You might also like
- RESEARCH MWTHODS M.ADocument11 pagesRESEARCH MWTHODS M.ADacosta FlectureNo ratings yet
- Peripheral Arterial Disease PDFDocument1 pagePeripheral Arterial Disease PDFpravin narkhedeNo ratings yet
- Jurnal Subkonjungtiva BleedingDocument3 pagesJurnal Subkonjungtiva BleedingPuetri 'Poe' SaptlyaNo ratings yet
- Teknik Operasi Splenektomi 2Document31 pagesTeknik Operasi Splenektomi 2sphericalfaNo ratings yet
- Infeksi Saluran KemihDocument35 pagesInfeksi Saluran KemihLestari Amelia AdmNo ratings yet
- Anatomi Mata CoassDocument41 pagesAnatomi Mata CoassSatria BuanaNo ratings yet
- Jurnal Unilateral Cleft LipDocument11 pagesJurnal Unilateral Cleft LipTriasnidaNo ratings yet
- VMware KB - Sample Configuration of Virtual Switch VLAN Tagging (VST ModeDocument4 pagesVMware KB - Sample Configuration of Virtual Switch VLAN Tagging (VST ModecorpacmNo ratings yet
- Referat Osteogenesis ImperfectaDocument21 pagesReferat Osteogenesis ImperfectaArdhian RamadhanNo ratings yet
- Referat OsteomielitisDocument22 pagesReferat OsteomielitisDexel Putra Simbolon100% (1)
- Olanzapine Vs AripiprazoleDocument8 pagesOlanzapine Vs AripiprazoleDivaviyaNo ratings yet
- MESSDocument9 pagesMESStaufik sofistiawanNo ratings yet
- Rupture Tendon Digiti III, IV, V Manus Sinistra Vulnus Laceratum Wrist Joint SinistraDocument13 pagesRupture Tendon Digiti III, IV, V Manus Sinistra Vulnus Laceratum Wrist Joint SinistraNubhy NubNo ratings yet
- Laporan Kasus Home Visit Hemoroid Interna - CoverDocument4 pagesLaporan Kasus Home Visit Hemoroid Interna - CoverSarah Humaira DennisonNo ratings yet
- Tutorial Kasus: AppendisitisDocument50 pagesTutorial Kasus: Appendisitiseruza hiwatariNo ratings yet
- Vesicolithiasis BSHDocument24 pagesVesicolithiasis BSHBobby Faisyal RakhmanNo ratings yet
- Fraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapDocument26 pagesFraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapUmi YatunNo ratings yet
- Antibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisDocument7 pagesAntibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisTias SubagioNo ratings yet
- Cervical Spine InjuriesDocument18 pagesCervical Spine InjuriesAnnapurna DangetiNo ratings yet
- Fracture CrurisDocument44 pagesFracture CrurisAnonymous turPUJtErNo ratings yet
- Tokyo Guidelines 2018 Flowchart For The Management of Acute CholecystitisDocument43 pagesTokyo Guidelines 2018 Flowchart For The Management of Acute Cholecystitisfranciscomejia14835No ratings yet
- Pityriasis Rosea - Background, Pathophysiology, EtiologyDocument4 pagesPityriasis Rosea - Background, Pathophysiology, EtiologysyahrulroziNo ratings yet
- Fraktur Dan Infeksi TulangDocument25 pagesFraktur Dan Infeksi TulangAnonymous HAbhRTs2TfNo ratings yet
- HEMOROIDDocument29 pagesHEMOROIDDanang Aryo PinujiNo ratings yet
- Craniotomy FlapsDocument41 pagesCraniotomy FlapsKaramsi Gopinath NaikNo ratings yet
- Referat Radiologi Fraktur AntebrachiiDocument3 pagesReferat Radiologi Fraktur AntebrachiiAnita Sari PutriiNo ratings yet
- Referat Skleritis PDFDocument25 pagesReferat Skleritis PDFDevi Melissa RiupassaNo ratings yet
- White Island in The Red SeaDocument1 pageWhite Island in The Red SeaIndach RatnaNo ratings yet
- Anatomy Fisiologi Spine LumbosacralDocument27 pagesAnatomy Fisiologi Spine LumbosacraloyomziicNo ratings yet
- Askep Atresia EsophagusDocument18 pagesAskep Atresia EsophagusKhoLisoh Sae Anugrah100% (1)
- ClubfootDocument30 pagesClubfootdrusmanjamilhcmdNo ratings yet
- Tata Kelola DM Di FKTPDocument29 pagesTata Kelola DM Di FKTPRSTN BoalemoNo ratings yet
- 11 - 206memahami DispareuniaDocument8 pages11 - 206memahami DispareuniaResti Puteri Apriyuslim0% (1)
- Nervus Laryngeus RecurrensDocument5 pagesNervus Laryngeus RecurrensAri Julian SaputraNo ratings yet
- LONG CASE Luka BakarDocument16 pagesLONG CASE Luka BakarAfiazka LuthfitaNo ratings yet
- Guildelines For Hiv Testing NacoDocument165 pagesGuildelines For Hiv Testing NacoNagendra Singh BeniwalNo ratings yet
- Colonic Volvulus: Disusun Oleh: Dhea Faizia Tasya (2110221036) Pembimbing: Dr. Yulia Rachmawati, Sp. Rad (K)Document25 pagesColonic Volvulus: Disusun Oleh: Dhea Faizia Tasya (2110221036) Pembimbing: Dr. Yulia Rachmawati, Sp. Rad (K)Dhea Faizia TasyaNo ratings yet
- Preface: - Fracture Discontinuity of The BoneDocument8 pagesPreface: - Fracture Discontinuity of The BoneWonderCatNo ratings yet
- Tugas MSCT Rhino 2 Scan Rikha FixDocument29 pagesTugas MSCT Rhino 2 Scan Rikha FixRikha LiemiyahNo ratings yet
- Dr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTDocument51 pagesDr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTCOVID RSHJNo ratings yet
- Karakteristik Penderita DM Dengan Ulkus Diabetik Di RSUD Dr. M. Haulussy Ambon Tahun 2011-2013Document20 pagesKarakteristik Penderita DM Dengan Ulkus Diabetik Di RSUD Dr. M. Haulussy Ambon Tahun 2011-2013musculussNo ratings yet
- Presentation LLD FarzandDocument44 pagesPresentation LLD Farzanddrakkashmiri100% (1)
- Journal Reading The Drowning IndexDocument5 pagesJournal Reading The Drowning IndexYuliasminde SofyanaNo ratings yet
- Fix - Laporan Kasus VesikolitiasisDocument11 pagesFix - Laporan Kasus VesikolitiasisHeri SatryawanNo ratings yet
- Aldo Febriananto Kurniawan 22010112140205 Lap - Kti Bab ViiDocument19 pagesAldo Febriananto Kurniawan 22010112140205 Lap - Kti Bab ViiAfrilia ShafiraNo ratings yet
- GestosisDocument12 pagesGestosisravannofanizzaNo ratings yet
- Congenital Adrenal HyperplasiaDocument2 pagesCongenital Adrenal HyperplasiaesyNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- Daftar Nama Pendataan Pembimbing BedahDocument6 pagesDaftar Nama Pendataan Pembimbing Bedahegi lewisNo ratings yet
- De La Maza, Maite Sainz, MD, Phd. Scleritis. 2010. (Diakses Tanggal)Document1 pageDe La Maza, Maite Sainz, MD, Phd. Scleritis. 2010. (Diakses Tanggal)fa dliNo ratings yet
- PPK Perdoski 2017 Skabies (English)Document3 pagesPPK Perdoski 2017 Skabies (English)yumizoneNo ratings yet
- Ankle Instability (Full) 2Document20 pagesAnkle Instability (Full) 2dwi rezki amaliaNo ratings yet
- Bebas Remedial TraumaDocument11 pagesBebas Remedial TraumaLilac MintNo ratings yet
- Emailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFDocument38 pagesEmailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFHaykal FathirrahmanNo ratings yet
- LimfadenopatiDocument8 pagesLimfadenopatiZulkarnain PrakosoNo ratings yet
- Stenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandStenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hay2014 PDFDocument5 pagesHay2014 PDFsuci lestariNo ratings yet
- Biology 11 01797Document13 pagesBiology 11 01797alejandra queenNo ratings yet
- Management of Disease and Disorders by Prebiotics and Probiotic Therapy: Probiotics in Bacterial VaginosisDocument9 pagesManagement of Disease and Disorders by Prebiotics and Probiotic Therapy: Probiotics in Bacterial Vaginosissiska tiaraNo ratings yet
- Bacterial VaginosisDocument11 pagesBacterial VaginosisMuh. Idham RahmanNo ratings yet
- Gynecologic Infections: Genet Gebremedhin (MD) Assistant Prof of Gynecology & Obstetrics University of Gondar March 4 2012Document91 pagesGynecologic Infections: Genet Gebremedhin (MD) Assistant Prof of Gynecology & Obstetrics University of Gondar March 4 2012Degefaw BikoyNo ratings yet
- Body Transportation After Homicides Offender and Offense CharacteristicsDocument4 pagesBody Transportation After Homicides Offender and Offense CharacteristicsIntan PermataNo ratings yet
- Aggression and Violent Behavior: $Jjuhvvlrqdqg9Lrohqw%HkdylruDocument7 pagesAggression and Violent Behavior: $Jjuhvvlrqdqg9Lrohqw%HkdylruIntan PermataNo ratings yet
- Schweitzer 2019Document12 pagesSchweitzer 2019Intan PermataNo ratings yet
- Cold Case Homicides: DNA Testing of Retained Autopsy Sexual Assault SmearsDocument5 pagesCold Case Homicides: DNA Testing of Retained Autopsy Sexual Assault SmearsIntan PermataNo ratings yet
- Malpositions and Malpresentations of The Fetal Head: ReviewDocument9 pagesMalpositions and Malpresentations of The Fetal Head: ReviewIntan PermataNo ratings yet
- Hiperemesis GravidarumDocument8 pagesHiperemesis GravidarumIntan PermataNo ratings yet
- Partus LamaDocument4 pagesPartus LamaIntan PermataNo ratings yet
- Disproporsi Kepala PanggulDocument14 pagesDisproporsi Kepala PanggulIntan PermataNo ratings yet
- RektokelDocument13 pagesRektokelIntan PermataNo ratings yet
- Practice: Superficial Thrombophlebitis (Superficial Venous Thrombosis)Document4 pagesPractice: Superficial Thrombophlebitis (Superficial Venous Thrombosis)Intan PermataNo ratings yet
- DistosiaDocument12 pagesDistosiaIntan PermataNo ratings yet
- HBMT 4103Document34 pagesHBMT 4103Donna OngNo ratings yet
- Geometry Practice Test 7 - ACT PROBLEMSDocument7 pagesGeometry Practice Test 7 - ACT PROBLEMSCarlos OrtizNo ratings yet
- Ata 38 MD-80Document18 pagesAta 38 MD-80JOSUÉ CABRERANo ratings yet
- LABP0311Document4 pagesLABP0311Mr. JalilNo ratings yet
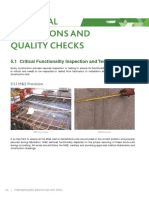
- Critical Inspections and Quality ChecksDocument8 pagesCritical Inspections and Quality ChecksalfieNo ratings yet
- Suggested Answers To Practical Workbook: CH 7 Gas Exchange in HumansDocument31 pagesSuggested Answers To Practical Workbook: CH 7 Gas Exchange in HumansCharmine HolmesNo ratings yet
- Bukh DV 36 SmeDocument5 pagesBukh DV 36 SmeTullio OpattiNo ratings yet
- Day 1 Part of Speech, Noun, PronounDocument18 pagesDay 1 Part of Speech, Noun, PronounZulfan FirdausNo ratings yet
- Design Education Through Toy Design OldDocument12 pagesDesign Education Through Toy Design Oldvalentina zigangirovaNo ratings yet
- Session 1 Goal and Function of FinanceDocument59 pagesSession 1 Goal and Function of FinanceMayank PatelNo ratings yet
- Identity and Travel Document FraudDocument2 pagesIdentity and Travel Document FraudPinas SayaNo ratings yet
- Project Report On Multi Speciality Hospital (70 Beds)Document5 pagesProject Report On Multi Speciality Hospital (70 Beds)EIRI Board of Consultants and PublishersNo ratings yet
- Star Method Interview Prep Packet 2020Document11 pagesStar Method Interview Prep Packet 2020snvales92No ratings yet
- Barangay Livelihood CommitteeDocument3 pagesBarangay Livelihood CommitteeMary Jane Licmo-anNo ratings yet
- Africa in American Media:: A Content Analysis of Magazine's Portrayal of Africa, 1988-2006 By: Stella Maris KunihiraDocument11 pagesAfrica in American Media:: A Content Analysis of Magazine's Portrayal of Africa, 1988-2006 By: Stella Maris KunihiraEthanNo ratings yet
- Foundation of GuidanceDocument17 pagesFoundation of GuidanceFroilan FerrerNo ratings yet
- Chapter - I: Introduction: Part - I: Nature and Methodology of EconomicsDocument8 pagesChapter - I: Introduction: Part - I: Nature and Methodology of EconomicsshafistoreNo ratings yet
- Shmoop Summary One Flew Over The Cuckoo's NestDocument61 pagesShmoop Summary One Flew Over The Cuckoo's NestDaniela Torres Noriega100% (1)
- Grade 8 Maths Algebraic Expressions and Exponents MCQDocument4 pagesGrade 8 Maths Algebraic Expressions and Exponents MCQa1b3doNo ratings yet
- RealTime 1st Quarter Student GuideDocument28 pagesRealTime 1st Quarter Student GuideHenry Ng'honzelaNo ratings yet
- Regionalization Peru 5thversionDocument31 pagesRegionalization Peru 5thversionRobertNo ratings yet
- Beverage Brochure EnglishDocument16 pagesBeverage Brochure Englishsalicurri0% (1)
- Epa Facilities Manual Vol 3 Facilities SafetyDocument43 pagesEpa Facilities Manual Vol 3 Facilities Safetykeneth john manayagaNo ratings yet
- Fujifilm Fujinon Catalogue 2023Document17 pagesFujifilm Fujinon Catalogue 2023kadir benklitasNo ratings yet
- CV of HASAN MAHAMUDDocument3 pagesCV of HASAN MAHAMUDMuhammad Azharul HannanNo ratings yet
- Week 1 IntroductionDocument13 pagesWeek 1 Introductionobai AlhwimelNo ratings yet
- Cp05-03-Mmc-Mst-Mec-0019 Rev.01Document55 pagesCp05-03-Mmc-Mst-Mec-0019 Rev.01Mohamed AshrafNo ratings yet
- Catalog PDFDocument226 pagesCatalog PDFAndika Arihta Pasaribu100% (1)