa Doogle100% (2)
- Bone and Bone Graft HealingDocument12 pagesBone and Bone Graft HealingJayanth PerumalNo ratings yet
- AN OVERVIEW OF BONE CELLS AND THEIR REGULATING FACTORS OF DIFFERENTIATION, Mohamed 2008Document9 pagesAN OVERVIEW OF BONE CELLS AND THEIR REGULATING FACTORS OF DIFFERENTIATION, Mohamed 2008Faizal Reza PahleviNo ratings yet
- Biomechanics and Biomaterials in Orthopedic SurgeryDocument11 pagesBiomechanics and Biomaterials in Orthopedic SurgeryManiventhan NachimuthuNo ratings yet
- Principles of Bone GraftingDocument6 pagesPrinciples of Bone GraftingJayanth Perumal100% (2)
- Maxillary Sinus Bone GraftingDocument181 pagesMaxillary Sinus Bone GraftingTuấn Hành TrầnNo ratings yet
- Chemistry Project On Estimation of Contant of Bone Ash PDFDocument9 pagesChemistry Project On Estimation of Contant of Bone Ash PDFPooja BhagwatNo ratings yet
- Maxilary Sinus Graft ArunDocument181 pagesMaxilary Sinus Graft ArunJose Fernando Fragozo MendozaNo ratings yet
- Capitulo Do Livro Bone BiologyDocument15 pagesCapitulo Do Livro Bone BiologyLuiz Guilherme FiorinNo ratings yet
- Obs-13 240122 184549Document51 pagesObs-13 240122 184549Edison MesacheNo ratings yet
- Biología Celular Metabolismo OseoDocument12 pagesBiología Celular Metabolismo Oseoandreaelisa17No ratings yet
- Lecture Activities No. 6 Skeletal System: Guide Questions AnswersDocument13 pagesLecture Activities No. 6 Skeletal System: Guide Questions AnswersPrancheska Abigayle Peneyra SantiagoNo ratings yet
- Biology of Tooth Movement - Ortho / Orthodontic Courses by Indian Dental AcademyDocument62 pagesBiology of Tooth Movement - Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- English 20.05.2020Document100 pagesEnglish 20.05.2020Bernythefly axcNo ratings yet
- Physiological Bases of Bone Regeneration II. The Remodeling ProcessDocument7 pagesPhysiological Bases of Bone Regeneration II. The Remodeling ProcessNelly Solange TamayoNo ratings yet
- Effect of The Nano/microscale Structure of Biomaterial Scaffolds On Bone RegenerationDocument15 pagesEffect of The Nano/microscale Structure of Biomaterial Scaffolds On Bone RegenerationjmanuelNo ratings yet
- Bone Grafts and Their SubstitutesDocument4 pagesBone Grafts and Their SubstitutesIndriastuti SoetomoNo ratings yet
- Biology of Normal Bone Remodeling 2017Document5 pagesBiology of Normal Bone Remodeling 2017Amani FezaiNo ratings yet
- Biology of Tooth MovementDocument16 pagesBiology of Tooth MovementLanaNo ratings yet
- Biology of Orthodontic Tooth MovementDocument16 pagesBiology of Orthodontic Tooth MovementGowri ShankarNo ratings yet
- Chemistry Project On Estimation of Content of Bone AshDocument13 pagesChemistry Project On Estimation of Content of Bone AshShlok Sah50% (2)
- Skeletal System ReviewerDocument19 pagesSkeletal System ReviewerChloe Mikaela MonsantoNo ratings yet
- Osteoblasts, Osteoclasts, and Osteocytes: Unveiling Their Intimate-Associated Responses To Applied Orthodontic ForcesDocument12 pagesOsteoblasts, Osteoclasts, and Osteocytes: Unveiling Their Intimate-Associated Responses To Applied Orthodontic ForcesMariya NazimNo ratings yet
- Bone Injury and Fracture Healing Biology: ArticleDocument16 pagesBone Injury and Fracture Healing Biology: Articleali amerNo ratings yet
- Bones As A Living Dynamic TissueDocument13 pagesBones As A Living Dynamic TissueSanish Basnet100% (1)
- Pathophysiology and Treatment of Osteoporosis: Challenges For Clinical Practice in Older PeopleDocument15 pagesPathophysiology and Treatment of Osteoporosis: Challenges For Clinical Practice in Older PeopleDeddy ZulkarnaenNo ratings yet
- Normal Bone Anatomy and PhysiologyDocument9 pagesNormal Bone Anatomy and PhysiologyindrapratisthaNo ratings yet
- Chemistry Project On Estimation of Content of Bone AshDocument18 pagesChemistry Project On Estimation of Content of Bone AshKim TaesiNo ratings yet
- ChemistryDocument29 pagesChemistryIshkruti WaghmareNo ratings yet
- 06 KnightDocument5 pages06 Knightcristina ArraisNo ratings yet
- Bone Regeneration Molecular and Cellular InteractionsDocument17 pagesBone Regeneration Molecular and Cellular InteractionsRuben Aquino MartinezNo ratings yet
- A Brief Introduction Into Orthopaedic ImplantsDocument20 pagesA Brief Introduction Into Orthopaedic ImplantsLuisAngelPonceTorresNo ratings yet
- Tereos - Structure of PresentationDocument72 pagesTereos - Structure of PresentationSumitNo ratings yet
- HHS Public Access: The Potential of Probiotics As A Therapy For OsteoporosisDocument26 pagesHHS Public Access: The Potential of Probiotics As A Therapy For OsteoporosisBagastyoNo ratings yet
- BONE (Histology)Document65 pagesBONE (Histology)fhfebriiNo ratings yet
- Bone Remodelling: Scientific SectionDocument7 pagesBone Remodelling: Scientific SectionRohini TondaNo ratings yet
- Bone RegenereationDocument15 pagesBone Regenereationhayet debbichNo ratings yet
- Role of RANKL-RANK-osteoprotegerinDocument7 pagesRole of RANKL-RANK-osteoprotegerinsebastian BarrigaNo ratings yet
- Bone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthDocument3 pagesBone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthHarsh Kumar0% (3)
- Alveolarbone Graftingand Reconstruction Procedurespriorto ImplantplacementDocument10 pagesAlveolarbone Graftingand Reconstruction Procedurespriorto ImplantplacementKranti PrajapatiNo ratings yet
- BP MecanismDocument14 pagesBP MecanismAdryana StefyNo ratings yet
- (ANA) - Online ActivityDocument4 pages(ANA) - Online ActivityJomari ManalansanNo ratings yet
- t3 Som 2014 2Document14 pagest3 Som 2014 2Julio AbarzuaNo ratings yet
- Arnett, T.Document10 pagesArnett, T.Alex AmorimNo ratings yet
- Factors of Bone Resorption of The Residual Ridge Ortman1962Document12 pagesFactors of Bone Resorption of The Residual Ridge Ortman1962AbdelKhalek BouararaNo ratings yet
- Bones: Defination: Bone Is Highly Vascular, Living, Constantly ChangingDocument21 pagesBones: Defination: Bone Is Highly Vascular, Living, Constantly ChangingMd Ahsanuzzaman PinkuNo ratings yet
- Zhu 2021Document31 pagesZhu 2021Nazmi ZegarraNo ratings yet
- Basic of Bone GraftingDocument29 pagesBasic of Bone GraftingdoctorniravNo ratings yet
- Session #14 SAS - AnaPhy (Lab)Document8 pagesSession #14 SAS - AnaPhy (Lab)G INo ratings yet
- Aaid Joi D 17 00053Document11 pagesAaid Joi D 17 00053Yun De LinNo ratings yet
- Teaching Series BoneDocument26 pagesTeaching Series BoneNAND KUMARNo ratings yet
- Bone Physiology DR NzauDocument84 pagesBone Physiology DR NzauNzau MuangeNo ratings yet
- 1.1 Bone Function: 2 OsteoarchaeologyDocument5 pages1.1 Bone Function: 2 OsteoarchaeologyKeila MenaNo ratings yet
- Basic Bone BiologyDocument3 pagesBasic Bone BiologyRuxandra Maria100% (1)
- General Anatomy: 1. SupportDocument4 pagesGeneral Anatomy: 1. SupportNu Ri LeeNo ratings yet
- Advances in Biology of Orthodontic Tooth Movement - A ReviewDocument10 pagesAdvances in Biology of Orthodontic Tooth Movement - A ReviewMarwan AlareqiNo ratings yet
- 6 PATHO 3b Part 1 - Musculoskeletal IIA - Dr. Dy-LedesmaDocument12 pages6 PATHO 3b Part 1 - Musculoskeletal IIA - Dr. Dy-LedesmaBanana BananaNo ratings yet
- Kenkre Bassett 2018 The Bone Remodelling CycleDocument20 pagesKenkre Bassett 2018 The Bone Remodelling Cyclealealer2708No ratings yet
- Normal Bone Anatomy and PhysiologyDocument9 pagesNormal Bone Anatomy and PhysiologyElsa GonçalvesNo ratings yet
- Bone Remodeling Process: Mechanics, Biology, and Numerical ModelingFrom EverandBone Remodeling Process: Mechanics, Biology, and Numerical ModelingNo ratings yet
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Hayek DKKDocument7 pagesHayek DKKwatidinaNo ratings yet
- A Conservative Technique For Repairing Class IV Composite RestorationsDocument6 pagesA Conservative Technique For Repairing Class IV Composite RestorationswatidinaNo ratings yet
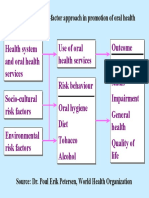
- Figure 5: The Risk-Factor Approach in Promotion of Oral HealthDocument1 pageFigure 5: The Risk-Factor Approach in Promotion of Oral HealthwatidinaNo ratings yet
- Soal 3Document5 pagesSoal 3watidinaNo ratings yet
- Kanagalingam2015 PDFDocument10 pagesKanagalingam2015 PDFwatidinaNo ratings yet
- Antiseptics in The Era of Bacterial Resistance A Focus On Povidone IodineDocument14 pagesAntiseptics in The Era of Bacterial Resistance A Focus On Povidone IodinewatidinaNo ratings yet
- Scanned With CamscannerDocument7 pagesScanned With CamscannerwatidinaNo ratings yet
- A Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivityDocument5 pagesA Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivitywatidinaNo ratings yet
- A Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivityDocument5 pagesA Brief Study On Catharanthus Roseus: A Review: Anti-Microbial ActivitywatidinaNo ratings yet
- Prevention and Control of Noncommunicable DiseasesDocument3 pagesPrevention and Control of Noncommunicable DiseaseswatidinaNo ratings yet
- 2 2 15 923 PDFDocument4 pages2 2 15 923 PDFwatidina100% (1)
- Daftar PustakaDocument1 pageDaftar PustakawatidinaNo ratings yet
- GBRI WELL AP Exam Prep Study Guide Unlocked PDFDocument150 pagesGBRI WELL AP Exam Prep Study Guide Unlocked PDFAngelo Mar MallariNo ratings yet
- Organ System WorksheetDocument23 pagesOrgan System Worksheetsrisuhartini0% (1)
- Bams AllxcfgxfDocument104 pagesBams AllxcfgxfRaheel Bhai0% (1)
- Science7 Q2 Week3 LAS2Document1 pageScience7 Q2 Week3 LAS2Irish Beth Tambo-onNo ratings yet
- Table No.1A Work Done Ground Section of Tooth (L.S, T.S) S. No. Date Title SignatureDocument38 pagesTable No.1A Work Done Ground Section of Tooth (L.S, T.S) S. No. Date Title SignatureSmila Mahajan NangiaNo ratings yet
- (11.10) Imaging of The Endocrine System (TG1-CG14) Final VersionDocument12 pages(11.10) Imaging of The Endocrine System (TG1-CG14) Final VersionLANCE GILL TolentinoNo ratings yet
- Biology Notes For O LevelsDocument13 pagesBiology Notes For O Levelstahira mujahidNo ratings yet
- Case Study RevisedDocument8 pagesCase Study RevisedKjetil Rossignol100% (1)
- Haematology: Normal Sequence of Development of Cells of Haematopoietic SystemDocument71 pagesHaematology: Normal Sequence of Development of Cells of Haematopoietic SystemMaxamed AadanNo ratings yet
- Body Systems PuzzleDocument6 pagesBody Systems PuzzleNenita AlonzoNo ratings yet
- Cell Analogy ProjectDocument3 pagesCell Analogy ProjectAP - 10KG 732763 John Fraser SSNo ratings yet
- 6 B&B CirrhosisDocument30 pages6 B&B CirrhosisSara Joseph100% (1)
- Htaa Pathology Handbook 2018Document252 pagesHtaa Pathology Handbook 2018OTOH RAYA OMARNo ratings yet
- HydraDocument6 pagesHydraMishti2100% (2)
- Coronary Artery Disease - Case StudyDocument19 pagesCoronary Artery Disease - Case StudyJulieteeySarania100% (3)
- Chapter 13 - Cranial Nerve ReviewDocument14 pagesChapter 13 - Cranial Nerve ReviewCiprian HronaNo ratings yet
- Human ReproductionDocument2 pagesHuman ReproductionGrace KatjiovaNo ratings yet
- Iliac Crest: From Wikipedia, The Free EncyclopediaDocument4 pagesIliac Crest: From Wikipedia, The Free EncyclopediaMarigold CortezNo ratings yet
- Anatomy & Physiology: Chapter 7: Skeletal SystemDocument25 pagesAnatomy & Physiology: Chapter 7: Skeletal SystemDarandy CruzNo ratings yet
- Short Note Biology Form 5-Chapter 3 Coordination and ResponseDocument6 pagesShort Note Biology Form 5-Chapter 3 Coordination and Responsesalamah_sabri75% (4)
- Cancers: Cell Origins of High-Grade Serous Ovarian CancerDocument28 pagesCancers: Cell Origins of High-Grade Serous Ovarian CancerAlfonso AnggriawanNo ratings yet
- MCQ in Orl CourseDocument46 pagesMCQ in Orl CoursesulnaikNo ratings yet
- Clinics in Sports Medicine PDFDocument173 pagesClinics in Sports Medicine PDFmostafa143941366No ratings yet
- Yellow Green Blue and Red Handwritten Zones of Regulation SEL Social and Emotional Learning Education PresentationDocument15 pagesYellow Green Blue and Red Handwritten Zones of Regulation SEL Social and Emotional Learning Education PresentationAngel ChrisleneNo ratings yet
- Lesson Plan: Preliminary DetailsDocument7 pagesLesson Plan: Preliminary DetailsMurali SambhuNo ratings yet