You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pediatric Cardiovascular DisordersDocument9 pagesPediatric Cardiovascular Disorderscayla mae carlos0% (1)
- OnlineWOD Open Prep Program 7 Day Trial PDFDocument8 pagesOnlineWOD Open Prep Program 7 Day Trial PDFJomari ServanoNo ratings yet
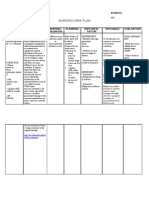
- NCP Tissue Perfusion For Pre-EclampsiaDocument2 pagesNCP Tissue Perfusion For Pre-Eclampsiaanreilegarde83% (23)
- Gapuz Review CenterDocument3 pagesGapuz Review CenterKyle CasanguanNo ratings yet
- Newborn Disorders - : Small For Gestational Age (Sga) NewbornDocument11 pagesNewborn Disorders - : Small For Gestational Age (Sga) Newborncayla mae carlos100% (1)
- Stages of LabourDocument43 pagesStages of LabourhaisureshNo ratings yet
- Pediatric Genitourinary DisordersDocument7 pagesPediatric Genitourinary Disorderscayla mae carlosNo ratings yet
- Separating MixturesDocument30 pagesSeparating Mixturescayla mae carlosNo ratings yet
- Practice Application of Nursing InformaticsDocument3 pagesPractice Application of Nursing Informaticscayla mae carlos100% (3)
- BKD Project ShareDocument3 pagesBKD Project ShareAbby- Gail14 CabralNo ratings yet
- HACCP Plan For ChikenDocument8 pagesHACCP Plan For ChikenPeter George0% (1)
- The Need of Improving Social Sustainability in Sri Lankan Construction ProjectsDocument28 pagesThe Need of Improving Social Sustainability in Sri Lankan Construction Projectslakshan mahanamaNo ratings yet
- Local Anaesthetic Dosing For Male CircumcisionDocument4 pagesLocal Anaesthetic Dosing For Male CircumcisionAssenav ZednemNo ratings yet
- The WASH Benefits Bangladesh, WASH Benefits Kenya, and SHINE Trials: A Summary of Their FindingsDocument2 pagesThe WASH Benefits Bangladesh, WASH Benefits Kenya, and SHINE Trials: A Summary of Their Findingscayla mae carlosNo ratings yet
- For Learners Handwashing StepsDocument1 pageFor Learners Handwashing Stepscayla mae carlosNo ratings yet
- Arrythmias 2-3Document4 pagesArrythmias 2-3cayla mae carlosNo ratings yet
- Pediatric Respiratory Disorders General InterventionsDocument2 pagesPediatric Respiratory Disorders General Interventionscayla mae carlosNo ratings yet
- Extraordinary Measures Jop 13 346Document1 pageExtraordinary Measures Jop 13 346cayla mae carlosNo ratings yet
- Cop Lec - Unit Iv - Physical Care of OlderDocument3 pagesCop Lec - Unit Iv - Physical Care of Oldercayla mae carlosNo ratings yet
- Problems With Eating and Feeding, Incontinence, Confusion, Evidence of Falls, and Skin BreakdownDocument1 pageProblems With Eating and Feeding, Incontinence, Confusion, Evidence of Falls, and Skin Breakdowncayla mae carlosNo ratings yet
- The COVIDDocument2 pagesThe COVIDcayla mae carlosNo ratings yet
- Lumad's Belief and ValuesDocument1 pageLumad's Belief and Valuescayla mae carlosNo ratings yet
- Made of A-Grade Poured Concrete and Over-Sized Steel Bars, With Thick Hardwood FlooringDocument2 pagesMade of A-Grade Poured Concrete and Over-Sized Steel Bars, With Thick Hardwood Flooringcayla mae carlosNo ratings yet
- Parental ConsentDocument1 pageParental Consentcayla mae carlosNo ratings yet
- Subject Code Subject Title Course Grade Numeric EquivalentDocument2 pagesSubject Code Subject Title Course Grade Numeric Equivalentcayla mae carlosNo ratings yet
- Diseases of The Digestive SystemDocument5 pagesDiseases of The Digestive SystemmeiuuNo ratings yet
- Ig2 Risk Assessment Self Evaluation ChecklistDocument2 pagesIg2 Risk Assessment Self Evaluation ChecklistprinceNo ratings yet
- How To Run An Effective Journal Club A Systematic ReviewDocument14 pagesHow To Run An Effective Journal Club A Systematic Reviewsidra khaliqNo ratings yet
- Hypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood PressureDocument3 pagesHypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood Pressurejoanneceline16No ratings yet
- The-Effects-of - Social-Media-on-a-TeenagersDocument13 pagesThe-Effects-of - Social-Media-on-a-TeenagersJanella EuniceNo ratings yet
- Rodriguez, B. O., & Sanchez, T. L. (2020) .Document6 pagesRodriguez, B. O., & Sanchez, T. L. (2020) .Yanreza Dwi HermawanNo ratings yet
- Paradise TrialDocument26 pagesParadise TrialMiguel Martinez DuranNo ratings yet
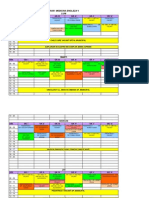
- Orar Medicina Engleza V Luni: ORA Gr. I Gr. Ii Gr. Iii Gr. Iv Gr. V Gr. ViDocument3 pagesOrar Medicina Engleza V Luni: ORA Gr. I Gr. Ii Gr. Iii Gr. Iv Gr. V Gr. ViCornel MihaiNo ratings yet
- Think Global Manila ProgramDocument16 pagesThink Global Manila ProgramRenzo R. GuintoNo ratings yet
- Indonesia Case StudyDocument42 pagesIndonesia Case StudyChad McMillenNo ratings yet
- February 2016 Ophthalmic Pearls PDFDocument3 pagesFebruary 2016 Ophthalmic Pearls PDFIndah IndrianiNo ratings yet
- PneumoniaDocument8 pagesPneumoniaNader Smadi100% (2)
- Cor Jesu College, IncDocument12 pagesCor Jesu College, Incalmira garciaNo ratings yet
- Case Study About Food Safety and SecurityDocument3 pagesCase Study About Food Safety and SecurityALCARAZ ChristineNo ratings yet
- Phoebe Lam ResumeDocument1 pagePhoebe Lam ResumeAnonymous 9gOf6VGNo ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument12 pagesPsychiatric Mental Health Comprehensive Case Studyapi-508432180No ratings yet
- Monthly Health CalendarDocument4 pagesMonthly Health CalendarMercicae ANo ratings yet
- Nurse Role in Caring For Women Victim of Ipv Sri Lankan ContextDocument9 pagesNurse Role in Caring For Women Victim of Ipv Sri Lankan Contextkaysa refaNo ratings yet
- Ozdemir Et Al-2015-Journal of Advanced Nursing PDFDocument15 pagesOzdemir Et Al-2015-Journal of Advanced Nursing PDFIMaa Wati AlbiizzahNo ratings yet
- CommunityNCP Ricafort140717Document3 pagesCommunityNCP Ricafort140717Dara Ellaine RicafortNo ratings yet
- From The Desk of Vice President-Elect: Mrugesh VaishnavDocument1 pageFrom The Desk of Vice President-Elect: Mrugesh Vaishnavgion.nandNo ratings yet
- CDC - HIV in Pregnant WomenDocument2 pagesCDC - HIV in Pregnant WomenMyrna Dianita SavitriNo ratings yet
- DocumentDocument4 pagesDocumentCeline RillonNo ratings yet