You might also like
- Changing The Physical Activity Behaviour of Adults With Fitness TrackersDocument13 pagesChanging The Physical Activity Behaviour of Adults With Fitness Trackershszv9qy6x2No ratings yet
- 4 EditedDocument13 pages4 EditedEmmanuel Ayodele DavidNo ratings yet
- The Prevalence and Associated Factors of Alcohol Use During Pregnancy Among Pregnant Women in The Buea Town Health CenterDocument70 pagesThe Prevalence and Associated Factors of Alcohol Use During Pregnancy Among Pregnant Women in The Buea Town Health CenterFavour ChukwuelesieNo ratings yet
- DR Mike Proposal EditsDocument8 pagesDR Mike Proposal EditsOladele RotimiNo ratings yet
- Version of Record:: ManuscriptDocument20 pagesVersion of Record:: ManuscriptChristiana TomescuNo ratings yet
- Alcohol Misuse Literature ReviewDocument4 pagesAlcohol Misuse Literature Reviewaflstezqg100% (1)
- Kavanagh 2014 Simplifying The Assessment of AntidDocument2 pagesKavanagh 2014 Simplifying The Assessment of AntidokNo ratings yet
- 10 1016@j Sleep 2019 11 1258Document19 pages10 1016@j Sleep 2019 11 1258Renan López ViañaNo ratings yet
- Smartphone Based - Self AssessmeDocument14 pagesSmartphone Based - Self Assessmerichardong lauNo ratings yet
- Statement of The ProblemDocument7 pagesStatement of The ProblemKen Dela CernaNo ratings yet
- Internet Addiction: The Emergence of A New Clinical DisorderDocument13 pagesInternet Addiction: The Emergence of A New Clinical DisorderSminkericaNo ratings yet
- Anxiety and Depressive Symptoms Associated To Alcohol Consumption in Health Care WorkersDocument17 pagesAnxiety and Depressive Symptoms Associated To Alcohol Consumption in Health Care WorkersTania MartinezNo ratings yet
- Pharm InfoDocument3 pagesPharm InfoAL IZMI AMILHASANNo ratings yet
- Discover Evidence-Based DataDocument7 pagesDiscover Evidence-Based DataBrian MaingiNo ratings yet
- Prospero Template ProtocolDocument5 pagesProspero Template Protocolrevanth kallaNo ratings yet
- Ahj 14 218Document6 pagesAhj 14 2186rqwhg67zvNo ratings yet
- How To Prevent WPS OfficeDocument9 pagesHow To Prevent WPS OfficeOnin T. LoterteNo ratings yet
- 2019 Ramos, Cheng, & Jonas - Validation of An Mhealth App For Depression Screening and Monitoring (Psychologist in A Pocket)Document14 pages2019 Ramos, Cheng, & Jonas - Validation of An Mhealth App For Depression Screening and Monitoring (Psychologist in A Pocket)Paula FerrerNo ratings yet
- Medical Cannabis For The Treatment of DementiaDocument24 pagesMedical Cannabis For The Treatment of DementiaLorina BoligNo ratings yet
- Journal Pre-Proofs: Brain, Behavior, and ImmunityDocument26 pagesJournal Pre-Proofs: Brain, Behavior, and ImmunitycoconitaNo ratings yet
- 6HC508 - Research 00492Document10 pages6HC508 - Research 00492chetna sharmaNo ratings yet
- Cross-Sectional and Longitudinal Epidemiological Studies of Internet Gaming Disorder: A Systematic Review of The LiteratureDocument20 pagesCross-Sectional and Longitudinal Epidemiological Studies of Internet Gaming Disorder: A Systematic Review of The LiteratureJason LiberiNo ratings yet
- Paper 4Document27 pagesPaper 4lemonauthentNo ratings yet
- Articulo Salud Mental & Ejercicio Fisico en Adulto Joven y AdultoDocument19 pagesArticulo Salud Mental & Ejercicio Fisico en Adulto Joven y AdultoLIZETH DAYANA NIÑO CAMACHONo ratings yet
- WaseemDocument14 pagesWaseemwaseemNo ratings yet
- Methodology NotesDocument2 pagesMethodology Notesadacanay2020No ratings yet
- Final Manuscript PDFDocument24 pagesFinal Manuscript PDFapi-620860184No ratings yet
- Examining The Prevalence and Rise Factors of Cigarette Smoking Chap 2Document9 pagesExamining The Prevalence and Rise Factors of Cigarette Smoking Chap 2Gcs GomezNo ratings yet
- Rapid Evidence Review of Mobile Applications For Self-Management of DiabetesDocument10 pagesRapid Evidence Review of Mobile Applications For Self-Management of DiabetesNersdilahNo ratings yet
- Research MethodologyDocument199 pagesResearch MethodologyJefferson L QuidorNo ratings yet
- Literature Review On Alcohol UseDocument4 pagesLiterature Review On Alcohol Useafduaciuf100% (2)
- Untitled PDFDocument8 pagesUntitled PDFSafaa Rabea osmanNo ratings yet
- Colombo (2019) - Current State and Future Directions of Technology-Based Ecological Momentary AssesmentDocument26 pagesColombo (2019) - Current State and Future Directions of Technology-Based Ecological Momentary AssesmentElizabeth Vino FloresNo ratings yet
- Big Data Technologies in Health and BiomedicalDocument7 pagesBig Data Technologies in Health and BiomedicalAJER JOURNALNo ratings yet
- Sensors: A Wellness Mobile Application For Smart Health: Pilot Study Design and ResultsDocument24 pagesSensors: A Wellness Mobile Application For Smart Health: Pilot Study Design and ResultsShri Prashant JhaNo ratings yet
- Review ArticleDocument36 pagesReview ArticleFoncho Silva SantistebanNo ratings yet
- Caffeine-Related DeathsDocument13 pagesCaffeine-Related DeathsMaya SwariNo ratings yet
- King JournalClubDocument7 pagesKing JournalClubTimothy Samuel KingNo ratings yet
- 10 5923 J Diabetes 20170601 04Document10 pages10 5923 J Diabetes 20170601 04Dewi Luqmana SariNo ratings yet
- Mental Health Field Manual - CaliforniaDocument44 pagesMental Health Field Manual - CaliforniaTom RueNo ratings yet
- Effect of TelenursingDocument17 pagesEffect of Telenursingirma nur amaliaNo ratings yet
- ThesisDocument39 pagesThesisPolitic FeverNo ratings yet
- Mental Health During Covid-19 PandemicDocument15 pagesMental Health During Covid-19 PandemicLamiya SimranNo ratings yet
- Drunkorexia: An Emerging Trend in Young Adults: ObjectiveDocument4 pagesDrunkorexia: An Emerging Trend in Young Adults: ObjectiveIoana CristinaNo ratings yet
- Onlinetobacco Cessationeducation Tooptimize Standardsofpractice Forpsychiatric MentalhealthnursesDocument9 pagesOnlinetobacco Cessationeducation Tooptimize Standardsofpractice Forpsychiatric MentalhealthnursesThaís MouraNo ratings yet
- An Internet-Based Physical Activity Intervention To Improve QualityDocument11 pagesAn Internet-Based Physical Activity Intervention To Improve Qualityamber.callenaere.1No ratings yet
- The Prevalence of Smoking, Determinants and Chance of Psychological Problems Among Smokers in An Urban Community Housing Project in MalaysiaDocument9 pagesThe Prevalence of Smoking, Determinants and Chance of Psychological Problems Among Smokers in An Urban Community Housing Project in Malaysialailatul husnaNo ratings yet
- PHD Thesis On Drug AbuseDocument6 pagesPHD Thesis On Drug Abuseioqyqenbf100% (1)
- Electronic Cigarettes: A Primer For CliniciansDocument10 pagesElectronic Cigarettes: A Primer For Cliniciansgirish_s777No ratings yet
- SOCW 3004 Research ImplicationsDocument7 pagesSOCW 3004 Research ImplicationsTyler HemsworthNo ratings yet
- Impact of COVID-19 Pandemic On Mental Health in The General Population - A Systematic ReviewDocument36 pagesImpact of COVID-19 Pandemic On Mental Health in The General Population - A Systematic ReviewCharlesNo ratings yet
- Modafinil For Cognitive NeuroenhancementDocument35 pagesModafinil For Cognitive NeuroenhancementAImeé MontoyaNo ratings yet
- Literature Review AlcoholDocument6 pagesLiterature Review Alcoholfvf2j8q0100% (1)
- Literature Review On Alcohol DependenceDocument4 pagesLiterature Review On Alcohol Dependenceea3d6w9v100% (1)
- 4-8 Final Research Manuscript UpdateDocument29 pages4-8 Final Research Manuscript Updateapi-623462188No ratings yet
- Literature Review Medication Safety in AustraliaDocument5 pagesLiterature Review Medication Safety in Australiaea7gpeqm100% (1)
- The Relationship Between Depression and Internet AddictionDocument5 pagesThe Relationship Between Depression and Internet AddictionUki NaeroraNo ratings yet
- "Happy Feet": Evaluating The Benefits of A 100-Day 10,000 Step Challenge On Mental Health and WellbeingDocument7 pages"Happy Feet": Evaluating The Benefits of A 100-Day 10,000 Step Challenge On Mental Health and WellbeingANA CALDERONNo ratings yet
- Synthesis For Se 1Document10 pagesSynthesis For Se 1api-485620816No ratings yet
- Memorandum of Agreement For Work Immersion PartnershipDocument8 pagesMemorandum of Agreement For Work Immersion PartnershipBernadette AycochoNo ratings yet
- ASSEMBLY&DISASSEMBLYDocument12 pagesASSEMBLY&DISASSEMBLYBernadette AycochoNo ratings yet
- Data Measurement ChartDocument6 pagesData Measurement ChartBernadette AycochoNo ratings yet
- Work Immersion Performance Appraisal - FINALDocument3 pagesWork Immersion Performance Appraisal - FINALBernadette Aycocho100% (5)
- Recipe Book: (Noodles and Desserts)Document31 pagesRecipe Book: (Noodles and Desserts)Bernadette Aycocho100% (1)
- Master in Data Science: Course Descriptions Professional Courses: Financial ManagementDocument3 pagesMaster in Data Science: Course Descriptions Professional Courses: Financial ManagementBernadette AycochoNo ratings yet
- Fractions in Lowest TermDocument2 pagesFractions in Lowest TermBernadette AycochoNo ratings yet
- AsteroidsDocument1 pageAsteroidsBernadette AycochoNo ratings yet
- Para Sa NewspaperDocument1 pagePara Sa NewspaperBernadette AycochoNo ratings yet
- Meal Plan For The Whole Week: SundayDocument2 pagesMeal Plan For The Whole Week: SundayBernadette AycochoNo ratings yet
- Operating System Lab ActivityDocument2 pagesOperating System Lab ActivityBernadette AycochoNo ratings yet
- Software Engineering and Design Project Documentation Outline For Chapter 1Document6 pagesSoftware Engineering and Design Project Documentation Outline For Chapter 1Bernadette AycochoNo ratings yet
- Authors of The Manuscript: Darryl Owens and Mark Anderson Reported By: Bernadette A. Dela CruzDocument6 pagesAuthors of The Manuscript: Darryl Owens and Mark Anderson Reported By: Bernadette A. Dela CruzBernadette AycochoNo ratings yet
- Addressing The Increasing Number of Diabetic Patients Through The Application of Descriptive, Predictive and Prescriptive AnalysesDocument2 pagesAddressing The Increasing Number of Diabetic Patients Through The Application of Descriptive, Predictive and Prescriptive AnalysesBernadette AycochoNo ratings yet
- Alpine 7164 ModificationsDocument12 pagesAlpine 7164 ModificationsFede CX5AANo ratings yet
- 2g GSM Radio Capacity JuneDocument8 pages2g GSM Radio Capacity JuneVenkata RamanaNo ratings yet
- JioFiber Router Login - 192.168.1.1Document3 pagesJioFiber Router Login - 192.168.1.1mayakaaranNo ratings yet
- DVSR v1-5 EN-0906Document114 pagesDVSR v1-5 EN-0906Prana RajNo ratings yet
- AZ-GTI and ASI AIR Pro InstructionsDocument5 pagesAZ-GTI and ASI AIR Pro InstructionsLane LastNo ratings yet
- VT10 Protocol Document (SIM900) V103Document85 pagesVT10 Protocol Document (SIM900) V103Héctor Ivan Guerrero GuerreroNo ratings yet
- H80BCAME Board DatasheetDocument2 pagesH80BCAME Board Datasheetسعيد المعدنNo ratings yet
- IPD2220ES / LD2222E: 1080P HD Dome IP CameraDocument15 pagesIPD2220ES / LD2222E: 1080P HD Dome IP CameraMahmoud AhmedNo ratings yet
- Kptcl-Scada ReportDocument26 pagesKptcl-Scada ReportHarshith ANANDNo ratings yet
- Sorcerer Installation and OperationDocument22 pagesSorcerer Installation and OperationFilip FilipovicNo ratings yet
- HG8145V5 Quick Start For QR Code 01 (En, Mexico Megacable)Document15 pagesHG8145V5 Quick Start For QR Code 01 (En, Mexico Megacable)Esteban QuirozNo ratings yet
- Distance Learning MatrixDocument1 pageDistance Learning MatrixRuth PetrosNo ratings yet
- Hussien SaidDocument145 pagesHussien SaidbissibNo ratings yet
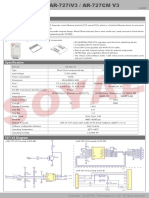
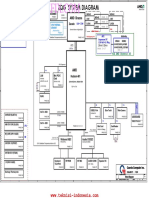
- AR-727iV3: Part NO. AR-727i V3 AR-727CM V3Document4 pagesAR-727iV3: Part NO. AR-727i V3 AR-727CM V3jorge franco HerreraNo ratings yet
- Experiment 4 PDFDocument9 pagesExperiment 4 PDFljjbNo ratings yet
- Na-A Julianto Wira MansaDocument5 pagesNa-A Julianto Wira MansawiraNo ratings yet
- Nov 23 RD Material Lice AgmDocument11 pagesNov 23 RD Material Lice AgmgamerkoteshchannelNo ratings yet
- Space Solutions: Aerospace and DefenseDocument20 pagesSpace Solutions: Aerospace and DefenseTarcisio Lima - Grupo AutcompNo ratings yet
- 508 V2 1 InstallationManualDocument544 pages508 V2 1 InstallationManualpankaj sharmaNo ratings yet
- Mukund Nikam Wireless Electricity..Document22 pagesMukund Nikam Wireless Electricity..mukund nikamNo ratings yet
- Acer 4253 - Zqe - ZQGDocument41 pagesAcer 4253 - Zqe - ZQGA Sufri ParaungiNo ratings yet
- Panasonic SC-PM18 Stereo System User ManualDocument28 pagesPanasonic SC-PM18 Stereo System User Manualdinosauro007No ratings yet
- MAPP XT - Project ReportDocument13 pagesMAPP XT - Project ReportAhonny LarpNo ratings yet
- 66e23833 LTN145AT01 H01Document4 pages66e23833 LTN145AT01 H01trattoriapizzeriapassioneNo ratings yet
- Identify These Applications ProgramDocument5 pagesIdentify These Applications ProgramRegil Tryadi AdhiwidjayaNo ratings yet
- Enki by Leroy Merlin Scales Up Smart Home Ecosystem Integration Thanks To MicroEJ SolutionsDocument3 pagesEnki by Leroy Merlin Scales Up Smart Home Ecosystem Integration Thanks To MicroEJ SolutionsPR.comNo ratings yet
- Opel Antara: Infotainment SystemDocument139 pagesOpel Antara: Infotainment SystemAndrei IonicaNo ratings yet
- X1N-H0401 Specification Q3Document12 pagesX1N-H0401 Specification Q3Waheed Uddin MohammedNo ratings yet
- Safety and Certifications: Important Information About The Sagemcom F@ST3486: Installation and Safe Usage InstructionsDocument4 pagesSafety and Certifications: Important Information About The Sagemcom F@ST3486: Installation and Safe Usage InstructionsRomina GuadagniniNo ratings yet
- Network Engineer Interview Questions and AnswersDocument11 pagesNetwork Engineer Interview Questions and AnswerssalahNo ratings yet