You might also like
- Clinical Bedside Swallowing AssessmentDocument7 pagesClinical Bedside Swallowing Assessmentlogoioannina100% (2)
- Taste of Herbs Flavor Wheel PacketDocument5 pagesTaste of Herbs Flavor Wheel PacketElma McGougan100% (2)
- Vocal Health HandoutDocument3 pagesVocal Health HandoutScott HamiltonNo ratings yet
- Chinese Foot Reflexology ChartsDocument1 pageChinese Foot Reflexology ChartsVelpandian ManiNo ratings yet
- Ebola: The Natural and Human History of A Deadly Virus (Norton, October 2014), by David QuammenDocument4 pagesEbola: The Natural and Human History of A Deadly Virus (Norton, October 2014), by David QuammenThe World50% (4)
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahNo ratings yet
- Case Report - Complete Denture - 2Document4 pagesCase Report - Complete Denture - 2Astri Ggamjong Xiao LuNo ratings yet
- Postural HypotensionDocument11 pagesPostural HypotensionMa Lyn GabayeronNo ratings yet
- Occlusion of Crown BridgeDocument39 pagesOcclusion of Crown BridgeRawzh Salih MuhammadNo ratings yet
- Assessment Diagnosis Rationale Expected Outcome Implementation Rationale EvaluationDocument5 pagesAssessment Diagnosis Rationale Expected Outcome Implementation Rationale EvaluationRazzel Daza100% (1)
- Report Sheets (Parasitology Lab)Document7 pagesReport Sheets (Parasitology Lab)billhaddNo ratings yet
- Materials, Chemicals and Methods for Dental ApplicationsFrom EverandMaterials, Chemicals and Methods for Dental ApplicationsNo ratings yet
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Hemiseksi Akar Distal Molar Kedua Rahang BawahDocument5 pagesHemiseksi Akar Distal Molar Kedua Rahang BawahAhmad Willy AntonNo ratings yet
- Maxillomandibular Relation (MMR)Document15 pagesMaxillomandibular Relation (MMR)Dea Intania DewiNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryFayiz SäbNo ratings yet
- Case Report Fissure SealantDocument8 pagesCase Report Fissure SealantrespikNo ratings yet
- FERGUSON John: Bibliotheca Chemica 1/2 (Voll.2) 1909 NO1954Document522 pagesFERGUSON John: Bibliotheca Chemica 1/2 (Voll.2) 1909 NO1954Acca Erma Settemonti100% (2)
- Preparasi Gigi AbutmentDocument15 pagesPreparasi Gigi AbutmentFransiskus Xaverius DoddieNo ratings yet
- 14 - Perawatan Endodontic Gigi Molar Dengan Perforasi BifurkasiDocument5 pages14 - Perawatan Endodontic Gigi Molar Dengan Perforasi Bifurkasisarah hanifahNo ratings yet
- Arch BarDocument28 pagesArch BarFachrul Latif DentistNo ratings yet
- SSCDocument10 pagesSSCYanuar MegaNo ratings yet
- Preventive Resin Restorations: Review ArticlesDocument5 pagesPreventive Resin Restorations: Review ArticlesFatma HandayaniNo ratings yet
- Curve of SpeeDocument7 pagesCurve of SpeeKorina CallerosNo ratings yet
- A Physiologic Impression Technique For Resorbed Mandibular Ridges PDFDocument3 pagesA Physiologic Impression Technique For Resorbed Mandibular Ridges PDFJyoti VermaNo ratings yet
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocument6 pagesClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaNo ratings yet
- Dense Bone Island: Temuan Insidental Pada Radiograf PanoramikDocument4 pagesDense Bone Island: Temuan Insidental Pada Radiograf PanoramikFransiski HoNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFZaenuriNo ratings yet
- Windowing: Mengatasi Akibat Pemakaian Gigitiruan Lama Dengan Pencetakan TeknikDocument12 pagesWindowing: Mengatasi Akibat Pemakaian Gigitiruan Lama Dengan Pencetakan TeknikSTEFFI MIFTANo ratings yet
- 1.1 Endodontik: HealingDocument52 pages1.1 Endodontik: HealingARINA KHAQ100% (1)
- Geriatri EndodontikDocument4 pagesGeriatri EndodontikMeidi KurniaNo ratings yet
- Guided Tissue RegenerationDocument4 pagesGuided Tissue RegenerationNicoleta MarcuNo ratings yet
- Coronoplasty 2Document4 pagesCoronoplasty 2Befalia Aisarahmadani100% (1)
- Hidden CariesDocument10 pagesHidden Cariesyenni_windasariNo ratings yet
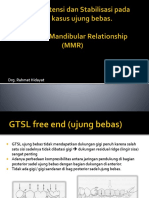
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 pagesDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarNo ratings yet
- Modified Bluegrass Appliance PDFDocument4 pagesModified Bluegrass Appliance PDFRenieKumalaNo ratings yet
- Jurnal Reading Bedah MulutDocument27 pagesJurnal Reading Bedah MulutArismunandar SosiloNo ratings yet
- Classification System For Full EdentulismDocument4 pagesClassification System For Full EdentulismmandakinimohanNo ratings yet
- Compomer CrownDocument2 pagesCompomer CrownIndah SimamoraNo ratings yet
- 40 130 1 PBDocument4 pages40 130 1 PBrinaaa2000No ratings yet
- Clinical Evaluation Between Zirconia Crowns and Stainless Steel Crowns in Primary Molars TeethDocument7 pagesClinical Evaluation Between Zirconia Crowns and Stainless Steel Crowns in Primary Molars TeethninisskyNo ratings yet
- Occlusal Adjustment Through Selective Grinding and SplintingDocument4 pagesOcclusal Adjustment Through Selective Grinding and SplintingAlex DogaruNo ratings yet
- Keilitis Eksfoliatif JurnalDocument8 pagesKeilitis Eksfoliatif JurnalIbnu MuttaqinNo ratings yet
- Terdapat Hubungan Keparahan Resesi Gingiva Terhadap Tingkat Usia Dan Macam GigiDocument5 pagesTerdapat Hubungan Keparahan Resesi Gingiva Terhadap Tingkat Usia Dan Macam GigiDevi AlfianiNo ratings yet
- Bagi '18211 - Scenario in Englis3.docx'Document6 pagesBagi '18211 - Scenario in Englis3.docx'ithanur316No ratings yet
- SialodenosisDocument76 pagesSialodenosisJessica GreenNo ratings yet
- Tes TLMDocument16 pagesTes TLMAmelia RosyidaNo ratings yet
- IckDocument6 pagesIckbkprosthoNo ratings yet
- 2019 Risk Factors For Caries Development in Primary Sjogren SyndromeDocument6 pages2019 Risk Factors For Caries Development in Primary Sjogren SyndromemrsilNo ratings yet
- Space Maintainer - A ReviewDocument5 pagesSpace Maintainer - A ReviewHabeeb AL-AbsiNo ratings yet
- Adhesive BridgesDocument9 pagesAdhesive BridgesShilpa ShrivastavaNo ratings yet
- Management of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryDocument4 pagesManagement of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryLatifa Hanif ZuhriNo ratings yet
- Identifikasi Bakteri Dental Plak Melalui Morfologi Koloni Dan PengecatanDocument19 pagesIdentifikasi Bakteri Dental Plak Melalui Morfologi Koloni Dan PengecatanfadilazahraNo ratings yet
- Predictable Diastema Closure Using An Innovative Indirect Mock Up TechniqueDocument4 pagesPredictable Diastema Closure Using An Innovative Indirect Mock Up TechniqueJane JaneeNo ratings yet
- Acc Pain FauziDocument8 pagesAcc Pain FauziMuchlis Fauzi ENo ratings yet
- Mono BlockDocument4 pagesMono BlockSiti Utami DewiNo ratings yet
- Enteriditis, Streptococcus Mutans. The Names ofDocument4 pagesEnteriditis, Streptococcus Mutans. The Names ofdianaNo ratings yet
- Cara Penggunaaan DevitalDocument2 pagesCara Penggunaaan DevitalKrisbudiSetyawanNo ratings yet
- CBL English Blok 7Document7 pagesCBL English Blok 7Ifata RDNo ratings yet
- Kuliah Glass Ionomer CementDocument40 pagesKuliah Glass Ionomer CementMaika RatriNo ratings yet
- Gambaran Radiografi Oklusa Kista DentigerousDocument6 pagesGambaran Radiografi Oklusa Kista DentigerousErlin ZukeNo ratings yet
- Orthodontic Treatment Needs in Adolescents Aged 13-15 Years Using Orthodontic Treatment Needs IndicatorsDocument7 pagesOrthodontic Treatment Needs in Adolescents Aged 13-15 Years Using Orthodontic Treatment Needs IndicatorsTitis NlgNo ratings yet
- Asds 06 1452Document9 pagesAsds 06 1452medicalrecords211No ratings yet
- Computerized Occlusal Analysis As An Alternative Occlusal IndicatorDocument6 pagesComputerized Occlusal Analysis As An Alternative Occlusal IndicatorMariana RaduNo ratings yet
- Pintado 2000Document8 pagesPintado 2000vicentejerezgonNo ratings yet
- 1 s2.0 S2210261221004363 MainDocument7 pages1 s2.0 S2210261221004363 MainFlávia de Souza BastosNo ratings yet
- Importance of A Stable Maxillomandibular Relation PDFDocument11 pagesImportance of A Stable Maxillomandibular Relation PDFOsvaldo OsunaNo ratings yet
- Jadwal Praktek DRG Per Januari 2021 FixDocument39 pagesJadwal Praktek DRG Per Januari 2021 FixKhaleda ShafiraNo ratings yet
- The Use of A Removable Orthodontic Appliance For Space Management Combined With Anterior Esthetic Restorations: A Case ReportDocument11 pagesThe Use of A Removable Orthodontic Appliance For Space Management Combined With Anterior Esthetic Restorations: A Case ReportKhaleda ShafiraNo ratings yet
- Jurnal Rmgic IIDocument7 pagesJurnal Rmgic IIKhaleda ShafiraNo ratings yet
- Dentalarticle PDFDocument9 pagesDentalarticle PDFKhaleda ShafiraNo ratings yet
- Rotational Versus ConventionalDocument7 pagesRotational Versus ConventionalKhaleda ShafiraNo ratings yet
- Jurnal MucoceleDocument6 pagesJurnal MucoceleKhaleda ShafiraNo ratings yet
- Journal Reading Reversible ProtectionDocument20 pagesJournal Reading Reversible ProtectionKhaleda ShafiraNo ratings yet
- Mucocele JurnalDocument6 pagesMucocele JurnalKhaleda ShafiraNo ratings yet
- Stabilization Splint (Night Guard, Mouth Guard) Comparative Research MDJDocument5 pagesStabilization Splint (Night Guard, Mouth Guard) Comparative Research MDJKhaleda ShafiraNo ratings yet
- Skenario 1 Blok 11Document5 pagesSkenario 1 Blok 11Khaleda ShafiraNo ratings yet
- Analisis Dimensi Kualitas Pelayanan Terhadap Kepuasan Pelanggan Pada Laboratorium Parahita Diagnostic Center Cabang Jember Akhmad SuhartoDocument9 pagesAnalisis Dimensi Kualitas Pelayanan Terhadap Kepuasan Pelanggan Pada Laboratorium Parahita Diagnostic Center Cabang Jember Akhmad SuhartoKhaleda ShafiraNo ratings yet
- Recurrent Sprain OF: THE WithDocument4 pagesRecurrent Sprain OF: THE WithKhaleda ShafiraNo ratings yet
- Osce EmergenciesjDocument31 pagesOsce EmergenciesjTess WilliamsNo ratings yet
- Hip Arthroplasty GAP Analysis and CI StudyDocument6 pagesHip Arthroplasty GAP Analysis and CI StudyHarrison HayesNo ratings yet
- Good and Bad Thesis Statements ExerciseDocument3 pagesGood and Bad Thesis Statements ExerciseBillyNo ratings yet
- Medication20quizzes 12028429Document2 pagesMedication20quizzes 12028429DurgaNadellaNo ratings yet
- Asian MS Newsletter Issue 1, 2014Document16 pagesAsian MS Newsletter Issue 1, 2014AsianMS_SupportGroupNo ratings yet
- List Provider - Great Eastern 2018Document60 pagesList Provider - Great Eastern 2018wawanknNo ratings yet
- Jurnal Acute Decompensated Heart FailureDocument4 pagesJurnal Acute Decompensated Heart FailureMayang Sri WulandNo ratings yet
- CASE PRESENTATION ON U AnginaDocument40 pagesCASE PRESENTATION ON U AnginaSafoora RafeeqNo ratings yet
- Principles or Elements If Effective DocumentationDocument9 pagesPrinciples or Elements If Effective DocumentationHoney Bitas OriasNo ratings yet
- Sri Ramachandra University Application-09Document5 pagesSri Ramachandra University Application-09Mohammed RaziNo ratings yet
- Internship Report On SearleDocument28 pagesInternship Report On Searlemadiha_madihaNo ratings yet
- Injuries To Neck Structures in Deaths Due To Constriction of Neck, With A Special Reference To HangingDocument8 pagesInjuries To Neck Structures in Deaths Due To Constriction of Neck, With A Special Reference To Hangingemmanueltobon0621No ratings yet
- Sds Disability Scale InformationDocument2 pagesSds Disability Scale InformationcarolineNo ratings yet
- Panchakarma Power (Autosaved)Document24 pagesPanchakarma Power (Autosaved)drkimi ralte2No ratings yet
- Chapter - 1: Ayurvedic Subhasitas in Sanskrit Literature, Is A New Field inDocument46 pagesChapter - 1: Ayurvedic Subhasitas in Sanskrit Literature, Is A New Field inIniNo ratings yet
- Mark Rwigamba: Career ObjectiveDocument2 pagesMark Rwigamba: Career Objectiveapi-314188365No ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document86 pagesChronic Obstructive Pulmonary Disease (COPD)physio43No ratings yet
- Creatinine DogDocument18 pagesCreatinine DogLuis Antonio Buitron RamirezNo ratings yet
- The Voice of The Anahata Chakra: "I Love" "I Am Lovable " "I Am Completely Loved"Document3 pagesThe Voice of The Anahata Chakra: "I Love" "I Am Lovable " "I Am Completely Loved"SouravNo ratings yet
- Mobil Jet Oil IIDocument8 pagesMobil Jet Oil IIJerome Cardenas TablacNo ratings yet