You might also like
- Sensory Enrichment Therapy For AutismDocument7 pagesSensory Enrichment Therapy For AutismCK_2023100% (2)
- Principles of ToxicologyDocument25 pagesPrinciples of ToxicologyHusam ShawaqfehNo ratings yet
- Wound CareDocument30 pagesWound Carerumaisha100% (2)
- Surgery One LinersDocument23 pagesSurgery One LinersKrishnaSagarNo ratings yet
- Phlebotomy Questions and Answers 2Document16 pagesPhlebotomy Questions and Answers 2emeki20029700100% (2)
- About AddicionsDocument186 pagesAbout AddicionsconservadorNo ratings yet
- Ferri's Clinical Advisor 2020 4Document3 pagesFerri's Clinical Advisor 2020 4Mourad BennaniNo ratings yet
- Surgery Mcqs PDFDocument43 pagesSurgery Mcqs PDFjcc50% (2)
- Review Notes - Fish & Freiberg Plastic SurgeryDocument24 pagesReview Notes - Fish & Freiberg Plastic SurgeryMartin Susanto, MDNo ratings yet
- Sedation in Critically IllDocument32 pagesSedation in Critically IllSamantha Deshapriya100% (1)
- General Pathology MCQsDocument32 pagesGeneral Pathology MCQsedcrfvtgb12345684% (37)
- Skin Integrity and Wound CareDocument47 pagesSkin Integrity and Wound CareCHALIE MEQUNo ratings yet
- Surgical Site Infection: Dr. Maryam. Surgical Unit 3Document22 pagesSurgical Site Infection: Dr. Maryam. Surgical Unit 3med stuNo ratings yet
- Wound ManagementDocument72 pagesWound Managementdrsonuchawla100% (1)
- Chronic Wounds PowerpointDocument34 pagesChronic Wounds PowerpointAnin DitaNo ratings yet
- Healing of Oral WoundsDocument73 pagesHealing of Oral WoundsMadhvendra Singh80% (5)
- Hassib Surgery, Volume IV - PDF @AUDatabotDocument49 pagesHassib Surgery, Volume IV - PDF @AUDatabotKhaled OmarNo ratings yet
- Secondary Union: Total of Lect: Wound Healing2 4 Stage College of Veterinary MedicineDocument4 pagesSecondary Union: Total of Lect: Wound Healing2 4 Stage College of Veterinary MedicineAshref BelhajNo ratings yet
- RJZ 269Document3 pagesRJZ 269Saffa AzharaaniNo ratings yet
- Medical Surgical Seminar 2Document87 pagesMedical Surgical Seminar 2charanjit kaurNo ratings yet
- Carbuncle Excision TechniqueDocument3 pagesCarbuncle Excision TechniquetseeckunNo ratings yet
- Wound Care and Laceration Repair For Nurse Practitioners in Emergency CareDocument2 pagesWound Care and Laceration Repair For Nurse Practitioners in Emergency CareJoriel Nicole Pedregosa PechonNo ratings yet
- 2012 A Case Report of Mucormycosis of Faciotemporal Region Mimicking As Bacterial Necrotizing FasciitisDocument5 pages2012 A Case Report of Mucormycosis of Faciotemporal Region Mimicking As Bacterial Necrotizing FasciitisWaqar JeelaniNo ratings yet
- BurnDocument1 pageBurnSPMC HRNo ratings yet
- General Surgery SEQDocument15 pagesGeneral Surgery SEQFatima Arshad100% (1)
- 1.types of Wounds & Wound HealingDocument21 pages1.types of Wounds & Wound Healingmhmdalbdyny764No ratings yet
- Skin UlcerDocument72 pagesSkin Ulcersahsweta67No ratings yet
- Wa0026.Document37 pagesWa0026.Ibrahim SultanNo ratings yet
- Metastatic Basal Cell Carcinoma of Buccal MucosaDocument8 pagesMetastatic Basal Cell Carcinoma of Buccal MucosaBlumeNo ratings yet
- Case Study 2Document7 pagesCase Study 2desdav100% (1)
- Necrotizing Fasciitis of The Breast: A Case Series and Review of The LiteratureDocument9 pagesNecrotizing Fasciitis of The Breast: A Case Series and Review of The LiteratureElli SymeonidouNo ratings yet
- (SURGERY SGD) Wound HealingDocument8 pages(SURGERY SGD) Wound HealingPaulene RiveraNo ratings yet
- Wound Healing: DR Ganesh SimkhadaDocument27 pagesWound Healing: DR Ganesh SimkhadaAnil BasnetNo ratings yet
- Group B 26.5.2023Document24 pagesGroup B 26.5.2023Yusuf ABBA MasaNo ratings yet
- GMS511Document29 pagesGMS511Mahmoud NafeaNo ratings yet
- GP Micro MCQ PDFDocument8 pagesGP Micro MCQ PDFAnna CortiNo ratings yet
- 2017 - Inflammation & Hamodinamic DisorderDocument93 pages2017 - Inflammation & Hamodinamic Disorder숭숩No ratings yet
- SMNR - 4... Wound HealingDocument62 pagesSMNR - 4... Wound HealingDrAmar GillNo ratings yet
- SDL 2 Wound and Wound HealingDocument4 pagesSDL 2 Wound and Wound HealingDn Ezrinah Dn EshamNo ratings yet
- Nursing Care in Plastic SurgeryDocument36 pagesNursing Care in Plastic Surgeryjengyee7186No ratings yet
- Acne Scars: Subcision: Methods and TechniquesDocument3 pagesAcne Scars: Subcision: Methods and TechniquesLuiz Henrique CararetoNo ratings yet
- CMTC Luz PulsadaDocument4 pagesCMTC Luz PulsadaIlse PalaciosNo ratings yet
- Dyshidrotic EczemaDocument2 pagesDyshidrotic EczemaHallison RanieriNo ratings yet
- Referat - CHRONIC WOUNDDocument19 pagesReferat - CHRONIC WOUNDAfifah Syifaul UmmahNo ratings yet
- Wound Healing & Wound Care: Souvik Adhikari Postdoctoral TraineeDocument55 pagesWound Healing & Wound Care: Souvik Adhikari Postdoctoral TraineeClaudio Luis VenturiniNo ratings yet
- Case ReportDocument5 pagesCase Reportyudhi kurniawanNo ratings yet
- Cystic Hy GromaDocument3 pagesCystic Hy GromaAhsan JamilNo ratings yet
- Decision Summary: Decision Memo For Electrostimulation For Wounds (CAG-00068N)Document28 pagesDecision Summary: Decision Memo For Electrostimulation For Wounds (CAG-00068N)omboNo ratings yet
- 2 - Healing & Repair2Document36 pages2 - Healing & Repair2aimi BatrisyiaNo ratings yet
- 2 Wound HealingDocument6 pages2 Wound HealingMohamad AlfarisNo ratings yet
- B. Caso Clinico. Turchin, I., & Barankin, B. 2006. Dermacase. Chronic Venous Insufficiency.Document3 pagesB. Caso Clinico. Turchin, I., & Barankin, B. 2006. Dermacase. Chronic Venous Insufficiency.Alex Andrés Cuevas UrriolaNo ratings yet
- Case Study - Hematology 1 PDFDocument21 pagesCase Study - Hematology 1 PDFMaria Lyn Ocariza ArandiaNo ratings yet
- Jordanian Board of Surgery Part 2 22Document3 pagesJordanian Board of Surgery Part 2 22izat husseinNo ratings yet
- Komplikasi FrakturDocument3 pagesKomplikasi FrakturDwi Tantri SPNo ratings yet
- Wound Healing1Document8 pagesWound Healing1muralidhar_mettaNo ratings yet
- Pathology Full Book Test (Powered by Medicose Prep Academy Prepared by Maria Shoaib, SZMC)Document12 pagesPathology Full Book Test (Powered by Medicose Prep Academy Prepared by Maria Shoaib, SZMC)farhannawaz015No ratings yet
- Hyperbaric Oxygen Therapy in The Treatment of DiabeticDocument28 pagesHyperbaric Oxygen Therapy in The Treatment of Diabeticnadya shabirah zahraNo ratings yet
- PDIA Art 17695-10Document6 pagesPDIA Art 17695-10faniaNo ratings yet
- Sub Epidermal Blister Formation. Immunofluorescence Reveals Iga Present Within Dermal PapillaeDocument6 pagesSub Epidermal Blister Formation. Immunofluorescence Reveals Iga Present Within Dermal PapillaeRabia RabiaNo ratings yet
- Chap-1a Wound HealingDocument60 pagesChap-1a Wound HealingAlex HaileyesusNo ratings yet
- Wound:: "A Type of Physical Trauma Whereby The Integrity of The Skin or of Any Tissue Is Compromised."Document15 pagesWound:: "A Type of Physical Trauma Whereby The Integrity of The Skin or of Any Tissue Is Compromised."IqraNo ratings yet
- Mri Scan Sir Ganga Ram Hospital DelhiDocument7 pagesMri Scan Sir Ganga Ram Hospital DelhiAmit SinghNo ratings yet
- Basic ECG InterpretationDocument62 pagesBasic ECG Interpretationmohannadalkwiese3No ratings yet
- MTLB New Highlighted Notes 2Document37 pagesMTLB New Highlighted Notes 2Kathleen Mae NatividadNo ratings yet
- Birth Asphycia and Cerebral Palsy Clinics Perinatology 2005Document16 pagesBirth Asphycia and Cerebral Palsy Clinics Perinatology 2005Sebastián Silva SotoNo ratings yet
- Guias Hipertension 2023 Esc BDocument14 pagesGuias Hipertension 2023 Esc Bmiguel contrerasNo ratings yet
- AnisocoriaDocument19 pagesAnisocoriadanitadwiNo ratings yet
- Efficacy of Dialectical Behavior Therapy For Adolescents at High Risk For Suicide: A Randomized Clinical TrialDocument11 pagesEfficacy of Dialectical Behavior Therapy For Adolescents at High Risk For Suicide: A Randomized Clinical TrialLia Marcela Rivera HernandezNo ratings yet
- Source E Learning NCM 121Document11 pagesSource E Learning NCM 121Nathaniel PulidoNo ratings yet
- Phenylephrine: 1568 Cough Suppressants Expectorants Mucolytics and Nasal DecongestantsDocument2 pagesPhenylephrine: 1568 Cough Suppressants Expectorants Mucolytics and Nasal DecongestantsRanny LaidasuriNo ratings yet
- BoilDocument4 pagesBoilPipipopoNo ratings yet
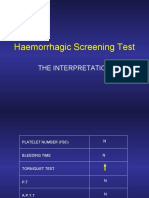
- Haemorrhagic Screening Test: The InterpretationDocument40 pagesHaemorrhagic Screening Test: The InterpretationAngel 冯晓君No ratings yet
- Emergency Oxygen Therapy in The Dental Practice: Administration and ManagementDocument4 pagesEmergency Oxygen Therapy in The Dental Practice: Administration and ManagementAndi Suchy Qumala SarieNo ratings yet
- Primolut N NorethisteroneDocument2 pagesPrimolut N NorethisteroneSarathyTDNo ratings yet
- Medical Monitor PDFDocument5 pagesMedical Monitor PDFFábio Vitor MartinsNo ratings yet
- A.O. No. 67 S 1989: "Revised Rules and Regulations On Registration of Pharmaceutical Products"Document24 pagesA.O. No. 67 S 1989: "Revised Rules and Regulations On Registration of Pharmaceutical Products"khara teanoNo ratings yet
- Deficient Knowledge CanalesDocument4 pagesDeficient Knowledge CanalesIzhra MargateNo ratings yet
- Psicosis - 2021Document30 pagesPsicosis - 2021Felipe VergaraNo ratings yet
- CV-Alfred - AgaDocument6 pagesCV-Alfred - AgaAgostin CukajNo ratings yet
- IvpDocument18 pagesIvpFranz SalazarNo ratings yet
- Signs RadiopediaDocument142 pagesSigns RadiopediaasadroxNo ratings yet
- Reforms Booklet HWC English Updated 14th Sep 2021Document42 pagesReforms Booklet HWC English Updated 14th Sep 2021Akanksha SinghNo ratings yet
- Management of Ocular Chemical InjuriesDocument82 pagesManagement of Ocular Chemical InjuriesAfiqah FaizalNo ratings yet
- Leo PlusDocument2 pagesLeo PluskbrinaldiNo ratings yet
- 02 Chain of SurvivalDocument1 page02 Chain of SurvivalHatem FaroukNo ratings yet
- Amets ZurutuzaDocument3 pagesAmets ZurutuzaMaitane ArrietaNo ratings yet