Professional Documents
Culture Documents
Assessment of The Male Reproductive System: Pamela D. Ceo
Assessment of The Male Reproductive System: Pamela D. Ceo
Uploaded by
pravina praviOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Assessment of The Male Reproductive System: Pamela D. Ceo
Assessment of The Male Reproductive System: Pamela D. Ceo
Uploaded by
pravina praviCopyright:
Available Formats
UNJ August 2006-290.
ps 7/24/06 3:14 PM Page 290
Assessment of the Male
Reproductive System
Pamela D. Ceo
Many diseases and medications can affect the urinary system and its
T
he importance of a good
physical examination function. Assessment of the male genitalia is accomplished with
cannot be underestimat- inspection and palpation. It is important to chart what is seen, what
ed. A good clinician is felt, and what the patient reports.
must be able to differentiate nor-
mal from abnormal findings and
should be familiar with both func- urinary tract infection, or treat- Cappaleri, Smith, Lipsky, & Pena,
tion (see Table 1) and location (see ment for low-grade bladder can- 1999).
Table 2) of the organs involved. It cer. Complaints of a lump in the
may be as subtle as a mole that scrotum can be an inguinal her- Examination Basics
has changed slightly from last nia. It is always important to dis- Upon entering the examina-
examination or as obvious as a cuss and clarify the details of any tion room, the clinican should
new lesion that is draining. previous genitourinary (GU) greet the patient appropriately
surgeries, particularly if they with an introduction including
Obtaining the History occurred during childhood. the clinician’s title. The patient
Many diseases and medica- Details of any previous treatment should be asked what he would
tions can affect the urinary sys- for GU diseases or complaints prefer to be called. This simple
tem and its function. The initial should be discussed. Ask the introduction can help reduce
interaction with a patient should patient whether he has been anxiety, particularly when the
begin in a nonthreatening way, treated recently in an emergency specific encounter is related to a
by reviewing his medical-surgi- department for the presenting man’s sexual or urological
cal history and his current med- problem or any other problem. health. If a genital examination is
ications. A complete assessment There are some conditions necessary, permission is asked
of the male reproductive system for which a physical examination before beginning the examina-
includes a thorough review of the is only modestly helpful. Erectile tion. This is especially important
patient’s history, since many con- dysfunction cannot be seen or when the clinician is a female,
ditions may present as com- felt during a physical examina- since it allows the patient to
plaints of pain to the reproduc- tion; therefore, this issue should decline gracefully if he prefers a
tive structures. Pain from a kid- be discussed with the patient. male clinician to perform this
ney stone can radiate along the Ask about his relationship(s) and part of the examination. Genital
spermatic cord and present as about his level of sexual satisfac- examination should be done last
testicular pain. Difficulty starting tion. If the patient has diabetes, if this is a full physical examina-
the urinary stream and com- hypertension, or depression and tion, in order to reduce embar-
plaints of perineal tenderness takes medication for these condi- rassment and to allow time for
may indicate prostatitis or tions, he may have erectile prob- the patient to become comfort-
benign prostatic hypertrophy. lems but may be too embarrassed able with the overall interaction.
Urethral pain can be a result of to talk about it. A statement such A parent should always be pre-
prostatitis, sexually transmitted as “Diabetes often causes erectile sent when examining an infant or
diseases, or recent instrumenta- dysfunction. Have you encoun- minor. The adolescent should be
tion. Urgency and frequency may tered any problems getting an asked if he would like to have
be due to bladder dysfunction, a erection?” or use of a standard- anyone present during the exam-
ized questionnaire may encour- ination. An adult male should be
age the patient to discuss the asked the same question, espe-
Pamela D. Ceo, APRN,BC, CUNP, is problem more openly (for exam- cially if he is accompanied by his
a Urology Nurse Practitioner, St. ple, the Sexual Health Inventory wife. Social or cultural mores
Joseph Mercy Hospital, Ann Arbor, MI. for Men [SHIM] by Rosen, may dictate that the wife leave
290 UROLOGIC NURSING / August 2006 / Volume 26 Number 4
UNJ August 2006-291.ps 7/24/06 3:14 PM Page 291
Table 1. the room during her husband’s
Function of Male Genital Organs examination.
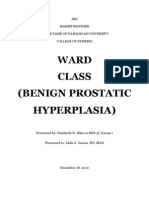
Assessment of the male geni-
Organ Function talia (see Figure 1) is accom-
Penis Protects the urethra; houses the corpora caver- plished with inspection and pal-
nosum which when engorged makes the penis pation. Normally, only examina-
rigid and erect; prepuce protects the glans penis. tion gloves and water-soluble
Scrotum Protective loose sac divided into two compart- lubricant are needed but a stetho-
ments for the internal organs: testis, epididymis, scope and flashlight may be use-
and vas deferens; temperature regulation of the ful if the scrotal examination is
testes. abnormal. A stethoscope can be
used to listen for bowel sounds if
Testes Produce spermatozoa (seminiferous tubules) and
testosterone. there is a concern for a hernia
within the scrotal sac. The flash-
Epididymis Storage and transport of sperm cells; sperm mat- light would be used to transillu-
uration.
minate the scrotum during an
Ductus (Vas) deferens Cord-like structure that transports sperm from evaluation for a hydrocele. Prior
the testis and epididymis into the urethra. to any examination, the index
Spermatic cord Protects the ductus (vas) deferens, internal and finger can be measured and used
external spermatic arteries, artery of the vas, as a ruler to measure the penis,
venous pampiniform plexus, lymph vessels, and testes, and prostate.
nerves. With the patient in the
Prostate gland Produces some of the seminal fluid; also pro- supine position, only the geni-
duces a thin, white fluid that mixes with seminal talia are uncovered and two
fluid to neutralize the urethra and vagina to main- sheets are used, one to cover his
tain sperm viability. chest/abdomen area and the
other one to cover his legs.
Seminal vesicles Produces most of the seminal fluid.
Privacy for the patient is always
Table 2.
Developmental Changes in the Appearance of the Male Genital Organs
Developmental
Time Pubic Hair Appearance of Penis Testes and Scrotum
Stage 1 None except for fine body hair Size proportional to body Size proportional to body size
as on the abdomen. size as in childhood as in childhood
Stage 2 Sparse, long, slightly pigmented Slight enlargement Enlargement of testes and
thin hair at the base of penis. scrotum; reddened pigmenta-
tion; texture more prominent.
Stage 3 Darkens, becomes more coarse Elongation Enlargement continues.
and curly; growth extends over
symphysis.
Stage 4 Continues to darken, thicken, and Breadth and length Enlargement continues;
become coarser and more curly; increase, glans develops. skin pigmentation darkens.
growth extends laterally, superi-
orly, and inferiorly.
Stage 5 Adult distribution and appear- Adult appearance Adult appearance
ance; growth extends to inner
thighs, umbilicus, and anus, and
is abundant.
Stage 6 Sparse and gray Decrease in size Testes hang low in scrotum;
(Elderly clients) scrotum appears pendulous.
Source: Barkauskas, Baumann, & Darling-Fisher, 2002.
UROLOGIC NURSING / August 2006 / Volume 26 Number 4 291
UNJ August 2006-292.ps 7/24/06 3:14 PM Page 292
Figure 1. provided. The room should be
Male Anatomy warm enough for the patient to
be comfortable. The patient
should be asked if the room is
warm enough. This is especially
important in examining the
elderly, since they may be less
tolerant of the cold. The warm
room will also avoid activation
of the cremasteric reflex that
causes the testes to ascend from
the scrotum upward toward the
pelvic cavity (Pulsifer, 2005).
This reflex can also be provoked
by touch. If possible, interrup-
tions should be avoided after the
examination is begun.
INSPECTION
Source: Marieb, 2006. Used with permission of Pearson Education, Inc. Pubic Area/Penis
The patient’s hair distribu-
Table 3. tion pattern is examined (see
Pubic Area/Penis Hair Distribution Table 3). Does it correlate with
his age? The suprapubic area is
Infant/child No hair inspected for any rashes,
Adolescence Few hairs on pubic area at first, then becomes fuller lesions, folliculitis, scarring,
(see Table 2). nodules, bulges, or scratch
marks (from a parasite). If the
Adult Abundant in pubic area, coarser than hair on other parts
of the body, curlier and on medial aspects of thighs hair is full it will need to be
parted during the examination.
Geriatric Gray and sparse The inguinal/groin area is
inspected. When the patient
coughs or bears down there
Figure 2. should not be any bulges or
Differentiating Hernias masses. If there are, this may
indicate a hernia. A direct
inguinal hernia would be near
the external inguinal ring, while
an indirect inguinal hernia
would be at the internal inguinal
ring (see Figure 2).
Penile growth rate is progres-
sive and predictable (see Table
4). An abnormally small penis
may be indicative of a clitoris,
Klinefelter’s or Down’s syndrome
(Gomella, 2002). An obese child
may appear to have a small
(retracted) penis secondary to
overlying skin folds and large
prepubic fat pad (Engel, 2002). A
penis that is large relative to stage
Source: Swartz, 2002. Used with permission of W.B. Saunders Company. of development may suggest pre-
cocious puberty or a possible tes-
ticular tumor (Engel, 2002).
292 UROLOGIC NURSING / August 2006 / Volume 26 Number 4
UNJ August 2006-293.ps 7/24/06 3:15 PM Page 293
Table 4. from the tip of the penis to the
Penis Size/Length penoscrotal junction. Both of
these disorders are congenital
Infant/child Size 1.9 cm newborn and up to 3 cm in young boys and are usually diagnosed at
until puberty. birth.
Adolescence Enlarges to adult size.
Urethral Meatus
Adult Size varies from male to male average: flaccid 4 to 10 When inspecting the urethral
cm; stretched 7 to 13 cm; color usually darker than the meatus, the glans is gently com-
skin on other parts of the body; skin should be smooth
and hairless and cylindrical in shape.
pressed between the index finger
(positioned on the dorsal surface)
Geriatric Retracted, small with some surface vascularities. and thumb (positioned on the ven-
tral surface). This will open the
Sources: Gomella, 2000; Jarvis, 2004; Shamloul, 2005.
meatus for inspection. Any dis-
charge, warts, lesions, swelling,
Table 5. inflammation, and shape are
Prepuce (Foreskin) noted. If the meatus is round this
may be indicative of meatal steno-
Infant/Child May or may not be present. sis secondary to repeated infection
Adolescence May or may not be present. (Engel, 2002) (see Table 7).
Many patients who have a
Adult/Geriatric May or may not be present.
sexually transmitted disease
(STD) present with dysuria and
penile discharge, but an asymp-
Table 6.
tomatic patient could also have
Glans Penis
an STD. That is why issues of
All ages Glans penis size should be proportional to the penis, and the sexuality should be addressed
skin should be smooth. during the examination, espe-
cially if an STD is suspected.
Questions about the number of
sexual partners, sexual prefer-
Prepuce/Foreskin are at a higher risk for penile can- ences, whether the current rela-
If the male is circumcised, cer, with the glans being the first tionship is monogamous, and
the prepuce is removed, and the site and the prepuce the sec- condom use can be asked in a
glans penis is exposed. For uncir- ondary site (see Table 5). professional, nonjudgmental
cumcised males the prepuce and nonthreatening manner. A
(foreskin) is retracted. The pre- Glans Penis clinician should never assume
puce is normally adherent in To inspect the glans penis the that elderly patients are not sex-
children younger than 3 years of prepuce must be retracted, if the ually active, especially if wid-
age. Older than 3 years of age, an male has not been circumcised. owed or divorced. Keep in mind
attempt can be made to retract Any lesions, drainage, warts, that symptoms associated with
the prepuce, but it should not be scars, rash, skin texture, color, or untreated gonorrhea could be
forced (Engel, 2002). An unre- swelling are noted. Inflammation interpreted as another disease
tractable prepuce may be indica- of the glans is called balanitis and more common in the elderly,
tive of phimosis and the patient may be caused by a fungal infec- such as prostate problems or
should be referred to a urologist. tion or tinea. Balanoposthitis is arthritis (Grigg, 2000). Older
Any drainage, lesions, scars, inflammation of both the glans adults may not use condoms
rash, or swelling are noted. There and prepuce (see Table 6). since they do not perceive a risk
may be a white, cheesy sub- If the male is uncircum- of pregnancy. Many older adults
stance, called smegma, and this cised, the prepuce is retracted do not understand STDs and
is normal. The prepuce must to expose the glans penis. If the their vulnerability to them.
always be replaced back over urethral meatus is located on When examining a child or ado-
the glans (head of the penis). If the dorsal (upper side) surface it lescent, sexual activity or sexual
the prepuce cannot be advanced is called epispadias. If it is abuse should be suspected if
over the glans, this is a condition located on the ventral (under- genital warts are present. Both
called paraphimosis. The patient side) surface it is called STDs and suspected sexual
should be referred emergently to hypospadias and can be located abuse are reportable events.
a urologist. Uncircumcised males anywhere on the ventral surface
UROLOGIC NURSING / August 2006 / Volume 26 Number 4 293
UNJ August 2006-294.ps 7/24/06 3:15 PM Page 294
Shaft of Penis Table 7.
The color of the skin on the Urethral Meatus
shaft of the penis varies and the
dorsal vein may be prominent. All ages The urethral meatus should be positioned centrally at the tip
of the glans penis and appear as a pink slit.
The skin is inspected for any
lesions, scars, genital warts, rash,
swelling, or noticeable nodules
(see Table 8). Table 8.
Shaft of Penis
Scrotal Sac All ages The skin of the shaft should be smooth to slightly wrinkled
When the ambient air is and hairless.
warm, the scrotal sac is more
pendulous and the skin is
smoother but when the ambient Table 9.
air is cold, the scrotal sac Skin of the Scrotum/Perineum
becomes contracted and the skin
more wrinkled (see Table 9) Infant/Child Rugae (wrinkles or folds) skin surface, color pink in white
(Swartz, 2002). Any rashes, geni- infants and dark brown in dark-skinned infants; perineum:
tal warts, scars, lesions, or color moist and hairless.
changes are noted. Sebaceous
Adolescence Skin surface becoming coarser with more rugae and skin
cysts are common; these are cysts pigmentation darkens, the skin contains both hair and
that have a waxy appearance and sweat glands; perineum: hair growth to rectum.
can become inflamed and drain a
cheesy material. Pain, necrosis, Adult Skin slightly loose, skin surface coarse and with rugae, skin
and swelling of the scrotal sac in darker than rest of body, the skin contains both hair and
a diabetic male may be signs of sweat glands; perineum: hair growth to rectum; better
Fournier’s gangrene; this is a uro- inspection with rectal examination.
logic emergency. Any drainage, Geriatric Skin becomes pendulous and less rugae, skin color darker
redness, bulges, lesions, or geni- than rest of body and skin with hair; perineum: hair growth
tal warts on the perineum are to rectum; better inspection with rectal examination.
noted. The anal area is stroked to
elicit the anal reflex. The anus
should contract quickly. Slow Table 10.
reflex could indicate a disorder Contours of the Scrotum
of the pyramidal tract (Engel,
2002). All ages The left testicle may be lower than the right and therefore
If the scrotal sac appears appear asymmetrical.
“sunken in” on one side or both
sides, the testicle(s) may be
absent; an underdeveloped, non-
pendulous hemiscrotum com- nia (see Figure 2). soft, and without tenderness.
monly indicates undescended In the elderly patient, thick- During palpation any tenderness,
testis (see Table 10). If the scrotal ening of the scrotal sac may nodularity, or induration is
sac is edematous it may be occur in association with fluid noted. Tenderness along the ven-
indicative of a hernia or hydro- retention which can be associat- tral (underside) aspect of the
cele. To differentiate between the ed with cardiac, renal, or hepatic penis is indicative of periurethri-
two, a flashlight is placed against diseases (Gomella, 2002). Edema tis, which is often secondary to
the scrotal sac posteriorly with may also occur in epididymitis or urethral stricture. The patient
the room dark (transillumina- other local inflammation and should fill out the International
tion). If there is a red glow, it is obstruction of the inguinal lym- Prostate Symptom Score (I-PSS),
likely a hydrocele. No light will phatics (Jarvis, 2004). which is a helpful tool that
transmit through a solid tumor. addresses bladder emptying, fre-
Another way to differentiate PALPATON quency, intermittency, urgency,
scrotal swelling is to “get above” stream, and nocturia. This
the swelling. If this is possible, Penis should be assessed annually and
the swelling is scrotal and if not, The penis is palpated using as needed. Curvature, nodularity,
the swelling is inguino-scrotal the thumb and first two fingers. or induration of the penis sug-
and most likely an inguinal her- The penis should feel smooth, gests Peyronie’s disease. The
294 UROLOGIC NURSING / August 2006 / Volume 26 Number 4
UNJ August 2006-295.ps 7/24/06 3:15 PM Page 295
patient is asked if he is able to Table 11.
obtain an erection, and if so, Testes
whether there is any pain or cur-
Infant/Child Size 1.5 cm until puberty.
vature.
Adolescence/Adult Approximately 4.0 to 5.5 cm in length, 2.5 cm in
Scrotum width.
The skin of the scrotum is Geriatric Less firm and slightly smaller.
palpated using the thumb and
first two fingers. The scrotal sac Source: Rowland & Herman, 2002.
is divided into two compart-
ments. The contents should slide Table 12.
easily. Abnormalities within the Normal Prostate
scrotal sac are hydroceles and
hernias. A hydrocele is a collec- 4 cm wide, 2.5 to 3.0 cm long
tion of fluid that surrounds the
testes, which can be transillumi- Source: Grayback, McVary, & Kozlowski, 2002.
nated. Hydroceles can occur at
any age. A hernia is a portion of
bowel that protrudes into the sign of sexual maturation. This is absent, this is often associated
scrotal sac. A hernia does not can occur as early as age 10 years with an absent kidney on the
transilluminate but it may be (Engle, 2002). A small (<3.5 cm) same side (Swartz, 2002). The
possible to auscultate bowel and soft testis may indicate atro- spermatic cord may become tor-
sounds. phy as with cirrhosis, hypopitu- tuous which is a varicocele and
itarism, or may occur following feels like a “bag of worms.” The
Testes estrogen therapy or androgen spermatic cord may also form a
The testis is palpated gently blockade. If the testis is smaller cyst after a vasectomy that is
with the thumb and first two fin- than 2 cm and alopecia in the painless and contains sperm
gers (see Table 11). Each testis is pubic region is noted, suspect (spermatocele).
palpated separately; they should Klinefelter’s syndrome (hypogo-
be ovoid, firm and smooth, much nadism) (Jarvis, 2004). Inguinal Area/Lymph Nodes
like a hard-boiled egg. The testis The inguinal area is palpated
should feel suspended and move Epididymis/Ductus (Vas) for pulses, using the pads of the
easily in each sac. The testes Deferens/Spermatic Cord index, middle, and ring fingers.
should have the same consisten- The epididymis is located on Decreased or absent pulses may
cy and be nearly the same size. A the posterior aspect of the testes. indicate a vascular problem. The
firm nodule may indicate a tes- It is palpated gently with the inguinal (superficial) and subin-
ticular tumor. The testes can thumb and first two fingers. The guinal (deep) lymph nodes are
become infected (orchitis). epididymis should be nontender, palpated. The lymph nodes are
To prevent the creamateric smooth, and feel softer than the usually not felt. An enlarged
reflex during palpation in infants testes. Palpate upwards toward lymph node may represent
and young children, either a fin- the inguinal ring using only the inflammation or metastatic dis-
ger is held over the inguinal thumb and index finger to feel ease spread from the genital or
canal while palpating the scrotal the ductus (vas) deferens. It peri-anal area. Note any tender-
sac or have the child sit cross- should feel smooth and be non- ness and size of lymph node.
legged. Inability to palpate a tender. It feels like partially
testis in an infant may indicate cooked spaghetti and is about 2 Prostate and Seminal Vesicle
cryptorchidism (undescended mm to 4 mm in diameter. A normal prostate feels sym-
testis) and the testis may be pal- Upward, a thicker cord (spermat- metrical, smooth, rubbery, with-
pated in the inguinal canal. The ic cord) is felt. It should also be out tenderness and the median
testis may descend on its own as smooth and nontender. Palpate sulcus is palpable; benign dis-
the infant grows. If it has not the right side first, then the left ease feels like the tip of a nose
descended by 1 year old, surgical side. whereas a cancerous nodule feels
correction should be done Abnormalities are infection more like a forehead (see Table
(McAninch, 2000). If the cryp- of the epididymis, ductus (vas) 12). The prostate may also feel
torchid testis is not corrected, the deferens, and spermatic cord. flat, indurated (hardened), boggy
male is at a higher risk of infertil- The epididymis can also be (spongy), or enlarged. Seminal
ity and testicular cancer. nodular, which may be indicate a vesicles lie cephalic to the
Testicular growth is a visible cyst or tumor. If the vas deferens prostate, are about 6 cm long and
UROLOGIC NURSING / August 2006 / Volume 26 Number 4 295
UNJ August 2006-296.ps 7/24/06 3:15 PM Page 296
soft, normally nonpalpable; if is instructed to bear down, as if he assessment (3rd ed.) (pp. 496-514).
they are palpable, this may be were having a bowel movement. St. Louis: Mosby.
Engel, J. (2002). Reproductive system. In J.
suspicious for cancer. This relaxes the rectal sphincter Engel (Ed.), Pocket guide to pediatric
The digital rectal examina- and allows for easy insertion of assessment (4th ed.) (pp. 215-229).
tion should be explained to the the finger. The index finger is St. Louis: Mosby.
patient. Advise him to report any inserted as far as possible, as the Gomella, L. (2002). The 5-minute urology
consult (1st ed.) (pp. 30, 344).
tenderness or pain experienced patient relaxes and breathes Philadelphia: Lippincott, Williams &
during the examination. The deeply. The sphincter tone is Wilkins.
location of any significant dis- noted and the prostate is palpated Grayback, J., McVary, K., & Kozlowski, J.
comfort or abnormality is identi- using the finger as a ruler to assess (2002). Benign prostatic hyperplasia.
fied by using the face of a clock the size of the gland (side to side In J. Gillenwater, J. Grayhack, S.
Howards, & M. Mitchell (Eds.), Adult
as a reference point (for example, and top to bottom). With slight and pediatric urology (4th ed.) (pp.
the lesion is at the 3 o’clock posi- pressure, palpate the lateral right 1401-1470). Philadelphia: Lippincott,
tion on the rectum). The width of side from top to bottom (base to Williams & Wilkins.
the clinician’s index finger (usu- apex), move the finger to the cen- Grigg, E. (2000). Sexually transmitted
infections and older people. Nursing
ally about 1.5 cm-2 cm) and the ter, which should dip down Standard, 14(39), 48-53.
length of the finger can be mea- (median sulcus), and continue to Jarvis, C. (2004). Male genitalia. In C. Jarvis
sured and used as a reference to move to the lateral left side, pal- (Ed.), Physical examination and
help measure the prostate. pating from top to bottom. health assessment (4th ed.) (pp. 721-
If the patient is unable to Normally the seminal vesicles are 748). St. Louis: W.B. Saunders.
Marieb, E. (2006). Essentials of human
stand, the rectal examination can not palpable. The prostate should anatomy & physiology (8th ed.) (pp.
be done in either the Sims’ or dor- be symmetrical, feel smooth, rub- 528-563). San Francisco: Pearson
sal recumbent position. To place bery, and without tenderness. The Education, Inc.
the patient in the Sims’ position, prostate may be enlarged especial- McAninch, J. (2000). Disorders of the
testis, scrotum and spermatic cord. In
he should lie on his left side with ly if the male is older. Prior to E. Tanagho & J. McAninch (Eds.),
his right thigh and knee, flexed as removing the finger, palpate the Smith’s general urology (15th ed.)
much as possible, over his left leg, rectal wall for nodules and ten- (pp. 684-693). New York: Lange
which is also partially flexed. To derness. This completes the digi- Medical Books/McGraw-Hill.
place the patient in the dorsal tal rectal examination. Pulsifer, A. (2005). Pediatric genitourinary
examination: A clinician’s reference.
recumbent position, have him lie Any stool on the gloved finger Urologic Nursing, 25(3), 163-168.
on his back with his hips and should be checked for occult Rosen, R., Cappalleri, J., Smith, M., Lipsky,
knees bent (flexed), and feet flat blood. Either the rectum is wiped J., & Pena, N. (1999). Development and
on the examination table or mat- free of lubricant with a tissue or evaluation of an abridged, 5-item ver-
sion of the International Index of
tress (if the patient is in the bed). the tissue is offered to the patient. Erectile Function (IIEF-5) as a diagnos-
Otherwise, have the patient stand The patient is allowed to stand up tic tool for erectile dysfunction.
on the floor. The scrotal sac is and get dressed. International Journal of Impotence
inspected again since hydroceles Research, 11, 319-326.
and hernias may be more promi- Conclusion Rowland, R., & Herman, J. (2002). Tumors
and infectious diseases of the testis,
nent in the standing position. Any No matter how long a clini- epididymis, and scrotum. In J.
abnormalities not detected earlier cian has been performing a male Gillenwater, J. Grayhack, S. Howards,
with palpation are noted. The genital examination, there can be & M. Mitchell (Eds.), Adult and pedi-
patient should turn around facing some level of discomfort or anxi- atric urology (4th ed.) (pp. 1897-
1934). Philadelphia: Lippincott,
the examination table for the ety from the clinician, the nurse Williams & Wilkins.
prostate examination. The patient (male or female), or the patient. Shamloul, R. (2005). Treatment of men
is told to bend forward (flexing at Confidence and competence in complaining of short penis. Urology,
hips) and rest his forearms and the physical examination tech-
elbows on the table while bending nique takes time to accomplish.
his knees slightly. The patient is There may also be unusual find- CE test located on page 297.
advised that the examination is ings on the genitals such as tattoos
about to begin. The buttocks are and/or piercings. The clinician
spread to inspect the rectal area should always remain profession- 65(6), 1183-1185.
Swartz, M. (2002). Male genitalia and her-
for hemorrhoids, genital warts, al and nonjudgmental. It is impor-
discharge, or rashes. The rectal tant to chart what is seen, what is Need CE Credit?
nias. In M. Swartz (Ed), Textbook of
physical diagnosis history and exam-
area is palpated for nodules and felt, and what the patient reports. Visit the “Education”
ination (4th ed.) (pp. 461-494).
tenderness. The clinician’s gloved • Philadelphia: W.B. Saunders.
index finger of the dominant hand section at
is lubricated. The clinician places References
it at the anal verge and the patient Barkauskas, V., Baumann, L., & Darling- www.suna.org
Fisher, C. (2002). Health and physical
296 UROLOGIC NURSING / August 2006 / Volume 26 Number 4
You might also like
- Anorectal MalformationDocument4 pagesAnorectal MalformationFawzia Haznah Nurul ImaniNo ratings yet
- A Case Study of A Patient With A Diagnosis of Prostate CancerDocument9 pagesA Case Study of A Patient With A Diagnosis of Prostate Cancer'jmark FranciaNo ratings yet
- Benign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraDocument56 pagesBenign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraJessica PurbaNo ratings yet
- Case Study On Prostate CancerDocument16 pagesCase Study On Prostate Cancerferdz02100% (5)
- Nursing Diagnosis of Prostate CancerDocument3 pagesNursing Diagnosis of Prostate CancerSyafiqAzizi100% (1)
- Undescended TestesDocument29 pagesUndescended TestesHillary Bushnell100% (1)
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic HyperplasiaLag Lag AlbercaNo ratings yet
- Buried PenisDocument3 pagesBuried Penischoirin nurNo ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- Screenshot 2021-12-09 at 11.53.30Document8 pagesScreenshot 2021-12-09 at 11.53.30mithaNo ratings yet
- Stress IncontinenceDocument35 pagesStress IncontinenceVeronica MendozaNo ratings yet
- p141 PDFDocument7 pagesp141 PDFAde FadilNo ratings yet
- Pelvic Organ Prolapse Quantification System (POP-Q) - A New Era in Pelvic Prolapse StagingDocument7 pagesPelvic Organ Prolapse Quantification System (POP-Q) - A New Era in Pelvic Prolapse StagingAnditha NamiraNo ratings yet
- Assessment and Diagnostic ExamsDocument10 pagesAssessment and Diagnostic ExamsJan Mark SotoNo ratings yet
- Best of The 2001 AUA Annual MeetingDocument14 pagesBest of The 2001 AUA Annual MeetingneleatucicovshiiNo ratings yet
- Focseneanu2015 PDFDocument3 pagesFocseneanu2015 PDFAniydaNo ratings yet
- Repro CorrDocument67 pagesRepro CorrsrhmdNo ratings yet
- Ethics FinalDocument7 pagesEthics FinalMADIZA AMBOLNo ratings yet
- Parurethral CystsDocument3 pagesParurethral CystsIoannis ValioulisNo ratings yet
- Malignant Struma OvariiDocument4 pagesMalignant Struma Ovariixwahyu 108No ratings yet
- Delay in Diagnosis of Congenital Anal ST PDFDocument4 pagesDelay in Diagnosis of Congenital Anal ST PDFJimi Kalvin SarareniNo ratings yet
- New Developments in Anal Surgery Congenital Ano RectalDocument5 pagesNew Developments in Anal Surgery Congenital Ano RectalOctavianus KevinNo ratings yet
- Pelvis Perineum Cases 04Document5 pagesPelvis Perineum Cases 04Uloko ChristopherNo ratings yet
- A Histological Study of ProstateDocument6 pagesA Histological Study of ProstatealdyNo ratings yet
- Postoperative Urinary Retention: Anesthetic and Perioperative ConsiderationsDocument19 pagesPostoperative Urinary Retention: Anesthetic and Perioperative Considerationspooria shNo ratings yet
- Module 6 Assignment Cortez and Salalila PDFDocument5 pagesModule 6 Assignment Cortez and Salalila PDFjennielunay00No ratings yet
- 14 Vol. 11 Issue 11 Nov 2020 IJPSR RE 3646Document7 pages14 Vol. 11 Issue 11 Nov 2020 IJPSR RE 3646Ehwanul HandikaNo ratings yet
- Large, Solitary, Luteinized Follicle Cyst of Pregnancy and PuerperiumDocument5 pagesLarge, Solitary, Luteinized Follicle Cyst of Pregnancy and PuerperiumMade RusmanaNo ratings yet
- Nursing Gyne Assessment PDFDocument6 pagesNursing Gyne Assessment PDFfaria ejazNo ratings yet
- Evaluation of Neck MassDocument17 pagesEvaluation of Neck MassMuammar Aqib MuftiNo ratings yet
- Tuberculous Peritonitis Presenting As An Acute Abdomen: A Case ReportDocument4 pagesTuberculous Peritonitis Presenting As An Acute Abdomen: A Case ReportDumitru RadulescuNo ratings yet
- Conservative Management of Pelvic Organ ProlapseDocument14 pagesConservative Management of Pelvic Organ ProlapseMarianaNo ratings yet
- Lecture Notes AnatomyDocument18 pagesLecture Notes AnatomyFau Fau DheoboNo ratings yet
- Auto Article ProcessDocument6 pagesAuto Article ProcessJamshaid AhmedNo ratings yet
- Desordenes Testiculares AgudosDocument9 pagesDesordenes Testiculares AgudosHernan Del CarpioNo ratings yet
- Intraabdominal Mass in NewbornDocument8 pagesIntraabdominal Mass in NewbornSridhar KaushikNo ratings yet
- ACOG Updates Guideline On Diagnosis and TreatmentDocument2 pagesACOG Updates Guideline On Diagnosis and TreatmentMichelle DefandiNo ratings yet
- Cervical Mucus Analysis: A Major Component in Evaluation of InfertilityDocument4 pagesCervical Mucus Analysis: A Major Component in Evaluation of InfertilityfifahcantikNo ratings yet
- Routine First Trimester Ultrasound Dcreening Using Standardized Anatomical ProtocolDocument15 pagesRoutine First Trimester Ultrasound Dcreening Using Standardized Anatomical ProtocolDimas Rahman SetiawanNo ratings yet
- An Evidence-Based Manual For Abdominal Paracentesis: Grant I. Chen Sander Veldhuyzen Van ZantenDocument9 pagesAn Evidence-Based Manual For Abdominal Paracentesis: Grant I. Chen Sander Veldhuyzen Van ZantenIULIAN LUPUNo ratings yet
- Grand Case Pres - Transverse Vaginal Septum..Document32 pagesGrand Case Pres - Transverse Vaginal Septum..Gio LlanosNo ratings yet
- Lung Ca Case StudyDocument3 pagesLung Ca Case StudyJoseNo ratings yet
- Chen, WW SurgDocument4 pagesChen, WW SurgMichael ChenNo ratings yet
- Canine Prostatic Diseases: Reproduction and Periparturient CareDocument13 pagesCanine Prostatic Diseases: Reproduction and Periparturient CareSatria Adi MarhendraNo ratings yet
- Assessment of The Urinary System: Chelsye Marviyouna Dearianto 1814201018Document19 pagesAssessment of The Urinary System: Chelsye Marviyouna Dearianto 1814201018Sinta WuLandariNo ratings yet
- FulltextDocument12 pagesFulltextn2763288No ratings yet
- Ambiguous Genitalia 3Document4 pagesAmbiguous Genitalia 3syarifah salmaNo ratings yet
- Interpretation of Urodynamic Studies: A Case Study-Based GuideFrom EverandInterpretation of Urodynamic Studies: A Case Study-Based GuideNo ratings yet
- Cloacal Prolapse in TortoiseDocument21 pagesCloacal Prolapse in TortoiseNabin NeupaneNo ratings yet
- Effectiveness of Homoeopathic Treatment On Prostate Cancer-A Detailed Information To A Common ManDocument3 pagesEffectiveness of Homoeopathic Treatment On Prostate Cancer-A Detailed Information To A Common Manskandan s kumarNo ratings yet
- Abdominal Masses in The Newborn: Marshall Z. Schwartz, MD, and Donald B. Shaul, MDTDocument10 pagesAbdominal Masses in The Newborn: Marshall Z. Schwartz, MD, and Donald B. Shaul, MDTAditya Rahman RYNo ratings yet
- Homeopathic Heritage-Anorectal DisordersDocument6 pagesHomeopathic Heritage-Anorectal DisordersDhanya G NairNo ratings yet
- Male Reproductive System 1mittalDocument23 pagesMale Reproductive System 1mittalSAYMABANUNo ratings yet
- Nerves DistributionDocument9 pagesNerves Distributiondeargrace2512No ratings yet
- Health Assessment ON Genito Urinary System: Submitted To: Submitted byDocument16 pagesHealth Assessment ON Genito Urinary System: Submitted To: Submitted byAnanthibalaNo ratings yet
- The Type of Cancer SuspectedDocument20 pagesThe Type of Cancer SuspectedkdfhjfhfNo ratings yet
- Clinical Examination of Companion AnimalsDocument6 pagesClinical Examination of Companion AnimalsLouise Alysson OrtegaNo ratings yet
- Der Chi 2001Document19 pagesDer Chi 20013bood.3raqNo ratings yet
- BPH and Its Scope in HomeopathyDocument3 pagesBPH and Its Scope in HomeopathyEditor IJTSRDNo ratings yet
- Female Bladder Outlet Obstruction and Urethral ReconstructionFrom EverandFemale Bladder Outlet Obstruction and Urethral ReconstructionNikhil KhattarNo ratings yet
- Vancouver GuideDocument10 pagesVancouver Guidepravina praviNo ratings yet
- Female Reproductive System Assessment22Document12 pagesFemale Reproductive System Assessment22pravina praviNo ratings yet
- Alteration in Body TemperatureDocument19 pagesAlteration in Body Temperaturepravina praviNo ratings yet
- Research in Continuing Education Seminar Typed ContentDocument31 pagesResearch in Continuing Education Seminar Typed Contentpravina praviNo ratings yet
- L Anand Reseamh Sotmlar Annarnalai UniversityDocument3 pagesL Anand Reseamh Sotmlar Annarnalai Universitypravina praviNo ratings yet