You might also like
- Murillo de Oliveira Antunes 2020Document15 pagesMurillo de Oliveira Antunes 2020Asisten Lab TLPNo ratings yet
- SIRT1 Role in Cardiovascular BiologyDocument8 pagesSIRT1 Role in Cardiovascular Biologyfatimakh462No ratings yet
- Guia Esvs Manejo Evc 2015Document60 pagesGuia Esvs Manejo Evc 2015Steeven Ruilova Valle100% (1)
- JurnalDocument7 pagesJurnalFirmansyah FirmansyahNo ratings yet
- ESVS Thoracic Ds PDFDocument49 pagesESVS Thoracic Ds PDFFredy CarolNo ratings yet
- Sandercock 2011Document23 pagesSandercock 2011Gabriel FidelisNo ratings yet
- VT Guidelines PDFDocument74 pagesVT Guidelines PDFgabrimarteNo ratings yet
- Endogenous Cardiotonic SteroidsDocument30 pagesEndogenous Cardiotonic SteroidsSebastian NemethNo ratings yet
- Paro en Sepsis 2017Document8 pagesParo en Sepsis 2017Michelle RdgzNo ratings yet
- Central NDocument73 pagesCentral NrosianaNo ratings yet
- Clinica Chimica ActaDocument8 pagesClinica Chimica ActaErdelyi-Molnár ImolaNo ratings yet
- Cardio RenalDocument11 pagesCardio RenalAgung WistaraNo ratings yet
- AMBOSS 2021 ENAM Study GuideDocument49 pagesAMBOSS 2021 ENAM Study GuideMadeline DelgadoNo ratings yet
- Barreras en El Crebro en DesarrolloDocument19 pagesBarreras en El Crebro en DesarrolloAlvarez Flores GilmerNo ratings yet
- Fisher Syndrome and Bickerstaff Brainstem Encephalitis (Fisher-Bickerstaff Syndrome)Document9 pagesFisher Syndrome and Bickerstaff Brainstem Encephalitis (Fisher-Bickerstaff Syndrome)John AnastasiadesNo ratings yet
- Concise Histology - Leslie P Gartner & James L Hiatt (1E)Document353 pagesConcise Histology - Leslie P Gartner & James L Hiatt (1E)Subhashree Nayak94% (17)
- Journal of Arrhythmia: Ryan J. Koene, MD, Wayne O. Adkisson, MD, FACC, David G. Benditt, MD, FACC, FRCPC, FHRS, FESCDocument12 pagesJournal of Arrhythmia: Ryan J. Koene, MD, Wayne O. Adkisson, MD, FACC, David G. Benditt, MD, FACC, FRCPC, FHRS, FESCSI VENNo ratings yet
- Maximino Et Al (2013)Document13 pagesMaximino Et Al (2013)DavidNo ratings yet
- AO ASIF Principles in Spine SurgeryDocument253 pagesAO ASIF Principles in Spine SurgeryKhaled RahmanNo ratings yet
- Preview-9781498712811 A38165272Document20 pagesPreview-9781498712811 A38165272darrenNo ratings yet
- Park 2015Document7 pagesPark 2015pokharelriwaj82No ratings yet
- Guillenbare 3Document15 pagesGuillenbare 3indadzilarsyNo ratings yet
- Free Radicals and Antioxidants in Normal PhysiologicalDocument41 pagesFree Radicals and Antioxidants in Normal PhysiologicalleosabreuNo ratings yet
- The Immunoregulatory Function of Polyphenols - Implications in Cancer ImmunityDocument11 pagesThe Immunoregulatory Function of Polyphenols - Implications in Cancer ImmunitySusan OstosNo ratings yet
- Ingles 4 Tesis Abayomi SorinolaDocument154 pagesIngles 4 Tesis Abayomi SorinolaThe Almighty BelugaNo ratings yet
- Arasu Biofluid PDFDocument106 pagesArasu Biofluid PDFNoel Mahung MelendezNo ratings yet
- Stroke in Tuberculous MeningitisDocument9 pagesStroke in Tuberculous MeningitisCylla RevataNo ratings yet
- Inborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsFrom EverandInborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsNo ratings yet
- Drop Foot Degenerative Lumbar Spinal DiseaseDocument7 pagesDrop Foot Degenerative Lumbar Spinal DiseaseNovi NuariNo ratings yet
- Carotid ESVS 2018Document79 pagesCarotid ESVS 2018Ahmed ElmallahNo ratings yet
- Cardiac HypertrofiDocument18 pagesCardiac HypertrofiIndraNiagaNo ratings yet
- Textbook of Clinical NeurologyDocument374 pagesTextbook of Clinical Neurologykanuparthyj100% (9)
- Lo Ultimo en Alopecia AreataDocument10 pagesLo Ultimo en Alopecia AreataJohannes Bazán ÁlvarezNo ratings yet
- Cockayne Syndrome Clinical Features Source Elsevier SO 2017 (GGT904768966)Document15 pagesCockayne Syndrome Clinical Features Source Elsevier SO 2017 (GGT904768966)dai shujuanNo ratings yet
- Radiology of Non-Spinal Pain Procedures - M. Syed, A. Shaikh (Springer, 2011) WWDocument236 pagesRadiology of Non-Spinal Pain Procedures - M. Syed, A. Shaikh (Springer, 2011) WWcatalin calinNo ratings yet
- Flee Nor 2015Document67 pagesFlee Nor 2015Cosmin AndreiNo ratings yet
- Uti in WomanDocument6 pagesUti in WomanPrimasari DiahNo ratings yet
- Pharmacol Rev-2000-Kim-11-34Document24 pagesPharmacol Rev-2000-Kim-11-34De La Torre Corral UrielNo ratings yet
- 2019 ESC Guidelines For The Management of SVT Supplementary DataDocument10 pages2019 ESC Guidelines For The Management of SVT Supplementary DataElena CosminaNo ratings yet
- S16427e PDFDocument356 pagesS16427e PDFhuda ifandaNo ratings yet
- Analysing Seasonal Health DataDocument174 pagesAnalysing Seasonal Health DataIsmailNo ratings yet
- Ideomotor Apraxia: A Review: Lewis A. Wheaton, Mark HallettDocument10 pagesIdeomotor Apraxia: A Review: Lewis A. Wheaton, Mark HallettCamila MadridNo ratings yet
- Bioengineering Heart MuscleDocument23 pagesBioengineering Heart MuscleNina TandonNo ratings yet
- Cardiovascular ImagingDocument401 pagesCardiovascular ImagingRani Mulia100% (5)
- Endocrine Hypertension - Diagnosis and Treatment of Hormone-Induced Blood Pressure DisordersFrom EverandEndocrine Hypertension - Diagnosis and Treatment of Hormone-Induced Blood Pressure DisordersNo ratings yet
- Jurnal Stapilokokus OsteomielitisDocument27 pagesJurnal Stapilokokus OsteomielitisWahyuNo ratings yet
- Outcomes - English Version-Min 1Document96 pagesOutcomes - English Version-Min 1Loulou ShamsNo ratings yet
- Guidelines For The Diagnosis and Management of Syncope (Version 2009)Document41 pagesGuidelines For The Diagnosis and Management of Syncope (Version 2009)Radu AlexNo ratings yet
- IchthyosisDocument154 pagesIchthyosisprajnamitaNo ratings yet
- Foot Surgery Viewed Through The Prism of Comparative Anatomy From Normal To Useful 1St Edition Cyrille Cazeau Full ChapterDocument68 pagesFoot Surgery Viewed Through The Prism of Comparative Anatomy From Normal To Useful 1St Edition Cyrille Cazeau Full Chapterkendra.kimball418100% (6)
- AMBOSS PLE Study GuideDocument77 pagesAMBOSS PLE Study GuideFhai Escio100% (1)
- Jean Keeling, Anthony Busuttil Paediatric Forensic Medicine and PathologyDocument521 pagesJean Keeling, Anthony Busuttil Paediatric Forensic Medicine and PathologyMadul15No ratings yet
- Forensic Aspects of Complications Resulting From Cardiopulmonary ResuscitationDocument6 pagesForensic Aspects of Complications Resulting From Cardiopulmonary ResuscitationMadul15No ratings yet
- 1 s2.0 S1344622305001264 MainDocument8 pages1 s2.0 S1344622305001264 MainMadul15No ratings yet
- Anesthesia in Prolonged Dental Cases.8Document7 pagesAnesthesia in Prolonged Dental Cases.8Madul15No ratings yet
- Sudden Cardiac Death With Normal Heart: Molecular AutopsyDocument5 pagesSudden Cardiac Death With Normal Heart: Molecular AutopsyMadul15No ratings yet
- Forensic Pathological Investigation of Myocardial Hypoxia-Inducible Factor-1a, Erythropoietin and Vascular Endothelial Growth Factor in Cardiac DeathDocument9 pagesForensic Pathological Investigation of Myocardial Hypoxia-Inducible Factor-1a, Erythropoietin and Vascular Endothelial Growth Factor in Cardiac DeathMadul15No ratings yet
- Legal Medicine: A. LunaDocument4 pagesLegal Medicine: A. LunaMadul15No ratings yet
- Forensic Science International: Ugo Da Broi, Carlo MoreschiDocument5 pagesForensic Science International: Ugo Da Broi, Carlo MoreschiAlifiah Putri BaharuddinNo ratings yet
- Legal Medicine: Dong Zhao, Takaki Ishikawa, Li Quan, Tomomi Michiue, Bao-Li Zhu, Hitoshi MaedaDocument3 pagesLegal Medicine: Dong Zhao, Takaki Ishikawa, Li Quan, Tomomi Michiue, Bao-Li Zhu, Hitoshi MaedaMadul15No ratings yet
- Sudden Cardiac Death E Historical Perspectives: SciencedirectDocument6 pagesSudden Cardiac Death E Historical Perspectives: SciencedirectMadul15No ratings yet
- Forensic Science InternationalDocument7 pagesForensic Science InternationalMadul15No ratings yet
- Euthanasia Position PaperDocument26 pagesEuthanasia Position PaperDamon Copeland50% (2)
- Forensic Science International: S. Remmer, A. Kuudeberg, M. To Nisson, D. Lepik, M. Va LiDocument4 pagesForensic Science International: S. Remmer, A. Kuudeberg, M. To Nisson, D. Lepik, M. Va LiMadul15No ratings yet
- Forensic Science International: S. Remmer, A. Kuudeberg, M. To Nisson, D. Lepik, M. Va LiDocument4 pagesForensic Science International: S. Remmer, A. Kuudeberg, M. To Nisson, D. Lepik, M. Va LiMadul15No ratings yet
- Relationship Between Hopelessness and Ultimate SuiDocument7 pagesRelationship Between Hopelessness and Ultimate SuiMadul15No ratings yet
- II.1.5 Ethanol: by Kanako WatanabeDocument8 pagesII.1.5 Ethanol: by Kanako WatanabeMadul15No ratings yet
- Pathology and Genetics of Head and Neck TumoursDocument435 pagesPathology and Genetics of Head and Neck TumoursMonica MehendirattaNo ratings yet
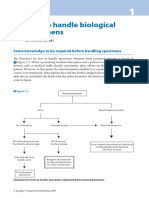
- I.1 How To Handle Biological Specimens: by Osamu SuzukiDocument7 pagesI.1 How To Handle Biological Specimens: by Osamu SuzukiMadul15No ratings yet
- Excess Mortality of Schizophrenia. A Meta-Analysis.: References ReprintsDocument8 pagesExcess Mortality of Schizophrenia. A Meta-Analysis.: References ReprintsMadul15No ratings yet
- I.3 Pitfalls and Cautions in Analysis of Drugs and PoisonsDocument8 pagesI.3 Pitfalls and Cautions in Analysis of Drugs and PoisonsMadul15No ratings yet
- I.3 Pitfalls and Cautions in Analysis of Drugs and PoisonsDocument8 pagesI.3 Pitfalls and Cautions in Analysis of Drugs and PoisonsMadul15No ratings yet
- II.1.4 Methanol and Formic AcidDocument11 pagesII.1.4 Methanol and Formic AcidMadul15No ratings yet
- II.1.1 Carbon MonoxideDocument9 pagesII.1.1 Carbon MonoxideMadul15No ratings yet
- II.1.1 Carbon MonoxideDocument9 pagesII.1.1 Carbon MonoxideMadul15No ratings yet
- II.1.4 Methanol and Formic AcidDocument11 pagesII.1.4 Methanol and Formic AcidMadul15No ratings yet
- II.1.5 Ethanol: by Kanako WatanabeDocument8 pagesII.1.5 Ethanol: by Kanako WatanabeMadul15No ratings yet
- I.9 Analysis of Chemical Warfare Agents and Their Related CompoundsDocument23 pagesI.9 Analysis of Chemical Warfare Agents and Their Related CompoundsJohn MillerNo ratings yet
- I.5 Detection MethodsDocument11 pagesI.5 Detection MethodsMadul15No ratings yet
- I.5 Detection MethodsDocument11 pagesI.5 Detection MethodsMadul15No ratings yet
- CellsDocument4 pagesCellscalustre2016No ratings yet
- NSTSE Class 3 2017 Part 4Document4 pagesNSTSE Class 3 2017 Part 4Shailendra YadavNo ratings yet
- The Human BrainDocument1 pageThe Human BrainedtxrsmNo ratings yet
- Mock Test Paper Class 4Document3 pagesMock Test Paper Class 4sukhvindersNo ratings yet
- Muscle and Fatpercentage of Lion and TigersDocument7 pagesMuscle and Fatpercentage of Lion and TigersMuhammed-Yusuf50% (2)
- Widoasti Putri Utami - 22010120410005 PDFDocument20 pagesWidoasti Putri Utami - 22010120410005 PDFdevaNo ratings yet
- Bukti ACCELERATION OF BONE FRACTURE HEALINGDocument18 pagesBukti ACCELERATION OF BONE FRACTURE HEALINGsanny silabanNo ratings yet
- Filtracion GlomerularDocument18 pagesFiltracion GlomerularNicole Jheny Raraz SosaNo ratings yet
- Origin and History of ETHOLOGY - Founders of EthologyDocument16 pagesOrigin and History of ETHOLOGY - Founders of Ethology7037Anant kumar prajapati100% (3)
- Lac Operon - Genetics-Essentials-Concepts-and-ConnectionsDocument15 pagesLac Operon - Genetics-Essentials-Concepts-and-ConnectionsDiandra AnnisaNo ratings yet
- Reconstruction of Defects Involving The Lip and ChinDocument17 pagesReconstruction of Defects Involving The Lip and ChinFabian Camelo OtorrinoNo ratings yet
- Unit 3 Plan - Grade 11 Biology - Transportation and Respiration - Michelle Romanuk - 7786294Document9 pagesUnit 3 Plan - Grade 11 Biology - Transportation and Respiration - Michelle Romanuk - 7786294api-536171687No ratings yet
- Anatomy Is The Study of The Structure of The Human Body:: Introduction To Anatomy: Anatomical TerminologyDocument9 pagesAnatomy Is The Study of The Structure of The Human Body:: Introduction To Anatomy: Anatomical TerminologyAj AquinoNo ratings yet
- Fenotipos DBP 2022Document19 pagesFenotipos DBP 2022Christian Isaac Rodriguez MoranNo ratings yet
- 10th Name The Following BiologyDocument11 pages10th Name The Following BiologyManoj ThakurNo ratings yet
- Connective Tissue StructureDocument8 pagesConnective Tissue StructureShael ZoletaNo ratings yet
- Epidermal Growth FactorDocument11 pagesEpidermal Growth FactorDanièle FeudjioNo ratings yet
- M 1 PPT-PDF XI Bio CH 7 Structural Organisation in AnimalsDocument39 pagesM 1 PPT-PDF XI Bio CH 7 Structural Organisation in Animalsamarendrar87No ratings yet
- Pain: Is It All in The Brain or The Heart?Document4 pagesPain: Is It All in The Brain or The Heart?KjellaNo ratings yet
- M2L1 Phonology and MorphologyDocument18 pagesM2L1 Phonology and MorphologyJJ BuicoNo ratings yet
- Pallor Mortis: 4 Stage of DeathDocument2 pagesPallor Mortis: 4 Stage of DeathAbegeil RadimaNo ratings yet
- The Pathophysiology of "Happy" Hypoglycemia: Casereport Open AccessDocument4 pagesThe Pathophysiology of "Happy" Hypoglycemia: Casereport Open Accessluandry medinaNo ratings yet
- 鄭淑鎂 - Dr. Lee's CA Side Effect Treatment (Part 1) (English)Document13 pages鄭淑鎂 - Dr. Lee's CA Side Effect Treatment (Part 1) (English)Bodhi SattvaNo ratings yet
- Markscheme: (209 Marks)Document24 pagesMarkscheme: (209 Marks)Michael WangNo ratings yet
- Alpha Amylase ExperimentDocument13 pagesAlpha Amylase ExperimentJessica BarcelonaNo ratings yet
- Posterior Triangle of NeckDocument47 pagesPosterior Triangle of NeckJuned LabbaiNo ratings yet
- Task 1Document2 pagesTask 1pancadewisNo ratings yet
- AP Psych 2.3 Notes - Nervous and Endocrine SystemDocument2 pagesAP Psych 2.3 Notes - Nervous and Endocrine SystemIan BurtNo ratings yet
- AnatomyDocument23 pagesAnatomyMiracle For NursesNo ratings yet
- Cyanexpert 130: Application SheetsDocument55 pagesCyanexpert 130: Application Sheets林圣贺No ratings yet