You might also like
- Remote Work Policy For (Company Name)Document3 pagesRemote Work Policy For (Company Name)Bee KayNo ratings yet
- COVID-19 Emergency Remote Work ProcedureDocument3 pagesCOVID-19 Emergency Remote Work ProcedureJosh SmithNo ratings yet
- Bahasa Inggris TugasDocument12 pagesBahasa Inggris TugasdayatNo ratings yet
- Lion Manpower Recruitment Policy SummaryDocument4 pagesLion Manpower Recruitment Policy SummaryDeepika AgnihotriNo ratings yet
- Internal Application for Leader ApprovalDocument2 pagesInternal Application for Leader Approvalevtim.edNo ratings yet
- Reporting Protocol 2023Document9 pagesReporting Protocol 2023mafeNo ratings yet
- Company Handbook OfficialDocument30 pagesCompany Handbook OfficialNeonNights HRNo ratings yet
- STATEMENT OF COMMITMENT KRAsDocument6 pagesSTATEMENT OF COMMITMENT KRAsAftab AalamNo ratings yet
- HR Onboarding Process in IndiaDocument6 pagesHR Onboarding Process in IndiaNeelam MandalNo ratings yet
- Descripción Completa Del EmpleoDocument5 pagesDescripción Completa Del EmpleoERIK EMMANUEL VAZQUEZ MARTINEZNo ratings yet
- Department of Biology and Marine Biology Policies and Procedures 2015-2016 I. General Office - (PDFDrive)Document44 pagesDepartment of Biology and Marine Biology Policies and Procedures 2015-2016 I. General Office - (PDFDrive)CrystalNo ratings yet
- Vacancy Circular CPE Valuation 2023Document6 pagesVacancy Circular CPE Valuation 2023jaswanthNo ratings yet
- WFH WaiverDocument4 pagesWFH WaiverMarc ResuelloNo ratings yet
- NYL WAH PolicyDocument6 pagesNYL WAH Policyvanuska sylesterNo ratings yet
- Media 327439 SMXXDocument5 pagesMedia 327439 SMXXCheena Vitug LabasanNo ratings yet
- Application For TransferDocument4 pagesApplication For TransferKhan Mohammad Mahmud HasanNo ratings yet
- Notification IBPS Deputy Manager PA To Director PostDocument8 pagesNotification IBPS Deputy Manager PA To Director PostRohitRajakNo ratings yet
- State Student COOPDocument6 pagesState Student COOPeisen20aNo ratings yet
- 2014-2015 Workstudy ApplicationDocument2 pages2014-2015 Workstudy ApplicationLupita V. MelchorNo ratings yet
- DEPED Online Application Guide for Teacher 1 PositionDocument17 pagesDEPED Online Application Guide for Teacher 1 PositionJaden Yanto AbreraNo ratings yet
- CINI - HR - Policy As On 140207Document44 pagesCINI - HR - Policy As On 140207sanyu1208No ratings yet
- Flexible Work Arrangement - Agreement FormDocument2 pagesFlexible Work Arrangement - Agreement FormDindo Arambala OjedaNo ratings yet
- WFH PolicyDocument3 pagesWFH Policyattiliasp60% (5)
- CINI - HR - Policy As On 140207Document44 pagesCINI - HR - Policy As On 140207Shanoo ShanNo ratings yet
- School Support Staff Application Form 1Document8 pagesSchool Support Staff Application Form 1Badiaa nonoNo ratings yet
- Journal-04Document1 pageJournal-04Shahnewaz ParvezNo ratings yet
- Other Employment ApplicationDocument2 pagesOther Employment Applicationzaki mubarrokNo ratings yet
- Internship PacketDocument23 pagesInternship Packetapi-307108598No ratings yet
- Sample Human Resources Policies, Checklists, Forms, and Procedures Policy Samples, Checklists, Forms, and ProceduresDocument5 pagesSample Human Resources Policies, Checklists, Forms, and Procedures Policy Samples, Checklists, Forms, and ProceduresNessa Motay CahapayNo ratings yet
- E-Recruitment Process in HRMSDocument4 pagesE-Recruitment Process in HRMSshabir135No ratings yet
- Recruitment & Selection Process-2Document18 pagesRecruitment & Selection Process-2Naila AnsariNo ratings yet
- DepEd Teacher 1 Hiring Guide: Online Application and Interview ProcessDocument24 pagesDepEd Teacher 1 Hiring Guide: Online Application and Interview ProcessOnin C. Opeña0% (1)
- Temporary Remote Work Requests 2021Document1 pageTemporary Remote Work Requests 2021Martin HellNo ratings yet
- Systems Administrator Business Systems AnalystDocument3 pagesSystems Administrator Business Systems AnalystPeter L. MontezNo ratings yet
- Recruitment of Officers and Executives in Cent Bank Home Finance Limited - 2015-16Document10 pagesRecruitment of Officers and Executives in Cent Bank Home Finance Limited - 2015-16JeshiNo ratings yet
- Remote Work Letter of AgreementDocument4 pagesRemote Work Letter of AgreementN Sudheer RêddyNo ratings yet
- 12 - Chapter 4 PDFDocument43 pages12 - Chapter 4 PDFJaydev JoshiNo ratings yet
- FFWO Employee Request Form - Sample - 3Document3 pagesFFWO Employee Request Form - Sample - 3Puji ApriliantimayaNo ratings yet
- Bio Metric Policy for NIU EmployeesDocument4 pagesBio Metric Policy for NIU EmployeesniteshvnairNo ratings yet
- Payroll Records and Security ProceduresDocument19 pagesPayroll Records and Security ProceduresNiomi Golrai100% (1)
- The Unit DNI AssignmentDocument4 pagesThe Unit DNI AssignmentAhmed ul BariNo ratings yet
- Recruitment Process Rev1Document3 pagesRecruitment Process Rev1vs176975No ratings yet
- US Census Bureau Job: Assistant Manager For TechnologyDocument8 pagesUS Census Bureau Job: Assistant Manager For TechnologyOffice on Latino Affairs (OLA)No ratings yet
- Administrative Clerk II Jobs in BreaDocument2 pagesAdministrative Clerk II Jobs in BreaNattymanNo ratings yet
- Employee Referal Program PolicyDocument6 pagesEmployee Referal Program PolicyAanchal chopraNo ratings yet
- Date: March 27, 2021 To: To All Managers From: HR Department Memo No. Subject:: Asya Business Continuity For EcqDocument3 pagesDate: March 27, 2021 To: To All Managers From: HR Department Memo No. Subject:: Asya Business Continuity For EcqRoseanne CarsolaNo ratings yet
- Prospective ApplicantsDocument3 pagesProspective Applicantsukyo0801No ratings yet
- Vacancy Announcement - Management Data AnalystDocument4 pagesVacancy Announcement - Management Data Analystpmakenya systemNo ratings yet
- BSBHRM529 Task TwoDocument7 pagesBSBHRM529 Task TwoMade BagusNo ratings yet
- Hiring PolicyDocument5 pagesHiring PolicyPrachi RajputNo ratings yet
- Date: March 28, 2021 To: To All Department Heads / Managers From: HR Department Memo No. Subject:: Asya Business Continuity For EcqDocument5 pagesDate: March 28, 2021 To: To All Department Heads / Managers From: HR Department Memo No. Subject:: Asya Business Continuity For EcqRoseanne CarsolaNo ratings yet
- Deped Citizens Charter'Document78 pagesDeped Citizens Charter'Nom-de Plume67% (3)
- Employment Exit ChecklistDocument2 pagesEmployment Exit ChecklistokulluocenNo ratings yet
- HR Operations ManualDocument40 pagesHR Operations Manualbook xpert1No ratings yet
- Sitxhrm002 0003002652Document11 pagesSitxhrm002 0003002652Jasmeet LotaNo ratings yet
- Performance EmployeePerformanceAppraisalDocument6 pagesPerformance EmployeePerformanceAppraisalGeetanjali Geet100% (1)
- Terms and Conditions for ReceiptDocument3 pagesTerms and Conditions for ReceiptatozdhiyanesNo ratings yet
- Leave Policy - GTSDocument7 pagesLeave Policy - GTSSupreet SinghNo ratings yet
- Administrative Procedures and ManagementFrom EverandAdministrative Procedures and ManagementRating: 5 out of 5 stars5/5 (1)
- Philam Plans Not Liable Due to Concealment of Medical HistoryDocument2 pagesPhilam Plans Not Liable Due to Concealment of Medical HistoryKris GaoatNo ratings yet
- The Manila Hotel Corp. v. NLRCDocument2 pagesThe Manila Hotel Corp. v. NLRCKris GaoatNo ratings yet
- Antonia Maranan vs. Pascual PerezDocument2 pagesAntonia Maranan vs. Pascual PerezKris GaoatNo ratings yet
- Agra Law CasesDocument2 pagesAgra Law CasesKris GaoatNo ratings yet
- Saudi Arabian Airlines v. Rebesencio, Adiong, Cristobal & CruzDocument3 pagesSaudi Arabian Airlines v. Rebesencio, Adiong, Cristobal & CruzKris GaoatNo ratings yet
- Puyat vs. ZabarteDocument2 pagesPuyat vs. ZabarteKris GaoatNo ratings yet
- Zamora v. QuinanDocument2 pagesZamora v. QuinanKris GaoatNo ratings yet
- THE Labor Code of The PhilippinesDocument7 pagesTHE Labor Code of The PhilippinesKris GaoatNo ratings yet
- LTD ReviewerDocument58 pagesLTD ReviewerKris GaoatNo ratings yet
- Law On Sales - Digested CasesDocument135 pagesLaw On Sales - Digested Casesangelikaroman90% (40)
- 1 NREL ReviewerDocument16 pages1 NREL Reviewer'Joshua Crisostomo'No ratings yet
- 1 NREL ReviewerDocument16 pages1 NREL Reviewer'Joshua Crisostomo'No ratings yet
- Antonia Maranan vs. Pascual PerezDocument2 pagesAntonia Maranan vs. Pascual PerezKris GaoatNo ratings yet
- Welcome To EMAPTA: Login To Your ESP For Daily Attendance RecordDocument6 pagesWelcome To EMAPTA: Login To Your ESP For Daily Attendance RecordKris GaoatNo ratings yet
- Land, Titles, and Deeds ReviewerDocument13 pagesLand, Titles, and Deeds ReviewerVictoria Denise MonteNo ratings yet
- Sales (De Leon)Document737 pagesSales (De Leon)Bj Carido100% (7)
- LTD Module 1Document4 pagesLTD Module 1Kris GaoatNo ratings yet
- Sales Rabanes Reviewer 2017 PDFDocument30 pagesSales Rabanes Reviewer 2017 PDFJeferson GrishamNo ratings yet
- Baclayon v. Mutia (1984)Document2 pagesBaclayon v. Mutia (1984)Angelika ParkNo ratings yet
- Myreviewer Notes Property 2013 08 02 PDFDocument17 pagesMyreviewer Notes Property 2013 08 02 PDFJade LorenzoNo ratings yet
- Labor Relations Reviewer Elah V. Definitions: Duty To Bargain CollectivelyDocument12 pagesLabor Relations Reviewer Elah V. Definitions: Duty To Bargain CollectivelyKris GaoatNo ratings yet
- Up Law Boc 2016 - Legal and Judicial Ethics Reviewer PDFDocument109 pagesUp Law Boc 2016 - Legal and Judicial Ethics Reviewer PDFGeraldine Gallaron - Casipong100% (6)
- Political LawDocument364 pagesPolitical LawJingJing Romero100% (99)
- CRIMINAL LAW REVIEW BOOK IIDocument174 pagesCRIMINAL LAW REVIEW BOOK IIRose Ann CayabanNo ratings yet
- Memory Aid in Labor LawDocument27 pagesMemory Aid in Labor LawDane Pauline AdoraNo ratings yet
- Agpalo Legal Ethics Reviewer PDFDocument87 pagesAgpalo Legal Ethics Reviewer PDFGerald Hernandez100% (56)
- Digested CasesDocument38 pagesDigested CasesJaelein Nicey A. Monteclaro100% (1)
- Crim 2 Reviewer PDFDocument34 pagesCrim 2 Reviewer PDFPauline Villanueva-YapNo ratings yet
- Constitutional Law 2 REVIEWERDocument18 pagesConstitutional Law 2 REVIEWERKris Gaoat100% (4)
- 2.4 Static Pressure Spreadsheet 1Document4 pages2.4 Static Pressure Spreadsheet 1Swapnil Pratap SinghNo ratings yet
- Coverage and Profiling For Real-Time Tiny KernelsDocument6 pagesCoverage and Profiling For Real-Time Tiny Kernelsanusree_bhattacharjeNo ratings yet
- Quiz II - Company MissionDocument4 pagesQuiz II - Company MissionSuraj SapkotaNo ratings yet
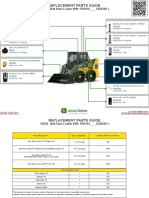
- 312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideDocument3 pages312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideNelson Andrade VelasquezNo ratings yet
- State Board of Education Memo On Broward County (Oct. 4, 2021)Document40 pagesState Board of Education Memo On Broward County (Oct. 4, 2021)David SeligNo ratings yet
- CSC V CADocument2 pagesCSC V CAAllen GrajoNo ratings yet
- Judicial Watch Vs State Dept Stephen Mull DepositionDocument415 pagesJudicial Watch Vs State Dept Stephen Mull DepositionThe Conservative Treehouse100% (1)
- Cambridge IGCSE: PHYSICS 0625/62Document12 pagesCambridge IGCSE: PHYSICS 0625/62yuNo ratings yet
- Tesco AnalysisDocument12 pagesTesco Analysisdanny_wch7990No ratings yet
- Kick Control: BY: Naga Ramesh D. Assistant Professor Petroleum Engineering Dept. KlefDocument13 pagesKick Control: BY: Naga Ramesh D. Assistant Professor Petroleum Engineering Dept. Klefavula43No ratings yet
- Empowerment Technologies Week 1-2 - Final Term: Prepared By: Mr. Jake Indico Edited By: Ms. Shaira G. RaquilDocument5 pagesEmpowerment Technologies Week 1-2 - Final Term: Prepared By: Mr. Jake Indico Edited By: Ms. Shaira G. RaquilJustine Evasco RubiaNo ratings yet
- Remote Environment: - Concern The Nature and Direction of Economy in Which A Firm Operates - Types of FactorsDocument27 pagesRemote Environment: - Concern The Nature and Direction of Economy in Which A Firm Operates - Types of FactorsmikiyingNo ratings yet
- ZeeVee ZVPro Quick Start GuideDocument2 pagesZeeVee ZVPro Quick Start GuideDavid WardNo ratings yet
- Excel calendarDocument28 pagesExcel calendarThanh LêNo ratings yet
- Violence ADocument236 pagesViolence AEndry AbidinNo ratings yet
- Newspaper Layout DummyDocument1 pageNewspaper Layout Dummy1w2e3r4t5y100% (9)
- IELTS PART 1 (Autoguardado)Document8 pagesIELTS PART 1 (Autoguardado)CARLOS CAICEDONo ratings yet
- PR100 Locks With Aperio Wireless Technology: Key FeaturesDocument2 pagesPR100 Locks With Aperio Wireless Technology: Key FeaturesMay SamboNo ratings yet
- Nitro2 User Manual v2.24 PDFDocument29 pagesNitro2 User Manual v2.24 PDFReifesxd ProNo ratings yet
- Assignment Number 2Document4 pagesAssignment Number 2Elson TalotaloNo ratings yet
- Yaskawa Ac Servo Drives & Controllers PDFDocument40 pagesYaskawa Ac Servo Drives & Controllers PDFNur CholisNo ratings yet
- Theories of EntrepreneurshipDocument3 pagesTheories of EntrepreneurshipIla Mehrotra Anand80% (5)
- Allison - Dp-8000 - Manual de Servicio - Pag-390Document390 pagesAllison - Dp-8000 - Manual de Servicio - Pag-390Manuales De Maquinaria Jersoncat100% (1)
- Signed-Off Komunikasyon-at-Pananaliksik11 q1 m2 - Konseptong-Pangwika v3 PDFDocument24 pagesSigned-Off Komunikasyon-at-Pananaliksik11 q1 m2 - Konseptong-Pangwika v3 PDFChristian Ocon100% (1)
- BSBPMG534 Task 2 - V2.4Document9 pagesBSBPMG534 Task 2 - V2.4Anoosha MazharNo ratings yet
- Optex Vibro DatasheetDocument2 pagesOptex Vibro DatasheetGabriel ChiriacNo ratings yet
- +1 TM Slow Learner Material For Reduced Portion 2021-22Document55 pages+1 TM Slow Learner Material For Reduced Portion 2021-22Prasanth Prasanth100% (2)
- The I NewspaperDocument60 pagesThe I Newspaperfagner barretoNo ratings yet
- Systematic Review of The Market Wide Herding Behavior in Asian RegionDocument9 pagesSystematic Review of The Market Wide Herding Behavior in Asian RegionIJAR JOURNALNo ratings yet
- ConclusionDocument1 pageConclusionSAVITHRINo ratings yet