You might also like
- Transducer Frequency - 205/305/5.0 MHZ: DR Satish Kumar Sharma Consultant CardiologistDocument1 pageTransducer Frequency - 205/305/5.0 MHZ: DR Satish Kumar Sharma Consultant CardiologistHappyNo ratings yet
- Patient Information: NCV (M/S)Document5 pagesPatient Information: NCV (M/S)ApriliaNo ratings yet
- 010424 Leeyoona NurmaulidyaDocument1 page010424 Leeyoona Nurmaulidyasigop25081993No ratings yet
- GurpreetDocument5 pagesGurpreetJoel AlexNo ratings yet
- 2016 UMEM ECG CompetitionDocument7 pages2016 UMEM ECG CompetitionCatherine MorrisNo ratings yet
- Gopal LalDocument2 pagesGopal LalPriyansh TanejaNo ratings yet
- Zara ReportsDocument13 pagesZara ReportsMuskanNo ratings yet
- Sample Emg/Ncv Report - Normal StudyDocument5 pagesSample Emg/Ncv Report - Normal StudyPhysiotherapist AliNo ratings yet
- I-Care Health Management & TPA Services Pvt. Ltd. Provider Tariff Provider Name: Section 1: Package RatesDocument4 pagesI-Care Health Management & TPA Services Pvt. Ltd. Provider Tariff Provider Name: Section 1: Package RatessakthiannamalaiNo ratings yet
- Anon ECHODocument3 pagesAnon ECHOMubasher UllahNo ratings yet
- Echo 20190914164646458Document2 pagesEcho 20190914164646458Gigi DajoyagNo ratings yet
- Gun 2Document1 pageGun 2M Fadli FahdurohmanNo ratings yet
- Mrs_Neha_Nandeshwar_11_09_2023_06_16_07_PMDocument2 pagesMrs_Neha_Nandeshwar_11_09_2023_06_16_07_PMdsz8wkvn4fNo ratings yet
- 010424 Alzhea MeghiDocument1 page010424 Alzhea Meghisigop25081993No ratings yet
- Ifu Splendor XDocument15 pagesIfu Splendor Xmedhat fathy100% (1)
- Lelly Muridi Zham Zham - Rep - OBDocument4 pagesLelly Muridi Zham Zham - Rep - OBPutera BrahmansaNo ratings yet
- L89 - Ypl Diagnostics Ypl Diagnosticssamrat Hopping Mall, Garh Road, Pin Code No: 252002meerut Uttar MeerutDocument3 pagesL89 - Ypl Diagnostics Ypl Diagnosticssamrat Hopping Mall, Garh Road, Pin Code No: 252002meerut Uttar MeerutAyush Kumar GuptaNo ratings yet
- BL ModerateDocument3 pagesBL ModerateResearch psychologistsNo ratings yet
- Lab Report 2 - Nerve Conduction Draft - Version 2Document8 pagesLab Report 2 - Nerve Conduction Draft - Version 2103304569No ratings yet
- DIAZ PASTOR, MARIA RAFAELA 07-06-2020 18-23-48 Full Report With Sentence GenDocument4 pagesDIAZ PASTOR, MARIA RAFAELA 07-06-2020 18-23-48 Full Report With Sentence Genangelica betancourtNo ratings yet
- 020424 Dea FitrianiDocument2 pages020424 Dea Fitrianisigop25081993No ratings yet
- Paciente: Juan Iorio Romero Fecha Nac: Medico Sexo: Talla: Medico Ref C.C: Peso: Técnico Historia ClinicaDocument4 pagesPaciente: Juan Iorio Romero Fecha Nac: Medico Sexo: Talla: Medico Ref C.C: Peso: Técnico Historia ClinicasorsoleyNo ratings yet
- INTRODocument20 pagesINTROdhruv kathuriaNo ratings yet
- Section: 1. Submitter's IdentilficationsDocument8 pagesSection: 1. Submitter's IdentilficationsLevi LeungNo ratings yet
- Cardiology Investigation Echo Doppler (2D Echo) EchocardiographyDocument2 pagesCardiology Investigation Echo Doppler (2D Echo) EchocardiographyManohar Kumar100% (2)
- S14 - Lpl-Ghaziabad C-30, RDC, Near Krishna Sagar, Rajnagar, Ghaziabad, U.P. GhaziabadDocument2 pagesS14 - Lpl-Ghaziabad C-30, RDC, Near Krishna Sagar, Rajnagar, Ghaziabad, U.P. GhaziabadVarunNo ratings yet
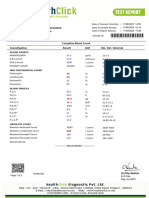
- Complete Blood Count and Dengue Test ResultsDocument4 pagesComplete Blood Count and Dengue Test ResultsThaneswar beheraNo ratings yet
- 8, Identitas Pasien SoapDocument10 pages8, Identitas Pasien SoapsunarsihNo ratings yet
- Huda 2010Document7 pagesHuda 2010Roshi_11No ratings yet
- Acc/Aha GuidelinesDocument63 pagesAcc/Aha GuidelinesPNVRSNo ratings yet
- Reed 1999 116 1 by OrTHoTaMiNe PDFDocument10 pagesReed 1999 116 1 by OrTHoTaMiNe PDFSankhyaNo ratings yet
- Shanae J DownerDocument2 pagesShanae J Downerapi-367795334No ratings yet
- 3lfng0szisu2rzbamlkul2a2Document12 pages3lfng0szisu2rzbamlkul2a2Bang ManNo ratings yet
- Clinical Evidence + ReferencesDocument313 pagesClinical Evidence + ReferencesPT Kimia Farma T&DNo ratings yet
- Word Dari PDFDocument7 pagesWord Dari PDFnskhldNo ratings yet
- ECOCARDIODocument3 pagesECOCARDIOArun ComedsNo ratings yet
- Date 02/jun/2023 09:05AM 20/mar/23 10:15AM 12/jan/23 02:47PM 12/nov/22 08:55AM 15/jul/21 02:18PM Unit Bio Ref IntervalDocument9 pagesDate 02/jun/2023 09:05AM 20/mar/23 10:15AM 12/jan/23 02:47PM 12/nov/22 08:55AM 15/jul/21 02:18PM Unit Bio Ref IntervalRemit DadhwalNo ratings yet
- Blood TestDocument2 pagesBlood TestDhruv JainNo ratings yet
- Summary Report:::: Motor Nerve StudiesDocument2 pagesSummary Report:::: Motor Nerve StudiesSonjoy mondalNo ratings yet
- Clinical Data: Patient Name: Age: 50 Years Referring Physician: Date: 4/7/2020 Whole Body FDG PET CT StudyDocument3 pagesClinical Data: Patient Name: Age: 50 Years Referring Physician: Date: 4/7/2020 Whole Body FDG PET CT StudyEl NadiNo ratings yet
- LPL - Rakesh FPSC Shalimar Bagh-4 H. No. 169, AA-Block, Shalimar Bagh, New Delhi-110088. No-7210779305 Delhi 110088Document4 pagesLPL - Rakesh FPSC Shalimar Bagh-4 H. No. 169, AA-Block, Shalimar Bagh, New Delhi-110088. No-7210779305 Delhi 110088Lakshav KapoorNo ratings yet
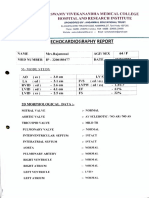
- Rumah Sakit Umum Daerah Muara Teweh Echocardiograpy: Pemerintah Kabupaten Barito UtaraDocument1 pageRumah Sakit Umum Daerah Muara Teweh Echocardiograpy: Pemerintah Kabupaten Barito UtaraMat YasinNo ratings yet
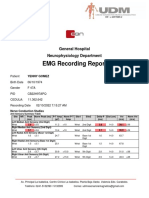
- EMG Report Shows Median Nerve EntrapmentDocument3 pagesEMG Report Shows Median Nerve EntrapmentUnidad de Diagnostico musculoesqueletico UdmNo ratings yet
- CBC and Widal Test ReportDocument4 pagesCBC and Widal Test ReportNeeraj KumarNo ratings yet
- Buletin de Analize 24031517Document3 pagesBuletin de Analize 24031517Iuliana PetrescuNo ratings yet
- David, Rosita7 23 18Document2 pagesDavid, Rosita7 23 18RMH Heart StationNo ratings yet
- resultadopdf (6)Document1 pageresultadopdf (6)Osvaldo TorresNo ratings yet
- Report Sep 22Document11 pagesReport Sep 22roshaniNo ratings yet
- S03 - FPSC Mayur Vihar Extension Shop No-07, Atlantic Plaza, Plot No-1 Samachar Market, Mayur Vihar Phase-1-Ext Mobil No:9811051975Document2 pagesS03 - FPSC Mayur Vihar Extension Shop No-07, Atlantic Plaza, Plot No-1 Samachar Market, Mayur Vihar Phase-1-Ext Mobil No:9811051975Mriganabh ChoudhuryNo ratings yet
- YSIODocument4 pagesYSIOrex.lopez.tmcclarkbiomedNo ratings yet
- ReportDocument16 pagesReportprachiNo ratings yet
- S60 - LPL - Noida 3 N-27, Sec-18, Commercial Complex, Near. Atta Market, Noida.120-3029866/3142530 NoidaDocument6 pagesS60 - LPL - Noida 3 N-27, Sec-18, Commercial Complex, Near. Atta Market, Noida.120-3029866/3142530 NoidaRam Kripal MishraNo ratings yet
- BGH 20220915 202638821232359365Document2 pagesBGH 20220915 202638821232359365kingadityaunhelNo ratings yet
- S53 - FPSC NFC Location D-819, Part A, C V Raman Marg, Near Fortis Escort Hospital, New Friends Colon New DelhiDocument8 pagesS53 - FPSC NFC Location D-819, Part A, C V Raman Marg, Near Fortis Escort Hospital, New Friends Colon New DelhiSohaib DurraniNo ratings yet
- Electrocardiograma NormalDocument6 pagesElectrocardiograma NormalwilmeralfredodelgadillolaraNo ratings yet
- EchoDocument1 pageEchoLukman AgoesNo ratings yet
- Caladiao, Carmelita7-26-18Document2 pagesCaladiao, Carmelita7-26-18RMH Heart StationNo ratings yet
- S28 - Oliva Diagnostics Services Mansoorabad B.O, Plot No:20, H.no:3-9-413 Saraswathi Nagar, Mansoorabad, HyderabadDocument11 pagesS28 - Oliva Diagnostics Services Mansoorabad B.O, Plot No:20, H.no:3-9-413 Saraswathi Nagar, Mansoorabad, HyderabadmohanvajjhaNo ratings yet
- S50 - PSC Gorakhpur - Home Visit 10 Park Road, GORAKHPUR, PH-05512203350Document2 pagesS50 - PSC Gorakhpur - Home Visit 10 Park Road, GORAKHPUR, PH-05512203350Ritika PandeyNo ratings yet
- Training Sessions - 03 11 2020Document3 pagesTraining Sessions - 03 11 2020hussainmiNo ratings yet
- Training ScheduleDocument1 pageTraining SchedulehussainmiNo ratings yet
- Free Vaccination Center in EnglishDocument1 pageFree Vaccination Center in EnglishhussainmiNo ratings yet
- Emirate of Abu Dhabi Reopening Guidelines SummaryDocument4 pagesEmirate of Abu Dhabi Reopening Guidelines SummaryhussainmiNo ratings yet
- PatakDocument183 pagesPatakhussainmiNo ratings yet
- Excellence in Customer ServiceDocument7 pagesExcellence in Customer ServicehussainmiNo ratings yet
- Heg 5Document15 pagesHeg 5Amine HaririNo ratings yet
- Prohibited Diets For Muslims As Per QuranDocument37 pagesProhibited Diets For Muslims As Per QuranhussainmiNo ratings yet
- Friday SurpriseDocument12 pagesFriday SurprisehussainmiNo ratings yet
- BT 002868846 TicketDocument1 pageBT 002868846 Ticketshafi rashid centerNo ratings yet
- Dear Members, We Going To Meet On 28 Feb 2021 Sunday, We Rectify All QuestionsDocument1 pageDear Members, We Going To Meet On 28 Feb 2021 Sunday, We Rectify All QuestionshussainmiNo ratings yet
- Amraz e Jild Aur Tib e Nabvi (S.A.W) PDFDocument353 pagesAmraz e Jild Aur Tib e Nabvi (S.A.W) PDFhussainmiNo ratings yet
- Phonetic Keyboard Layout PDFDocument1 pagePhonetic Keyboard Layout PDFziabutt100% (1)
- 200 PrintDocument4 pages200 PrinthussainmiNo ratings yet
- Aur Line Kat Gai by Prof Ghafoor PDFDocument86 pagesAur Line Kat Gai by Prof Ghafoor PDFhussainmiNo ratings yet
- 200 PrintDocument4 pages200 PrinthussainmiNo ratings yet
- Al Madeena Flyer PDFDocument4 pagesAl Madeena Flyer PDFhussainmiNo ratings yet
- Arbi CalligraphyDocument137 pagesArbi CalligraphyhussainmiNo ratings yet
- Defensive Driving PDFDocument46 pagesDefensive Driving PDFsasaNo ratings yet
- Qureshi 4Document19 pagesQureshi 4Ahmad HassanNo ratings yet
- Dil Ki Bimarian Aur Jadeed Science PDFDocument401 pagesDil Ki Bimarian Aur Jadeed Science PDFhussainmiNo ratings yet
- Al Madeena Flyer PDFDocument4 pagesAl Madeena Flyer PDFhussainmiNo ratings yet
- Driving DrowsyDocument20 pagesDriving DrowsyhussainmiNo ratings yet
- Training Department Arabia Taxi Abu DhabiDocument11 pagesTraining Department Arabia Taxi Abu DhabihussainmiNo ratings yet
- Top 10 tips to avoid speeding and stay safeDocument16 pagesTop 10 tips to avoid speeding and stay safehussainmiNo ratings yet
- 4.mystery Shopper Check-ListDocument10 pages4.mystery Shopper Check-ListhussainmiNo ratings yet
- Road Rage: Aggressive Driving On The RoadDocument22 pagesRoad Rage: Aggressive Driving On The RoadeastNo ratings yet
- Defensive Driving Course GuideDocument4 pagesDefensive Driving Course GuidehussainmiNo ratings yet
- Defensive Driving: For Noncommercial MotoristsDocument25 pagesDefensive Driving: For Noncommercial MotoristsHalasyanathan GanesanNo ratings yet
- 45-Article Text-183-1-10-20211230Document13 pages45-Article Text-183-1-10-20211230Eprilia AnnisyaNo ratings yet
- Clinical Differentiation of Upper Extremity Pain EtiologiesDocument9 pagesClinical Differentiation of Upper Extremity Pain EtiologiesmarcosgabNo ratings yet
- Carpal Tunnel SyndromeDocument7 pagesCarpal Tunnel Syndromeclaudia100% (1)
- Tarsal Tunnel SyndromeDocument2 pagesTarsal Tunnel SyndromeMuhammad Amri KautsarNo ratings yet
- Carpal Tunnel SyndromeDocument24 pagesCarpal Tunnel SyndromeReymond GuevarraNo ratings yet
- MS 36Document7 pagesMS 36jefrocNo ratings yet
- Hypothalamus and Amygdala Response To Acupuncture StimuliDocument13 pagesHypothalamus and Amygdala Response To Acupuncture StimuliAnibal CisternasNo ratings yet
- Online Gaming's Impact on Student HealthDocument11 pagesOnline Gaming's Impact on Student HealthPrincemarty2350% (2)
- Ergo ExercisesDocument30 pagesErgo ExercisesASR REDDYNo ratings yet
- Soft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistDocument54 pagesSoft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistarunupadhayaNo ratings yet
- Common Orthopedic Conditions of The HandDocument3 pagesCommon Orthopedic Conditions of The HandAb C. HermosoNo ratings yet
- PowerPoint Bursitis Tendonitis EnglishDocument109 pagesPowerPoint Bursitis Tendonitis EnglishPhil Adit RNo ratings yet
- Alliance Physical TherapyDocument178 pagesAlliance Physical TherapyAlliance Physical Therapy100% (1)
- Efficacy of Low-Level Laser Therapy in Carpal Tunnel Syndrome ManagementDocument10 pagesEfficacy of Low-Level Laser Therapy in Carpal Tunnel Syndrome ManagementChung Tze YangNo ratings yet
- Revision of SpacesDocument6 pagesRevision of SpacesFrancesca vitaleNo ratings yet
- Carpal TunnelDocument1 pageCarpal TunnelKadek Rudita YasaNo ratings yet
- Chapter 17Document105 pagesChapter 17Quangnd100% (3)
- 9 Pregnancy Stretches For The Whole Body 4 Pager Apr17 v3Document4 pages9 Pregnancy Stretches For The Whole Body 4 Pager Apr17 v3LeiltonNo ratings yet
- How To Prevent RSI - The Michelangelo CodeDocument59 pagesHow To Prevent RSI - The Michelangelo Codedel0gNo ratings yet
- Perils of Nigerian WorkersDocument32 pagesPerils of Nigerian WorkersChux ElumezeNo ratings yet
- Post Test 09Document2 pagesPost Test 09Evangeline Olarte QuilantangNo ratings yet
- Neuromuscular System 1Document13 pagesNeuromuscular System 1Shimmering MoonNo ratings yet
- Bursitis Tendinitis BrochureDocument8 pagesBursitis Tendinitis BrochureSebastian Cornellius Dicky Panduwinata100% (1)
- Impact of Information and Communication Technology On Child Health: ICT and Child HealthDocument6 pagesImpact of Information and Communication Technology On Child Health: ICT and Child HealthElena ElenaNo ratings yet
- Prevalence of Carpal Tunnel Syndrome Symptoms Among Dentists in Benghazi City - LibyaDocument6 pagesPrevalence of Carpal Tunnel Syndrome Symptoms Among Dentists in Benghazi City - LibyaIJAR JOURNALNo ratings yet
- Penatalaksanaan Fisioterapi Pada Kondisi Modalitas Ultrasound (Us) Dan Terapi Latihan Di Rsud Bendan Kota PekalonganDocument10 pagesPenatalaksanaan Fisioterapi Pada Kondisi Modalitas Ultrasound (Us) Dan Terapi Latihan Di Rsud Bendan Kota PekalongannurNo ratings yet
- Ict OhsDocument26 pagesIct Ohscloyd mark cabusogNo ratings yet
- Case Study on Graded Return to Work Program for Carpal Tunnel SyndromeDocument11 pagesCase Study on Graded Return to Work Program for Carpal Tunnel SyndromeMargeaux Deb Bartholomew CarleNo ratings yet
- 2 51 1656420123 1ijmpsdec20221Document4 pages2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNo ratings yet
- Carpal Tunnel Syndrome: Wren V. Mccallister, MDDocument43 pagesCarpal Tunnel Syndrome: Wren V. Mccallister, MDRohit LuthraNo ratings yet