You might also like
- UntitledDocument41 pagesUntitledDion AdalaNo ratings yet
- Birthday QuotesDocument24 pagesBirthday QuotesArniel CatubigNo ratings yet
- Fundamentals of Designing Relative Strength ProgramsDocument35 pagesFundamentals of Designing Relative Strength ProgramsFlorian WolfNo ratings yet
- Lesson Plan Personality DisorderDocument7 pagesLesson Plan Personality DisorderRaj MeghwalNo ratings yet
- IWGIA Book The Indigenous World 2021 ENGDocument824 pagesIWGIA Book The Indigenous World 2021 ENGREy FOxNo ratings yet
- PFI Freediver ManualDocument69 pagesPFI Freediver ManualLuca MariniNo ratings yet
- Nasoalveolar Moulding Seminar at MalakkaraDocument54 pagesNasoalveolar Moulding Seminar at MalakkaraAshwin100% (1)
- Ranitidine + OndansetronDocument7 pagesRanitidine + OndansetronAllicia PutriNo ratings yet
- 1-A Colored Substance That Is Spread Over A Surface and Dries To Leave A Thin Decorative or Protective Coating. Decorative or Protective CoatingDocument60 pages1-A Colored Substance That Is Spread Over A Surface and Dries To Leave A Thin Decorative or Protective Coating. Decorative or Protective Coatingjoselito lacuarinNo ratings yet
- Midterm and Final Exam TFNDocument6 pagesMidterm and Final Exam TFNalchriwNo ratings yet
- Vital Signs Monitoring System For Patients.: Universidad Politécnica Salesiana Cuenca - Ecuador AbstractDocument12 pagesVital Signs Monitoring System For Patients.: Universidad Politécnica Salesiana Cuenca - Ecuador AbstractFreddy Valdez GarciaNo ratings yet
- 1 s2.0 S0165168413004696 MainDocument10 pages1 s2.0 S0165168413004696 MainkhaledNo ratings yet
- A Fully-Asynchronous Low-Power Implantable Seizure Detector For Self-Triggering TreatmentDocument10 pagesA Fully-Asynchronous Low-Power Implantable Seizure Detector For Self-Triggering TreatmentshalvinNo ratings yet
- Adaptive Single-Channel EEG Artifact Removal With Applications To Clinical MonitoringDocument10 pagesAdaptive Single-Channel EEG Artifact Removal With Applications To Clinical MonitoringmuraliNo ratings yet
- Peng 2013Document8 pagesPeng 2013Dhanalekshmi YedurkarNo ratings yet
- EEG Signal Analysis and Characterization For The Aid of Disabled PeopleDocument8 pagesEEG Signal Analysis and Characterization For The Aid of Disabled PeopleShafayet UddinNo ratings yet
- TD AlbertoLopezMartinez PDFDocument286 pagesTD AlbertoLopezMartinez PDFCarlos Manuel Carranza VegaNo ratings yet
- EEG Artifact Removal-State-Of-The-Art and GuidelinesDocument24 pagesEEG Artifact Removal-State-Of-The-Art and GuidelinesYuanXin SuNo ratings yet
- DWT Kalnab 2016Document8 pagesDWT Kalnab 2016Nahidul IslamNo ratings yet
- ICASSP10Document5 pagesICASSP10Showkat RashidNo ratings yet
- Materials, Devices, and Systems of On-Skin Electrodes For Electrophysiological Monitoring and Human-Machine InterfacesDocument30 pagesMaterials, Devices, and Systems of On-Skin Electrodes For Electrophysiological Monitoring and Human-Machine InterfacesRendy PutraaaNo ratings yet
- JournalNX - Wavelet FunctionDocument3 pagesJournalNX - Wavelet FunctionJournalNX - a Multidisciplinary Peer Reviewed JournalNo ratings yet
- Signals 03 00035Document10 pagesSignals 03 00035Gilbert SihombingNo ratings yet
- 2021 10 19 21265197v1 FullDocument10 pages2021 10 19 21265197v1 FullmuraliNo ratings yet
- Body Electric: FO CU SE D Ue Fe AT UR EDocument11 pagesBody Electric: FO CU SE D Ue Fe AT UR EHarold RodriguezNo ratings yet
- Epileptic Seizure Prediction Based On Features Extracted Using Wavelet Decomposition and Linear Prediction FilterDocument6 pagesEpileptic Seizure Prediction Based On Features Extracted Using Wavelet Decomposition and Linear Prediction FilterTucha KedirNo ratings yet
- AttentivU A Wearable Pair of EEG and EOGDocument4 pagesAttentivU A Wearable Pair of EEG and EOGPriya ManojNo ratings yet
- Artgo FernandaDocument12 pagesArtgo FernandaEduardo Clasen BackNo ratings yet
- A NoveEOG L Topology For Design and Development of Wireless Electro Oculogram Biopotential AmpliferDocument6 pagesA NoveEOG L Topology For Design and Development of Wireless Electro Oculogram Biopotential AmpliferAbhinav GuptaNo ratings yet
- Arm and Wrist Surface Potential Mapping For Wearable ECG Rhythm Recording Devices A PilotDocument9 pagesArm and Wrist Surface Potential Mapping For Wearable ECG Rhythm Recording Devices A PilotKarthik Raj VNo ratings yet
- Kilicarslan Et Al HinfDocument17 pagesKilicarslan Et Al HinfMansoor MughalNo ratings yet
- Development and Evaluation of Multilead PDFDocument10 pagesDevelopment and Evaluation of Multilead PDFfelixsafar3243No ratings yet
- BECT Spike Detection Based On Novel EEG Sequence Features and LSTM AlgorithmsDocument10 pagesBECT Spike Detection Based On Novel EEG Sequence Features and LSTM AlgorithmsatewogboNo ratings yet
- Faster JNMDocument31 pagesFaster JNMmuraliNo ratings yet
- Electroretinography (A Review) Balicka, A., Trbolová, A., Vrbovská, TDocument6 pagesElectroretinography (A Review) Balicka, A., Trbolová, A., Vrbovská, TNisa TaslimNo ratings yet
- 1 PDFDocument11 pages1 PDFZoltan NadasdyNo ratings yet
- ElectrooculographyDocument66 pagesElectrooculographyDhinesh_90100% (2)
- Red Ocular Artifact Hi-Dimen Neural Data WangDocument9 pagesRed Ocular Artifact Hi-Dimen Neural Data WangAlex WongNo ratings yet
- QWEEDocument8 pagesQWEEJackyNo ratings yet
- Brain-Computer Interface (Bci)Document16 pagesBrain-Computer Interface (Bci)Amal Raj ANo ratings yet
- Erg Final PDFDocument17 pagesErg Final PDFKarthigaMurugesanNo ratings yet
- Driver Drowsiness Classification Using Fuzzy Wavelet-Packet-Based Feature-Extraction AlgorithmDocument11 pagesDriver Drowsiness Classification Using Fuzzy Wavelet-Packet-Based Feature-Extraction AlgorithmAlex WongNo ratings yet
- Eog FINAL PDFDocument18 pagesEog FINAL PDFKarthigaMurugesanNo ratings yet
- A Novel Signal Modeling Approach For Classification of Seizure and Seizure-Free EEG SignalsDocument11 pagesA Novel Signal Modeling Approach For Classification of Seizure and Seizure-Free EEG Signalssatyender jaglanNo ratings yet
- Einthovens Triangle Transparency - A Practical Method To Explain Limb LeadDocument23 pagesEinthovens Triangle Transparency - A Practical Method To Explain Limb LeadAishwarya SrinivasanNo ratings yet
- CCCCCCCCCCCCCCCCCCCCCC C C CDocument42 pagesCCCCCCCCCCCCCCCCCCCCCC C C CJoseph ReddyNo ratings yet
- Epileptic Siezure Onset Detection Based On EEG and ECG Data FusionDocument13 pagesEpileptic Siezure Onset Detection Based On EEG and ECG Data FusionSana UllahNo ratings yet
- Removing Electroencephalographic Artifacts by Blind Source Separation 2000-3397Document16 pagesRemoving Electroencephalographic Artifacts by Blind Source Separation 2000-3397Benazir BegamNo ratings yet
- Fnins 13 00804Document16 pagesFnins 13 00804maryambashir4306No ratings yet
- Tinku Biswas, Swarup Sarkar, Akash Ku. Bhoi, Surajit BagchiDocument7 pagesTinku Biswas, Swarup Sarkar, Akash Ku. Bhoi, Surajit BagchiInternational Journal of computational Engineering research (IJCER)No ratings yet
- Detection of EMG Signals by Neural Networks Using Autoregression and Wavelet Entropy For Bruxism DiagnosisDocument11 pagesDetection of EMG Signals by Neural Networks Using Autoregression and Wavelet Entropy For Bruxism DiagnosisMuhammad Fauzi D4 ElektromedikNo ratings yet
- EogDocument16 pagesEogchoppersureNo ratings yet
- Zhang2016 PDFDocument14 pagesZhang2016 PDFRubén CallataNo ratings yet
- An Electrical Insulator Defects Detection Method CDocument10 pagesAn Electrical Insulator Defects Detection Method Cpapuq solehNo ratings yet
- Journal 1 IJEECS Scopus PublishedDocument10 pagesJournal 1 IJEECS Scopus PublishedDigambar PuriNo ratings yet
- On The Measurement of Electrical Impedance Spectroscopy (EIS) of The Human HeadDocument15 pagesOn The Measurement of Electrical Impedance Spectroscopy (EIS) of The Human HeadgpaivNo ratings yet
- A Portable Wireless Eye Movement-Controlled Human-Computer Interface For TheDocument5 pagesA Portable Wireless Eye Movement-Controlled Human-Computer Interface For TheSAADSURNo ratings yet
- Applied SciencesDocument21 pagesApplied SciencesEduard-Marius LungulescuNo ratings yet
- 2010 - IEEE Rev Biomed - Analog Integrated Circuits Design For Processing Physiological SignalsDocument13 pages2010 - IEEE Rev Biomed - Analog Integrated Circuits Design For Processing Physiological SignalsSifat -Ul-AlamNo ratings yet
- Automatic Detection of Seizure ONSET in Pediatric EEGDocument9 pagesAutomatic Detection of Seizure ONSET in Pediatric EEGijesajournalNo ratings yet
- Eog-Based Signal Detection and Verification For HciDocument7 pagesEog-Based Signal Detection and Verification For HciAbhinav GuptaNo ratings yet
- Conception and Development of A Tele-Medical Interface Dedicated To Tele Monitoring of The Renal and CardiacinsufficiencyDocument10 pagesConception and Development of A Tele-Medical Interface Dedicated To Tele Monitoring of The Renal and CardiacinsufficiencyInternational Journal of Engineering Inventions (IJEI)No ratings yet
- Electronics 07 00077 v31Document23 pagesElectronics 07 00077 v31MárciaNo ratings yet
- Meng 2022 J. Opt. 24 054004Document8 pagesMeng 2022 J. Opt. 24 054004Ozan KarNo ratings yet
- Expert Systems With Applications: Semih Altunay, Ziya Telatar, Osman ErogulDocument5 pagesExpert Systems With Applications: Semih Altunay, Ziya Telatar, Osman ErogulViswanath ReddyNo ratings yet
- MOAD TemplateDocument12 pagesMOAD TemplateHadj Abdelkader BENGHENIANo ratings yet
- Analysis of Epilepsy Using Approximate Entropy AlgorithmDocument5 pagesAnalysis of Epilepsy Using Approximate Entropy Algorithmanon_287269697No ratings yet
- Alzheimers Disease Patients Classification Through EEG Signals ProcessingDocument8 pagesAlzheimers Disease Patients Classification Through EEG Signals ProcessingIoana GuțăNo ratings yet
- Electrical Impedance TomographyDocument8 pagesElectrical Impedance TomographyAman KumarNo ratings yet
- OCT Imaging in Glaucoma: A guide for practitionersFrom EverandOCT Imaging in Glaucoma: A guide for practitionersKi Ho ParkNo ratings yet
- Capacitive: Laboratory-On-Chip ApplicationsDocument4 pagesCapacitive: Laboratory-On-Chip ApplicationsAlex WongNo ratings yet
- Charge-Based Capacitive Sensor Array For CMOS-Based Laboratory-on-Chip ApplicationsDocument8 pagesCharge-Based Capacitive Sensor Array For CMOS-Based Laboratory-on-Chip ApplicationsAlex WongNo ratings yet
- An On-Chip, Interconnect Capacitance Characterization Method With Sub-Femto-Farad ResolutionDocument7 pagesAn On-Chip, Interconnect Capacitance Characterization Method With Sub-Femto-Farad ResolutionAlex WongNo ratings yet
- High Accuracy Differential Capacitive Circuit For Bioparticles Sensing ApplicationsDocument4 pagesHigh Accuracy Differential Capacitive Circuit For Bioparticles Sensing ApplicationsAlex WongNo ratings yet
- Charge-Based Capacitive Sensor Array For CMOS-Based Laboratory-on-Chip ApplicationsDocument8 pagesCharge-Based Capacitive Sensor Array For CMOS-Based Laboratory-on-Chip ApplicationsAlex WongNo ratings yet
- A Hybrid Microfluidic/CMOS Capacitive Sensor Dedicated To Lab-on-Chip ApplicationsDocument8 pagesA Hybrid Microfluidic/CMOS Capacitive Sensor Dedicated To Lab-on-Chip ApplicationsAlex WongNo ratings yet
- Y9. DataHandlingCheckoutDocument5 pagesY9. DataHandlingCheckoutAlex WongNo ratings yet
- Novel Direct-Write CMOS-based Laboratory-On-Chip: Design, Assembly and Experimental ResultsDocument10 pagesNovel Direct-Write CMOS-based Laboratory-On-Chip: Design, Assembly and Experimental ResultsAlex WongNo ratings yet
- Ultra Low Capacitance Measurements in Multilevel Metallisation CMOS by Using Built-In Electron-MeterDocument4 pagesUltra Low Capacitance Measurements in Multilevel Metallisation CMOS by Using Built-In Electron-MeterAlex WongNo ratings yet
- A Noise-Shaping Accelerometer Interface Circuit For Two-Chip ImplementationDocument4 pagesA Noise-Shaping Accelerometer Interface Circuit For Two-Chip ImplementationAlex WongNo ratings yet
- An On-Chip, Attofarad Interconnect Charge-Based Capacitance Measurement (CBCM) TechniqueDocument4 pagesAn On-Chip, Attofarad Interconnect Charge-Based Capacitance Measurement (CBCM) TechniqueAlex WongNo ratings yet
- The Wes 2006 FreqDocument9 pagesThe Wes 2006 FreqAlex WongNo ratings yet
- An On-Chip, Interconnect Capacitance Characterization Method With Sub-Femto-Farad ResolutionDocument7 pagesAn On-Chip, Interconnect Capacitance Characterization Method With Sub-Femto-Farad ResolutionAlex WongNo ratings yet
- Cmos Circuits For On-Chip Capacitance Ratio Testing or Sensor ReadoutDocument4 pagesCmos Circuits For On-Chip Capacitance Ratio Testing or Sensor ReadoutAlex WongNo ratings yet
- Sylvester 2Document5 pagesSylvester 2Alex WongNo ratings yet
- Sylvester 2Document5 pagesSylvester 2Alex WongNo ratings yet
- Detection of Vesicular Stomatitis Virus Using A Capacitive ImmunosensorDocument4 pagesDetection of Vesicular Stomatitis Virus Using A Capacitive ImmunosensorAlex WongNo ratings yet
- Use of Test Structures For Characterization and Modeling of Inter-And Intra-Layer Capacitances in A CMOS ProcessDocument9 pagesUse of Test Structures For Characterization and Modeling of Inter-And Intra-Layer Capacitances in A CMOS ProcessAlex WongNo ratings yet
- Cochlear Function in Mice With Only One Copy of The Prestin GeneDocument13 pagesCochlear Function in Mice With Only One Copy of The Prestin GeneAlex WongNo ratings yet
- The Wes 2007Document9 pagesThe Wes 2007Alex WongNo ratings yet
- Monolayers: Voltage-Dependent Capacitance in Lipid Bilayers FromDocument17 pagesMonolayers: Voltage-Dependent Capacitance in Lipid Bilayers FromAlex WongNo ratings yet
- The C-Terminus of Prestin Influences Nonlinear Capacitance and Plasma Membrane TargetingDocument10 pagesThe C-Terminus of Prestin Influences Nonlinear Capacitance and Plasma Membrane TargetingAlex WongNo ratings yet
- Var Cap MeasureDocument5 pagesVar Cap MeasureAlex WongNo ratings yet
- Noise Analysis and Characterization of A Sigma-Delta Capacitive MicroaccelerometerDocument10 pagesNoise Analysis and Characterization of A Sigma-Delta Capacitive MicroaccelerometerAlex WongNo ratings yet
- 12.4 Capacitive Sensor Array For Localization of Bioparticles in CMOS Lab-on-a-ChipDocument8 pages12.4 Capacitive Sensor Array For Localization of Bioparticles in CMOS Lab-on-a-ChipAlex WongNo ratings yet
- Mido AsadaDocument7 pagesMido AsadaAlex WongNo ratings yet
- A Fully Differential Rail-to-Rail Capacitance Measurement Circuit For Integrated Cell SensingDocument4 pagesA Fully Differential Rail-to-Rail Capacitance Measurement Circuit For Integrated Cell SensingAlex WongNo ratings yet
- A New Test Structure For Interconnect Capacitance MonitoringDocument4 pagesA New Test Structure For Interconnect Capacitance MonitoringAlex WongNo ratings yet
- Ultra Low Capacitance Measurements in Multilevel Metallisation CMOS by Using Built-In Electron-MeterDocument4 pagesUltra Low Capacitance Measurements in Multilevel Metallisation CMOS by Using Built-In Electron-MeterAlex WongNo ratings yet
- A Microfabricated Biosensor For Detecting Foodborne Bioterrorism AgentsDocument7 pagesA Microfabricated Biosensor For Detecting Foodborne Bioterrorism AgentsAlex WongNo ratings yet
- The Three Modern Relationship Models and Why They Are All FlawedDocument5 pagesThe Three Modern Relationship Models and Why They Are All FlawedBingoNo ratings yet
- Logiq e BT11 User Guide PDFDocument192 pagesLogiq e BT11 User Guide PDFprofesorbartolomeo0% (1)
- Shabeer Et Al-2018-Journal of PerinatologyDocument8 pagesShabeer Et Al-2018-Journal of PerinatologyrenataNo ratings yet
- Master of International HealthDocument5 pagesMaster of International HealthJesper Domincil BayauaNo ratings yet
- LinkageDocument47 pagesLinkageTony BernardNo ratings yet
- Evolve Reach - Powered by HESIDocument7 pagesEvolve Reach - Powered by HESIangelsarerare14% (7)
- Aerobic ActivitiesExercises PDFDocument14 pagesAerobic ActivitiesExercises PDFPalma, Arrabela M.No ratings yet
- 3RD Summative Exam in Science 6Document6 pages3RD Summative Exam in Science 6Maricris Palermo SancioNo ratings yet
- Material Data Sheet Durapro Asa: DescriptionDocument1 pageMaterial Data Sheet Durapro Asa: DescriptionAlexandru NeacsuNo ratings yet
- Name of Learner: Section: Subject Teacher: Date:: Practical Research 2Document4 pagesName of Learner: Section: Subject Teacher: Date:: Practical Research 2J-heart Basabas Malpal100% (6)
- Allosteric Regulation & Covalent ModificationDocument10 pagesAllosteric Regulation & Covalent ModificationBhaskar Ganguly100% (1)
- Operations Manual: Conical Burr Coffee GrinderDocument15 pagesOperations Manual: Conical Burr Coffee Grindercherrera73No ratings yet
- Princess Joy Placement and General Services vs. BinallaDocument2 pagesPrincess Joy Placement and General Services vs. Binallaapple_doctoleroNo ratings yet
- Social Science Assignment Class 8 CBSEDocument3 pagesSocial Science Assignment Class 8 CBSEgurdeepsarora8738No ratings yet
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- Cord Care Evaluation ToolDocument1 pageCord Care Evaluation ToolCherry AnnNo ratings yet
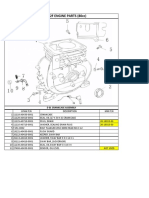
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- My Project PresentationDocument12 pagesMy Project Presentationkarunasand15No ratings yet
- 1often Wonder About My Future As I Am About To Finish Secondary SchoolDocument2 pages1often Wonder About My Future As I Am About To Finish Secondary SchoolMidz Santayana100% (1)
- ISO 9001 - 14001 - 2015 enDocument2 pagesISO 9001 - 14001 - 2015 enVĂN THÀNH TRƯƠNGNo ratings yet