You might also like
- Physical Assessment of Normal Pregnant ClientDocument24 pagesPhysical Assessment of Normal Pregnant ClientGhilah MaeNo ratings yet
- GDMDocument11 pagesGDMNikki GarlejoNo ratings yet
- CHN Case Analysis Case ScenarioDocument7 pagesCHN Case Analysis Case ScenarioNathalie kate petallarNo ratings yet
- Prenatal CareDocument64 pagesPrenatal CareAmy LalringhluaniNo ratings yet
- I. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsDocument5 pagesI. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsSophia Loraine Dorone Jesura100% (1)
- Assessment of Preschooler and SchoolerDocument49 pagesAssessment of Preschooler and SchoolerNancy SamuelNo ratings yet
- Malpositionslideshare 131213102326 Phpapp02Document33 pagesMalpositionslideshare 131213102326 Phpapp02santhanalakshmi100% (1)
- Family Planning MethodDocument105 pagesFamily Planning MethodKailash NagarNo ratings yet
- Terminology CHNDocument4 pagesTerminology CHNKailash NagarNo ratings yet
- Breech Case StudyDocument31 pagesBreech Case StudyRed Williams100% (1)
- Medical & Nursing Management For Cervical CancerDocument11 pagesMedical & Nursing Management For Cervical CancerPromise Encinares100% (1)
- Case Study PIHDocument26 pagesCase Study PIHChen OmbrosaNo ratings yet
- Postnatal ExaminationDocument19 pagesPostnatal ExaminationAlpha100% (1)
- Nursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionDocument2 pagesNursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionVincent Paul SantosNo ratings yet
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- Teaching Plan For Proper Breast Feeding Begh ErDocument7 pagesTeaching Plan For Proper Breast Feeding Begh ErAmira Fatmah QuilapioNo ratings yet
- Minggu 5 LP Hiperemesis GravidarumDocument16 pagesMinggu 5 LP Hiperemesis GravidarumMuhammad PanduNo ratings yet
- Diet For Pregnancy and Lactating WomenDocument49 pagesDiet For Pregnancy and Lactating WomenrjNo ratings yet
- Group 2. Ectopic PregnancyDocument61 pagesGroup 2. Ectopic PregnancyIvan Laurentine Aceret100% (1)
- CASE ANALYSIS Ectopic Pregnancy Part 1Document10 pagesCASE ANALYSIS Ectopic Pregnancy Part 1Diane Celine SantianoNo ratings yet
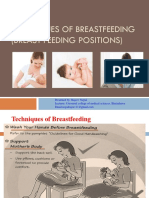
- Technique of Breast Feeding (Position of Breast Feeding)Document17 pagesTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalNo ratings yet
- Case Study On Observation and Newborn CareDocument38 pagesCase Study On Observation and Newborn CarePiyush Dutta100% (2)
- Community Health Nursing - Case PresentationDocument45 pagesCommunity Health Nursing - Case PresentationLev Jasper Alcantara Blanco100% (8)
- Obesity Prevention and Education For School Nurses Community Health NursingDocument66 pagesObesity Prevention and Education For School Nurses Community Health NursingGabrielaNo ratings yet
- Newborn Case StudyDocument16 pagesNewborn Case StudyErl Joy Montaño Cañete0% (1)
- Intrauterine Growth RestrictionDocument21 pagesIntrauterine Growth Restrictionمصطفى محمدNo ratings yet
- Case Study NursingDocument18 pagesCase Study Nursingdaisy dizaNo ratings yet
- Failure To Thrive (FTT)Document23 pagesFailure To Thrive (FTT)Endrow Francisco100% (1)
- Bsn2c Dalipe de Los Reyes NDT Lab Activity Dietary ModificationsDocument2 pagesBsn2c Dalipe de Los Reyes NDT Lab Activity Dietary ModificationsXeyanNo ratings yet
- Teaching Plan Breast Feeding 270Document8 pagesTeaching Plan Breast Feeding 270Franco ObedozaNo ratings yet
- Discharge Planning FinalDocument5 pagesDischarge Planning FinalRose AnnNo ratings yet
- Diet Modification and Diet TherapyDocument76 pagesDiet Modification and Diet TherapyFatima Ysabelle Marie RuizNo ratings yet
- Ethico-Moral Principles and Cultural/Spiritual Preferences: By: Kim Angelique TinoDocument14 pagesEthico-Moral Principles and Cultural/Spiritual Preferences: By: Kim Angelique TinoPRIMA, CAMILLE JOY ROSELANo ratings yet
- Chapter24 PDFDocument43 pagesChapter24 PDFCindy MaslagNo ratings yet
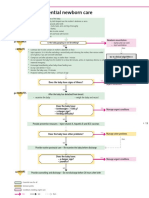
- Algorithm 2: Essential Newborn Care: BirthDocument1 pageAlgorithm 2: Essential Newborn Care: BirthGabriel Anthony ArtizaNo ratings yet
- Family Case StudyDocument58 pagesFamily Case Studyrodcyruskent100% (1)
- NCM119ClinicalLab Pediatric Ward Pneumonia Case Study Group 4Document40 pagesNCM119ClinicalLab Pediatric Ward Pneumonia Case Study Group 4Allysa MacalinoNo ratings yet
- Discharge PlanDocument2 pagesDischarge PlanJude Labajo100% (1)
- Nutrition During InfancyDocument48 pagesNutrition During InfancyMabelle Blancada ConsultaNo ratings yet
- Gary Fending For HimselfDocument3 pagesGary Fending For HimselfPrincess Levie CenizaNo ratings yet
- Ob Case Presentation GDMDocument78 pagesOb Case Presentation GDMmarsphinx50% (4)
- Nursing Care PlanDocument6 pagesNursing Care PlanFrances CalaraNo ratings yet
- Anatomy and Physiology of Breech PresentationDocument2 pagesAnatomy and Physiology of Breech Presentationeskempertus0% (2)
- Discharge PlanningDocument3 pagesDischarge PlanningAlex Marie100% (2)
- Case Study - GDMDocument5 pagesCase Study - GDMRomeo ReyesNo ratings yet
- Presentaton On LBW BabyDocument59 pagesPresentaton On LBW Babycharanjit kaur100% (1)
- Care of A NewbornDocument54 pagesCare of A Newbornzachariah nkhukuzaliraNo ratings yet
- Week 2 Rle ActivityDocument3 pagesWeek 2 Rle ActivityMICHELLE BIANCA PATRICE CRUZNo ratings yet
- Implementing Family Care PlanDocument74 pagesImplementing Family Care PlanMarlon Glorioso II100% (2)
- Chapter 24: Nursing Care of A Family During A Surgical Intervention For BirthDocument22 pagesChapter 24: Nursing Care of A Family During A Surgical Intervention For BirthAlyssaGrandeMontimorNo ratings yet
- New Case of Pre-EclampsiaDocument13 pagesNew Case of Pre-EclampsiaKristine AlejandroNo ratings yet
- ORESOL Is "Oral Glucose-ElectrolyteDocument4 pagesORESOL Is "Oral Glucose-ElectrolyteMichelle ViduyaNo ratings yet
- Teaching Plan Scabies 11Document4 pagesTeaching Plan Scabies 11umar khan0% (1)
- Dyci Sample Family-Case-AnalysisDocument75 pagesDyci Sample Family-Case-AnalysisNat Lynne Distor TrondilloNo ratings yet
- VIII. Discharge PlanDocument2 pagesVIII. Discharge PlanPia Therese CabaticNo ratings yet
- Care of Mother, Child, and Adolescents (Well Clients) NCM - 107 Nursing Care Plan Assessment Diagnosis Plan Intervention EvaluationDocument4 pagesCare of Mother, Child, and Adolescents (Well Clients) NCM - 107 Nursing Care Plan Assessment Diagnosis Plan Intervention EvaluationSophia Caisip100% (1)
- Nursing Care Plan Assessment Nursing Diagnosis Scientific Inference Planning Nursing Intervention Rationale Evaluation Long TermDocument10 pagesNursing Care Plan Assessment Nursing Diagnosis Scientific Inference Planning Nursing Intervention Rationale Evaluation Long TermSofia CartallaNo ratings yet
- Small For Gestational Age: (Case Presentation)Document17 pagesSmall For Gestational Age: (Case Presentation)BRYAN JOSEPH TIONGSONNo ratings yet
- Small For Gestational Age: (Case Presentation)Document18 pagesSmall For Gestational Age: (Case Presentation)BRYAN JOSEPH TIONGSONNo ratings yet
- Script Pedia 1Document38 pagesScript Pedia 1Jessy Arcaina BañagaNo ratings yet
- Small For Gestational Age: (Case Presentation)Document17 pagesSmall For Gestational Age: (Case Presentation)BRYAN JOSEPH TIONGSONNo ratings yet
- Lourdes Ward Manual On Policies and ProceduresDocument200 pagesLourdes Ward Manual On Policies and ProceduresBRYAN JOSEPH TIONGSONNo ratings yet
- Small For Gestational Age: (Case Presentation)Document18 pagesSmall For Gestational Age: (Case Presentation)BRYAN JOSEPH TIONGSONNo ratings yet
- 2019 Value Based Activity Proposal Format - Docx I 2021Document4 pages2019 Value Based Activity Proposal Format - Docx I 2021BRYAN JOSEPH TIONGSONNo ratings yet
- Medical - Surgical Nursing 3 & 4: Final ExaminationsDocument6 pagesMedical - Surgical Nursing 3 & 4: Final ExaminationsBRYAN JOSEPH TIONGSON100% (1)
- Causes of Death: How The Sexes Differ: Kathryn WilkinsDocument11 pagesCauses of Death: How The Sexes Differ: Kathryn WilkinsPRATIK GANGULYNo ratings yet
- Rhinomycosis: Rhinomycosis Disease Name Overview of Rhinomycosis DiseasesDocument3 pagesRhinomycosis: Rhinomycosis Disease Name Overview of Rhinomycosis Diseasesfais123No ratings yet
- Hyperthyroidism Article PubmedDocument12 pagesHyperthyroidism Article PubmedSandu AlexandraNo ratings yet
- Adult Development and Aging 7thDocument498 pagesAdult Development and Aging 7thFernandaGuimaraes83% (6)
- Veterinary Emergency Medicine SecretsDocument585 pagesVeterinary Emergency Medicine SecretsDea Marie Lopez100% (21)
- Friends Intro BookletDocument17 pagesFriends Intro Bookletxlitx02No ratings yet
- Indoor Air Quality in MalaysiaDocument63 pagesIndoor Air Quality in MalaysiakylerilNo ratings yet
- CASE PRESENTATION ON AnemiaDocument25 pagesCASE PRESENTATION ON AnemiaSafoora Rafeeq100% (2)
- BRS PediatricsDocument971 pagesBRS Pediatricstycobb6371% (7)
- Malignant Gliomas: Anaplastic Astrocytoma, Glioblastoma, Gliosarcoma, and Anaplastic OligodendrogliomaDocument11 pagesMalignant Gliomas: Anaplastic Astrocytoma, Glioblastoma, Gliosarcoma, and Anaplastic OligodendrogliomaSarahScandyNo ratings yet
- Cherie Cephas Nur 460 RN To BSN ReflectionDocument14 pagesCherie Cephas Nur 460 RN To BSN Reflectionapi-570349057No ratings yet
- Esophageal and Stomach Pathology-May+2019Document71 pagesEsophageal and Stomach Pathology-May+2019Karami Brutus0% (1)
- JNJNDocument1 pageJNJNGachibag IdNo ratings yet
- Hes 008 - Sas 13Document2 pagesHes 008 - Sas 13Juliannah ColinaresNo ratings yet
- Macroscopic UrinalysisDocument29 pagesMacroscopic UrinalysisJames De VeraNo ratings yet
- Patient ComplianceDocument2 pagesPatient ComplianceShadrackNo ratings yet
- Chapter 30 - Chronic Asthma - Dust in The Wind Level IIDocument5 pagesChapter 30 - Chronic Asthma - Dust in The Wind Level IIArriane AntonioNo ratings yet
- ACNS Training Module 2022-01-01 Part3 FINALDocument38 pagesACNS Training Module 2022-01-01 Part3 FINALAndres Rojas JerezNo ratings yet
- Blood Pressure Levels For Boys by Age and Height PercentileDocument4 pagesBlood Pressure Levels For Boys by Age and Height PercentileNuzla EmiraNo ratings yet
- Solve The OutbreakDocument1 pageSolve The OutbreakTUSHAR DASHNo ratings yet
- COVID 19 & Orthopedic Related Articles Till April 2021 Pgs 118Document119 pagesCOVID 19 & Orthopedic Related Articles Till April 2021 Pgs 118Mohan DesaiNo ratings yet
- Essential Health Assessment, Second Edition (p711-712)Document2 pagesEssential Health Assessment, Second Edition (p711-712)Aeshel TabuzoNo ratings yet
- Baharudin Et Al 2023 Factors Associated With Achievement of Blood Pressure Low Density Lipoprotein Cholesterol LDL CDocument13 pagesBaharudin Et Al 2023 Factors Associated With Achievement of Blood Pressure Low Density Lipoprotein Cholesterol LDL CFifi RetiatyNo ratings yet
- Chapter 1 ACSM Guidelines For Exercise Testing and Prescription 10 Edit Book (049-069)Document21 pagesChapter 1 ACSM Guidelines For Exercise Testing and Prescription 10 Edit Book (049-069)Sofi TarquinoNo ratings yet
- Cardiac Dysfunction in Neurocritical Care An Autonomic PerspectiveDocument14 pagesCardiac Dysfunction in Neurocritical Care An Autonomic PerspectiveMELVIN BURTONNo ratings yet
- Clinical Microscopy Ratio 2019 PDFDocument7 pagesClinical Microscopy Ratio 2019 PDFBinky SophiaNo ratings yet
- Post Natal CareDocument15 pagesPost Natal CareDaphneyNo ratings yet
- Nursing Care of A Family When A Child Has Gastrointestinal DisorderDocument3 pagesNursing Care of A Family When A Child Has Gastrointestinal DisorderIan BathanNo ratings yet
- Parotid 121206120631 Phpapp01Document26 pagesParotid 121206120631 Phpapp01shravani100% (1)
- Examination PositionsDocument2 pagesExamination PositionsMaddy Love YaelNo ratings yet