You might also like
- Heart LectureDocument38 pagesHeart Lecturesamer3383No ratings yet
- Antiplatelet Medications Mechanism AtfDocument4 pagesAntiplatelet Medications Mechanism AtfAmir mohammad moori MohammadiNo ratings yet
- Cardiotonic Drugs Revised DheryanDocument16 pagesCardiotonic Drugs Revised Dheryanlinnet17No ratings yet
- Physio 3Document5 pagesPhysio 3Mohammad AlomariNo ratings yet
- Inotropes and Vasopressors - Circulation. 2008Document11 pagesInotropes and Vasopressors - Circulation. 2008Dani AguirreNo ratings yet
- Individual AssignmentDocument3 pagesIndividual AssignmentPutri Rizky AmaliaNo ratings yet
- Renal PhysiologyDocument20 pagesRenal PhysiologyRana SohelNo ratings yet
- Urinary Module NotesDocument22 pagesUrinary Module NotesAthira SureshNo ratings yet
- s13 ArtDocument9 pagess13 ArtRober Nuñez AlbercaNo ratings yet
- D - Water and Electrolyte Balance of KidneyDocument6 pagesD - Water and Electrolyte Balance of KidneyNav ThiranNo ratings yet
- Heart Failure PharmDocument7 pagesHeart Failure PharmAmitShettyNo ratings yet
- Mod04 - HF Pharm - Fall2020Document25 pagesMod04 - HF Pharm - Fall2020RafaelNo ratings yet
- Stores in MPTP OpeningDocument20 pagesStores in MPTP OpeningCarolina RicárdezNo ratings yet
- Cardiovascular Pharmacology Part TwoDocument50 pagesCardiovascular Pharmacology Part Twoelias adugnaNo ratings yet
- General Principles of Tubular ReabsorptionDocument54 pagesGeneral Principles of Tubular ReabsorptionRalph JacintoNo ratings yet
- Atrial Natriuretic PeptideDocument4 pagesAtrial Natriuretic PeptideZiedTrikiNo ratings yet
- CVS VasodilatorsDocument45 pagesCVS Vasodilatorsapi-3723461100% (1)
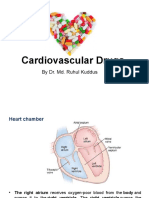
- Cardiovascular Drugs: by Dr. Md. Ruhul KuddusDocument56 pagesCardiovascular Drugs: by Dr. Md. Ruhul Kuddus53-Deepankar SutradharNo ratings yet
- Halo On Bright Objects) ArrhythmiaDocument9 pagesHalo On Bright Objects) ArrhythmiaNoriko MatsumotoNo ratings yet
- Second LectrueDocument44 pagesSecond Lectrueapi-3700537No ratings yet
- Congestive Heart FailureDocument72 pagesCongestive Heart FailureCharles YiuNo ratings yet
- Endo ShortlistingDocument3 pagesEndo ShortlistingMamoona RazzaqNo ratings yet
- Intern Survival GuideDocument12 pagesIntern Survival GuideHunter RossNo ratings yet
- Table 4-2. Mechanism of Action of Selected Nonpeptide NeurotransmittersDocument1 pageTable 4-2. Mechanism of Action of Selected Nonpeptide NeurotransmittersaustinchenNo ratings yet
- Renin Angio Sys 1Document27 pagesRenin Angio Sys 1SHRIKANTNo ratings yet
- Antianginal DrugsDocument38 pagesAntianginal Drugslemmademe204No ratings yet
- Static58e8b95bf5e231a18a2c2907t93746anticoagulants PDFDocument10 pagesStatic58e8b95bf5e231a18a2c2907t93746anticoagulants PDFNav ThiranNo ratings yet
- Kuliah S2 Dasar Air-ElekDocument38 pagesKuliah S2 Dasar Air-ElekViany RehansyahNo ratings yet
- Pi Is 1548559517301222Document7 pagesPi Is 1548559517301222Obito AkatsukiNo ratings yet
- Biokimia KardioDocument98 pagesBiokimia KardioirmaNo ratings yet
- Slow Flow of BloodDocument6 pagesSlow Flow of Blood黃郁晴No ratings yet
- 5 RenalDocument10 pages5 RenalAli EllaffiNo ratings yet
- Kreb's CycleDocument8 pagesKreb's CycleHaneen HafizNo ratings yet
- NOTZ SUMMARY - Aldosterone TableDocument1 pageNOTZ SUMMARY - Aldosterone TableAdmin DutiesNo ratings yet
- CalciumDocument12 pagesCalciumSachin ChaudharyNo ratings yet
- Calcium Channel BlockersDocument28 pagesCalcium Channel Blockershap hazardNo ratings yet
- Calcium For Resuscitation?: E. Erdmann and E. Reuschel-JanetschekDocument7 pagesCalcium For Resuscitation?: E. Erdmann and E. Reuschel-JanetschekMislav HilcNo ratings yet
- VQ MM Hypoxia CopdDocument2 pagesVQ MM Hypoxia Copd6ixSideCreate MNo ratings yet
- Enzymology Part 2Document5 pagesEnzymology Part 2Ella LobenariaNo ratings yet
- Water Follows Sodium (Via OsmoticDocument3 pagesWater Follows Sodium (Via OsmoticMark Vincent SahagunNo ratings yet
- 3001 - Lecture 3 - Ecc 2022 SlidesDocument40 pages3001 - Lecture 3 - Ecc 2022 Slidesshivanibhat1612No ratings yet
- 243 - Respiratory Pathology COPD - Treatment and PreventionDocument3 pages243 - Respiratory Pathology COPD - Treatment and PreventionPranav PunjabiNo ratings yet
- 13 08045 Askandar 0840Document9 pages13 08045 Askandar 0840Fadhil Muhammad AwaluddinNo ratings yet
- Antihypertensive DrugsDocument62 pagesAntihypertensive DrugsYeshaa MiraniNo ratings yet
- Drugs Mechanism Side Effect DiureticDocument3 pagesDrugs Mechanism Side Effect DiureticRebecca MarshallNo ratings yet
- Cardiac Physiology: David Rendra Mahardika SMF Anestesiologi Dan Terapi Intensif FK UNUD/RSUP Sanglah DenpasarDocument29 pagesCardiac Physiology: David Rendra Mahardika SMF Anestesiologi Dan Terapi Intensif FK UNUD/RSUP Sanglah DenpasarEka AriasyahNo ratings yet
- Renal PhysiologyDocument84 pagesRenal PhysiologyFauzan HafizNo ratings yet
- Control of Normal Cardiac Contractility: Contraction Results From The Interaction of Activator CaDocument24 pagesControl of Normal Cardiac Contractility: Contraction Results From The Interaction of Activator CaDana HamarshehNo ratings yet
- Urinary Concentration and DilutionDocument10 pagesUrinary Concentration and DilutionAbhineeth BhatNo ratings yet
- Agents Used in Cardiac ArrythmiasDocument79 pagesAgents Used in Cardiac ArrythmiasBrother GeorgeNo ratings yet
- Renal Physiology For The BoardsDocument37 pagesRenal Physiology For The BoardsRainy Day100% (1)
- CalcioDocument6 pagesCalcioArtur Franck Tenorio AronésNo ratings yet
- W2 PHARMACOLOGY OF DIURETICS Short Notes 2017Document6 pagesW2 PHARMACOLOGY OF DIURETICS Short Notes 2017Syximsh FPNo ratings yet
- Bio 93 Midterm 2 Review Session KEYDocument121 pagesBio 93 Midterm 2 Review Session KEYKenosNo ratings yet
- Calcium As A Secondary Messenger in Cell SignallingDocument5 pagesCalcium As A Secondary Messenger in Cell Signallingjeanoriordan02No ratings yet
- Hypokalemia FT 2020Document49 pagesHypokalemia FT 2020ebkai98No ratings yet
- Segue 1Document2 pagesSegue 1miorrNo ratings yet
- Sodium and Potassium - Atp Ase PumpDocument18 pagesSodium and Potassium - Atp Ase PumpYaswanthyadavNo ratings yet
- Sodium Pottasium PumpDocument15 pagesSodium Pottasium Pumpbiomedikbiokimiausu2014100% (1)
- CutOff Report RP 2016Document17 pagesCutOff Report RP 2016AdityaBhagiNo ratings yet
- Civil Prelims Exam 2018 Set BDocument16 pagesCivil Prelims Exam 2018 Set BRashmi SahooNo ratings yet
- CutOff Report RP 09052014Document14 pagesCutOff Report RP 09052014NTA UGC-NETNo ratings yet
- Research Program CutOff Report 2017 IIScDocument11 pagesResearch Program CutOff Report 2017 IIScLeela Krishna VegiNo ratings yet
- Cutoff Report Forrp Web 35 PDFDocument20 pagesCutoff Report Forrp Web 35 PDFGaurab SarkarNo ratings yet
- CutOff Report ForResearch 2015Document15 pagesCutOff Report ForResearch 2015DharmaTejaNo ratings yet
- Hypothalamic-Pituitary-Adrenal AxisDocument11 pagesHypothalamic-Pituitary-Adrenal AxisNTA UGC-NETNo ratings yet
- VasopressinDocument17 pagesVasopressinNTA UGC-NETNo ratings yet
- Hyper GlycemiaDocument7 pagesHyper GlycemiaNTA UGC-NETNo ratings yet
- Inbreeding: Understanding The Inbreeding NumbersDocument3 pagesInbreeding: Understanding The Inbreeding NumbersNTA UGC-NETNo ratings yet
- Homoplasy: Homoplastic. It Is Derived From The Two Ancient Greek WordsDocument5 pagesHomoplasy: Homoplastic. It Is Derived From The Two Ancient Greek WordsNTA UGC-NETNo ratings yet
- Viral VectorDocument7 pagesViral VectorNTA UGC-NETNo ratings yet
- SynaptojaninDocument5 pagesSynaptojaninNTA UGC-NETNo ratings yet
- Bio in For MaticsDocument18 pagesBio in For MaticsNTA UGC-NETNo ratings yet
- Cushing's SyndromeDocument11 pagesCushing's SyndromeNTA UGC-NETNo ratings yet
- SGLTDocument4 pagesSGLTNTA UGC-NETNo ratings yet
- Synapomorphy & ApomorphyDocument4 pagesSynapomorphy & ApomorphyNTA UGC-NETNo ratings yet
- Vasodilation: Vasodilation Is The Widening of Blood VesselsDocument8 pagesVasodilation: Vasodilation Is The Widening of Blood VesselsNTA UGC-NETNo ratings yet
- Bio Vs PhytoDocument23 pagesBio Vs PhytoNTA UGC-NETNo ratings yet
- Periodic BreathingDocument1 pagePeriodic BreathingNTA UGC-NETNo ratings yet
- ProlactinDocument15 pagesProlactinNTA UGC-NETNo ratings yet
- VasoconstrictionDocument6 pagesVasoconstrictionNTA UGC-NETNo ratings yet
- Group SelectionDocument12 pagesGroup SelectionNTA UGC-NETNo ratings yet
- Haldane's RuleDocument4 pagesHaldane's RuleNTA UGC-NETNo ratings yet
- Plesiomorphy and SymplesiomorphyDocument3 pagesPlesiomorphy and SymplesiomorphyNTA UGC-NETNo ratings yet
- Plasmids 101 Ebook 3rd Ed FinalDocument193 pagesPlasmids 101 Ebook 3rd Ed FinalManuel CamachoNo ratings yet
- Graves' DiseaseDocument15 pagesGraves' DiseaseNTA UGC-NETNo ratings yet
- Organ of CortiDocument6 pagesOrgan of CortiNTA UGC-NETNo ratings yet
- Phosphoribosylanthranilate IsomeraseDocument7 pagesPhosphoribosylanthranilate IsomeraseNTA UGC-NETNo ratings yet
- ChromatographyDocument12 pagesChromatographyNTA UGC-NETNo ratings yet
- A2 Buguina Peaches A.Document7 pagesA2 Buguina Peaches A.Peach Amparo BuguinaNo ratings yet
- Acid and BasesDocument4 pagesAcid and BasesMika SaldañaNo ratings yet
- The Owner's Manual For The Brain - PDF RoomDocument114 pagesThe Owner's Manual For The Brain - PDF RoomMustafa FarahmandNo ratings yet
- Botany Plant Anatomy SEM II H SEM I GDocument34 pagesBotany Plant Anatomy SEM II H SEM I GMartha-Angella MassaquoiNo ratings yet
- Case Study - The Case of The Painful Hands - SPR 2021Document5 pagesCase Study - The Case of The Painful Hands - SPR 2021Nicholas LeeNo ratings yet
- Positioning of Arterial Line Transducer at The Phlebostatic AxisDocument2 pagesPositioning of Arterial Line Transducer at The Phlebostatic AxisRudi HaryantoNo ratings yet
- 1 Klöppel Vortrag GEP NET The NE System 120217Document32 pages1 Klöppel Vortrag GEP NET The NE System 120217soledad88No ratings yet
- Ficha para Inventario de HuesosDocument24 pagesFicha para Inventario de HuesosAntony CevallosNo ratings yet
- Endocrinology PhysiologyDocument2 pagesEndocrinology PhysiologyzeeshanNo ratings yet
- CB7 All SheetsDocument38 pagesCB7 All SheetsAryan AdhikariNo ratings yet
- IB Style Test - Topic 8 HL Metabolism, Respiration and PhotosynthesisDocument8 pagesIB Style Test - Topic 8 HL Metabolism, Respiration and Photosynthesisika100% (1)
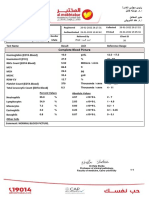
- Complete Blood Picture: 33 Year Male 29822507118Document4 pagesComplete Blood Picture: 33 Year Male 29822507118sayedaaeNo ratings yet
- CH-8 Notebook Work-Answer KeyDocument2 pagesCH-8 Notebook Work-Answer KeyEeshan SharmaNo ratings yet
- 1-Comprehensive Full Body Checkup - PO3310643047-461Document19 pages1-Comprehensive Full Body Checkup - PO3310643047-461newskishore100% (1)
- 3.4 - Parasit Pada Sistem Nefrourinarius - 2022Document38 pages3.4 - Parasit Pada Sistem Nefrourinarius - 202227rayhan rizqikaNo ratings yet
- CSEC Integrated Science June 1995 P1Document7 pagesCSEC Integrated Science June 1995 P1Saintm101No ratings yet
- Bio102 General Biology II SummaryDocument47 pagesBio102 General Biology II SummaryIkenna Okpala100% (1)
- Lesson 4: Anatomy and Physiology of Reproduction: Gee 2 - Gender & Society Dr. Teri Marie P. Laude Et. AlDocument1 pageLesson 4: Anatomy and Physiology of Reproduction: Gee 2 - Gender & Society Dr. Teri Marie P. Laude Et. AlRexson Dela Cruz TagubaNo ratings yet
- Anatomy and Physiology CVADocument11 pagesAnatomy and Physiology CVAmaryrose_jordan100% (6)
- BC Tiempo de Trombina Inserto OWNAG11E05Document6 pagesBC Tiempo de Trombina Inserto OWNAG11E05Isa Mar BCNo ratings yet
- snpwp97,+2376 2581 1 PBDocument4 pagessnpwp97,+2376 2581 1 PBChristalie Bea FernandezNo ratings yet
- Functions of The Human Respiratory System: What's inDocument4 pagesFunctions of The Human Respiratory System: What's injoyNo ratings yet
- Anti AgingDocument6 pagesAnti AgingZubair Akram JanjuaNo ratings yet
- Photosynthesiscombinedpogil 3Document9 pagesPhotosynthesiscombinedpogil 3Shaojie HeNo ratings yet
- Energy Gates QigongDocument43 pagesEnergy Gates QigongElena VlasceanuNo ratings yet
- Cholinergic DrugsDocument22 pagesCholinergic Drugsmug ashNo ratings yet
- Gen BioDocument86 pagesGen BioPaul MagbagoNo ratings yet
- Physiology AccommodationDocument109 pagesPhysiology AccommodationAmmar bushraNo ratings yet
- Your Guide To Success - The Big Guide To Yoga 2024Document148 pagesYour Guide To Success - The Big Guide To Yoga 2024saracena23No ratings yet
- IB DP Biology 1.3 Membrane Structure QuestionDocument15 pagesIB DP Biology 1.3 Membrane Structure QuestionikaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)