You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lab Experiment I Personality Traits, Free Association Test and Reaction TimeDocument134 pagesLab Experiment I Personality Traits, Free Association Test and Reaction TimeFatima Malik100% (1)
- Cosmology: Beyond The Big BangDocument60 pagesCosmology: Beyond The Big BangHaris_IsaNo ratings yet
- Peace Psychology in AsiaDocument16 pagesPeace Psychology in AsiaFatima Malik91% (11)
- Design ParameterDocument13 pagesDesign ParameterkennysawegNo ratings yet
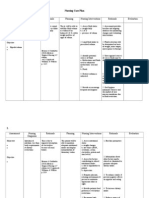
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- IGEM-UP-1C Draft For Comment - 2nd Consultation (IGEM-TSP-10-122)Document54 pagesIGEM-UP-1C Draft For Comment - 2nd Consultation (IGEM-TSP-10-122)eastway98100% (2)
- GratitudeDocument10 pagesGratitudeFatima Malik100% (1)
- Transportation EngineeringDocument312 pagesTransportation EngineeringCourtney Ward75% (4)
- Emotional Intelligence NotesDocument24 pagesEmotional Intelligence NotesFatima Malik67% (3)
- Adult Case Report Format PDFDocument11 pagesAdult Case Report Format PDFFatima Malik0% (1)
- Vendetta by Catherine Doyle EXCERPTDocument33 pagesVendetta by Catherine Doyle EXCERPTI Read YA50% (2)
- Preliminary Report School Child 2Document4 pagesPreliminary Report School Child 2Fatima MalikNo ratings yet
- Why We Need Statistics in Clinical PsychologyDocument12 pagesWhy We Need Statistics in Clinical PsychologyFatima Malik100% (1)
- Group ObservationDocument4 pagesGroup ObservationFatima MalikNo ratings yet
- Case Report School PsychologyDocument9 pagesCase Report School PsychologyFatima Malik100% (1)
- DSM 5 Checklist For Major Depressive DisorderDocument1 pageDSM 5 Checklist For Major Depressive DisorderFatima MalikNo ratings yet
- Rehabilitation Is Defined AsDocument10 pagesRehabilitation Is Defined AsFatima MalikNo ratings yet
- 3behavioral ObservationDocument3 pages3behavioral ObservationFatima MalikNo ratings yet
- Positive Psychology Wisdom ND HopeDocument22 pagesPositive Psychology Wisdom ND HopeFatima MalikNo ratings yet
- Preliminary Report 1Document4 pagesPreliminary Report 1Fatima MalikNo ratings yet
- Samra Shehzadi, Peace Psy, Assignment 1Document12 pagesSamra Shehzadi, Peace Psy, Assignment 1Fatima MalikNo ratings yet
- 5bender Gestalt TestDocument1 page5bender Gestalt TestFatima MalikNo ratings yet
- Assignment # 3, Group 4, Clinical Psychology IIDocument9 pagesAssignment # 3, Group 4, Clinical Psychology IIFatima MalikNo ratings yet
- Peace Psychology Chapter 3Document43 pagesPeace Psychology Chapter 3Fatima Malik100% (1)
- Cognitive ProcessesDocument22 pagesCognitive ProcessesFatima MalikNo ratings yet
- Aiman 019309 Peace Psychologyassignment 1Document8 pagesAiman 019309 Peace Psychologyassignment 1Fatima MalikNo ratings yet
- Problem Solving by Nine DotsDocument6 pagesProblem Solving by Nine DotsFatima Malik100% (1)
- Muqaddas SarwarDocument1 pageMuqaddas SarwarFatima MalikNo ratings yet
- Contribution To The Professionalization of The Field of Peace-BuildingDocument5 pagesContribution To The Professionalization of The Field of Peace-BuildingFatima MalikNo ratings yet
- Proselytizing TechniqueDocument4 pagesProselytizing TechniqueFatima Malik100% (1)
- Contribution To The Professionalization of The Field of Peace-BuildingDocument5 pagesContribution To The Professionalization of The Field of Peace-BuildingFatima MalikNo ratings yet
- Perception MsDocument15 pagesPerception MsFatima MalikNo ratings yet
- Experiment No. 4 Reaction Time For Visual Stimuli With and Without MusicDocument8 pagesExperiment No. 4 Reaction Time For Visual Stimuli With and Without MusicFatima MalikNo ratings yet
- Nutrition & Wound Care: Christina Merryfield, Lead Dietitian, Bupa Cromwell HospitalDocument4 pagesNutrition & Wound Care: Christina Merryfield, Lead Dietitian, Bupa Cromwell HospitalhafiezAmandaNo ratings yet
- Chapter 04 Skeletal NotesDocument36 pagesChapter 04 Skeletal NotesElizabeth WoodNo ratings yet
- FILE - 20211123 - 141203 - de Thi Mau Tieng AnhDocument17 pagesFILE - 20211123 - 141203 - de Thi Mau Tieng AnhDo Le Quoc LapNo ratings yet
- In-Situ AbstDocument5 pagesIn-Situ AbstFahim MunawarNo ratings yet
- Ui PATH - RE FRAMEWORKDocument2 pagesUi PATH - RE FRAMEWORKsaubhagya ranjan mohapatraNo ratings yet
- Science - Grade 5 - Test QuestionsDocument6 pagesScience - Grade 5 - Test QuestionsJeric MaribaoNo ratings yet
- Symbolism and Color in Folk ArtDocument11 pagesSymbolism and Color in Folk ArtshandryssNo ratings yet
- Attachment - Statement HP 2023 January Cyan, Magenta, Yellow, and BlackDocument2 pagesAttachment - Statement HP 2023 January Cyan, Magenta, Yellow, and BlackWayan PartaNo ratings yet
- Extraction of Pectin From Citrus Fruit Peel and Use As Natural Binder in Paracetamol TabletDocument7 pagesExtraction of Pectin From Citrus Fruit Peel and Use As Natural Binder in Paracetamol TabletIshtiaque IshtiNo ratings yet
- GC Guy Wire (US) Catalog Sheet FinalDocument1 pageGC Guy Wire (US) Catalog Sheet FinalAde 'aiyie' SasmitaNo ratings yet
- Costing of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMDocument3 pagesCosting of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMMohtashim KazmiNo ratings yet
- The IMA Volumes in Mathematics and Its Applications: Avner Friedman Willard Miller, JRDocument172 pagesThe IMA Volumes in Mathematics and Its Applications: Avner Friedman Willard Miller, JRPedro PereyraNo ratings yet
- SLB Lean Level 2 Module 19 TestDocument3 pagesSLB Lean Level 2 Module 19 TestEdiith CarvajalNo ratings yet
- Harga Satuan Precast 2017Document2 pagesHarga Satuan Precast 2017GenTigaBrotherhood BantenNo ratings yet
- HUDA Policy Allowing Four BasementsDocument3 pagesHUDA Policy Allowing Four BasementsRahul JindalNo ratings yet
- NCM 117 - Case Study 1 DarundayDocument18 pagesNCM 117 - Case Study 1 DarundayEzra Miguel DarundayNo ratings yet
- Divisional Chart-IIDocument1 pageDivisional Chart-IIabhisek19870% (1)
- Catalogo ComarDocument68 pagesCatalogo ComaralbertoNo ratings yet
- Thermal EngineeringDocument23 pagesThermal Engineeringakeey4uNo ratings yet
- Dairy Sector Thematic - Initiating CoverageDocument53 pagesDairy Sector Thematic - Initiating Coverageajoy sharmaNo ratings yet
- At22 ElectricalDocument19 pagesAt22 ElectricalfabuleukalengaNo ratings yet
- Experiment 2 Sku 3033Document8 pagesExperiment 2 Sku 3033Luw InNo ratings yet
- CTR201Document2 pagesCTR201Vicente RezabalaNo ratings yet
- Peripartum Cardiomyopathy CIRCULATIONAHADocument13 pagesPeripartum Cardiomyopathy CIRCULATIONAHAJessica WiryantoNo ratings yet