You might also like
- Atlas of Oral Histology by Akramjuaim PDFDocument151 pagesAtlas of Oral Histology by Akramjuaim PDFAna Maria Hernandez Ardila100% (1)
- Caries PPT - ppt11Document109 pagesCaries PPT - ppt11dr parveen bathlaNo ratings yet
- NATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideFrom EverandNATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideRating: 1 out of 5 stars1/5 (1)
- BARACARBDocument2 pagesBARACARBYudha Satria50% (2)
- DentinDocument133 pagesDentinMohammed hisham khan100% (3)
- DentinDocument88 pagesDentinSuhana Ahmed100% (1)
- Oral Histology Questions Part 2Document9 pagesOral Histology Questions Part 2hamzkk100% (3)
- Enamel Structure and FormationDocument106 pagesEnamel Structure and FormationManva MonishNo ratings yet
- Oral Histology BCQ ListDocument79 pagesOral Histology BCQ Listwaqas khanNo ratings yet
- Oral HistologyDocument6 pagesOral HistologyMr. Orange100% (2)
- Developmental Anomalies of Oral Soft TissuesDocument73 pagesDevelopmental Anomalies of Oral Soft Tissuesvellingiriramesh53040% (1)
- Oral Histology Quiz - Enumerate (AmCoFam)Document34 pagesOral Histology Quiz - Enumerate (AmCoFam)AmericanCornerFamily100% (2)
- Tooth Eruption QuestionsDocument8 pagesTooth Eruption QuestionsAli Al-Qudsi100% (2)
- Retention and Stability of Complete DentureDocument7 pagesRetention and Stability of Complete Denturemanishpankaj123No ratings yet
- Oral Mucous MembraneDocument200 pagesOral Mucous MembraneKush Pathak100% (3)
- Enamel NotesDocument7 pagesEnamel NotesShahid Hameed100% (2)
- Enamel Developmental Stages of A ToothDocument12 pagesEnamel Developmental Stages of A ToothClarisse Mendoza100% (2)
- Tarnish - CorrosionDocument18 pagesTarnish - CorrosionAmniAzmiNo ratings yet
- Seminar Presentation On Enamel: By-Devanshi Sharma P.G.1 Year Dept. of Cons. Dentistry & EndoDocument105 pagesSeminar Presentation On Enamel: By-Devanshi Sharma P.G.1 Year Dept. of Cons. Dentistry & EndoDevanshi SharmaNo ratings yet
- 1 EnamelDocument40 pages1 EnamelHarshvardhanNo ratings yet
- Role of Saliva in Dental CariesDocument29 pagesRole of Saliva in Dental Carieskhush sidhu100% (1)
- Oral Histology NotesDocument18 pagesOral Histology NotesKhalil Raziq100% (1)
- Development of Teeth 1Document37 pagesDevelopment of Teeth 1Muli MaroshiNo ratings yet
- Oral Histology Quiz - Short (AmCoFam)Document10 pagesOral Histology Quiz - Short (AmCoFam)AmericanCornerFamily100% (4)
- Tooth Eruption and Shedding ExplainedDocument29 pagesTooth Eruption and Shedding Explainedjenny girl100% (1)
- Oral Histology Questions Part 1Document8 pagesOral Histology Questions Part 1hamzkk100% (3)
- Oral Histology Quick ReviewDocument67 pagesOral Histology Quick ReviewTimothy Jairus LawNo ratings yet
- Dental Anatomy Final ReviewDocument10 pagesDental Anatomy Final ReviewSalma AhmedNo ratings yet
- Periodontal LigamentDocument56 pagesPeriodontal LigamentDent DealsNo ratings yet
- CEMENTUMDocument50 pagesCEMENTUMDENTALORG.COM100% (1)
- Zinc Polycarboxylate Cement: Properties and UsesDocument41 pagesZinc Polycarboxylate Cement: Properties and UsesASHWINI ATHULNo ratings yet
- Furcation 31 12 14Document25 pagesFurcation 31 12 14Ahmed BadrNo ratings yet
- Dental Enamel: Dr. Prabhat Saxena Dept of Endodontics S.G.T. Dental College, GurgaonDocument114 pagesDental Enamel: Dr. Prabhat Saxena Dept of Endodontics S.G.T. Dental College, GurgaonPrabhat Saxena100% (1)
- Idoc - Pub - Dental Anatomy Questions PDFDocument16 pagesIdoc - Pub - Dental Anatomy Questions PDFhieulee84No ratings yet
- Oral Histology Lecture 7Document5 pagesOral Histology Lecture 7Mohamed Harun B. SanohNo ratings yet
- 7 - Dentinogenesis PDFDocument14 pages7 - Dentinogenesis PDFHãnëën Twalbeh83% (12)
- AIIMS Dental PG November 2008 Question PaperDocument6 pagesAIIMS Dental PG November 2008 Question PaperRudra VermaNo ratings yet
- Glass Ionomer Cement PolyalkenoatesDocument26 pagesGlass Ionomer Cement PolyalkenoatesArifa parveenNo ratings yet
- MCQDocument1 pageMCQmarapottanNo ratings yet
- Dentogingival Junction AnatomyDocument7 pagesDentogingival Junction AnatomyDrKrishna Das100% (1)
- Principles of Cavity PreparationDocument18 pagesPrinciples of Cavity PreparationAnh Do Thi VanNo ratings yet
- Ortho SEQDocument15 pagesOrtho SEQMalik UmerNo ratings yet
- Oral Histology Quiz - Scientific Term (AmCoFam)Document22 pagesOral Histology Quiz - Scientific Term (AmCoFam)AmericanCornerFamily100% (5)
- Growth & Dev - of MaxillaDocument26 pagesGrowth & Dev - of Maxillaharshita parasharNo ratings yet
- BDS 3rd Year Oral Pathology NotesDocument35 pagesBDS 3rd Year Oral Pathology NotesDaniyal BasitNo ratings yet
- Dentin and Its Clinical ConsiderationDocument97 pagesDentin and Its Clinical ConsiderationKrithikaNo ratings yet
- Maxillary Permanent Central IncisorsDocument68 pagesMaxillary Permanent Central IncisorsAmit Singh100% (1)
- Oral Pathology Test Questions and AnswersDocument3 pagesOral Pathology Test Questions and Answersardesh abdille0% (1)
- Pulp Dentin ComplexDocument187 pagesPulp Dentin ComplexHitesh Chopra100% (1)
- Access Cavity Preparation FinalDocument63 pagesAccess Cavity Preparation Finalrasagna reddyNo ratings yet
- Periodontal LigamentDocument65 pagesPeriodontal LigamentReshmaa Rajendran100% (1)
- Space MaintainerDocument36 pagesSpace MaintainerDenis KimNo ratings yet
- Dental Pulp: A Unique Tissue's Unique Anatomy and CellsDocument83 pagesDental Pulp: A Unique Tissue's Unique Anatomy and CellsAnas Kallayil100% (2)
- GicDocument75 pagesGicNihar Arya100% (1)
- Oral Histo Midterm Review PDFDocument17 pagesOral Histo Midterm Review PDFHãnëën TwalbehNo ratings yet
- EnamelDocument89 pagesEnamelPavanNo ratings yet
- The Periodontium Tissues Supporting TeethDocument78 pagesThe Periodontium Tissues Supporting TeethShuba Prasad100% (1)
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideFrom EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNo ratings yet
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 16160/maq Chennai Exp Second Sitting (2S)Document2 pages16160/maq Chennai Exp Second Sitting (2S)siyaNo ratings yet
- Madhudentinppt 170809045059Document74 pagesMadhudentinppt 170809045059siyaNo ratings yet
- Pedi HN SlidesDocument71 pagesPedi HN SlidesvelangniNo ratings yet
- Osteosarcoma: A Guide to Clinical Features, Risk Factors, Variants & TreatmentDocument28 pagesOsteosarcoma: A Guide to Clinical Features, Risk Factors, Variants & TreatmentsiyaNo ratings yet
- Immunology of Dental Caries WordDocument12 pagesImmunology of Dental Caries WordsiyaNo ratings yet
- Development of TeethDocument30 pagesDevelopment of TeethsiyaNo ratings yet
- Development and Growth of Teeth: Dr. Madhusudhan ReddyDocument48 pagesDevelopment and Growth of Teeth: Dr. Madhusudhan ReddysiyaNo ratings yet
- Development and Growth of Teeth: Dr. Madhusudhan ReddyDocument48 pagesDevelopment and Growth of Teeth: Dr. Madhusudhan ReddysiyaNo ratings yet
- Development of TeethDocument30 pagesDevelopment of TeethsiyaNo ratings yet
- BIODENTINEDocument1 pageBIODENTINEsiyaNo ratings yet
- Development and Growth of Teeth: Dr. Madhusudhan ReddyDocument48 pagesDevelopment and Growth of Teeth: Dr. Madhusudhan ReddysiyaNo ratings yet
- Enamel DR RiazDocument76 pagesEnamel DR RiazDevaraj ManicamNo ratings yet
- BIODENTINEDocument1 pageBIODENTINEsiyaNo ratings yet
- BIODENTINEDocument1 pageBIODENTINEsiyaNo ratings yet
- Vitamin and Mineral Contents of Gongronema Latifolium LeavesDocument3 pagesVitamin and Mineral Contents of Gongronema Latifolium LeavesFrida Febriani IsnanisafitriNo ratings yet
- DM3xxx Accessory List LeafletDocument2 pagesDM3xxx Accessory List LeafletAdvantec SrlNo ratings yet
- Bronchiolitis A Practical Approach For The General RadiologistDocument42 pagesBronchiolitis A Practical Approach For The General RadiologistTara NareswariNo ratings yet
- HymssheetDocument4 pagesHymssheettoby_wardmanNo ratings yet
- Israel Is The MessIahDocument288 pagesIsrael Is The MessIahTeerayoot NoidaNo ratings yet
- RTWP OptimisationHanFeedbackDocument31 pagesRTWP OptimisationHanFeedbackSeth Mawuli Dedzoe100% (1)
- Maersk QuestionnaireDocument43 pagesMaersk QuestionnaireSahil SharmaNo ratings yet
- A Drop of Blood: Casting Time Range Components Duration Casting Time Range Components DurationDocument6 pagesA Drop of Blood: Casting Time Range Components Duration Casting Time Range Components DurationCristobal RencoretNo ratings yet
- Mec 323Document68 pagesMec 323VINAY B.SNo ratings yet
- 978 613 8 91055 8 PDFDocument309 pages978 613 8 91055 8 PDFEr Sayan ParamanikNo ratings yet
- Fundamentals of Wind EnergyDocument24 pagesFundamentals of Wind EnergyMas3odNo ratings yet
- GREEN AIR CONDITIONER Mechanical Presentation TopicsDocument9 pagesGREEN AIR CONDITIONER Mechanical Presentation TopicsCerin91No ratings yet
- 3 Soal Ganjil Inggris MaritimDocument8 pages3 Soal Ganjil Inggris MaritimFikri Mu'izNo ratings yet
- PDM TempDocument2 pagesPDM Tempamit rajputNo ratings yet
- EVS Complete Notes PDFDocument148 pagesEVS Complete Notes PDFrevantrajkpdh2002No ratings yet
- Singaporean Notices To Mariners: Section ContentDocument35 pagesSingaporean Notices To Mariners: Section ContentGaurav SoodNo ratings yet
- 3 Sample Warranty: Sun Control Window FilmDocument1 page3 Sample Warranty: Sun Control Window FilmJanan AhmadNo ratings yet
- Fetal and Placental Development - FETAL Sac, Umbilical Cord .Abnormalities of PlacentaDocument150 pagesFetal and Placental Development - FETAL Sac, Umbilical Cord .Abnormalities of PlacentaKripa SusanNo ratings yet
- The Practical Welding EngineerDocument154 pagesThe Practical Welding EngineerMohamed Atef0% (1)
- Engineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignDocument28 pagesEngineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignMehdi NouriNo ratings yet
- Fiber Crops - FlaxDocument33 pagesFiber Crops - Flaxmalath bashNo ratings yet
- Mathematical Structures of The UniverseDocument228 pagesMathematical Structures of The UniverseMaki MajomNo ratings yet
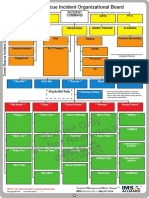
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Minitek Indore Profile 2Document9 pagesMinitek Indore Profile 2kunal agiwaleNo ratings yet
- 88 Dean StreetDocument36 pages88 Dean StreetPatrick BatyNo ratings yet
- Theoretical Development of The Brooks-Corey CapillDocument7 pagesTheoretical Development of The Brooks-Corey CapillDiana Vanessa PedrazaNo ratings yet
- Foundation of EducationDocument31 pagesFoundation of EducationM T Ząřřąř100% (1)
- MUSCULAR SYSTEM WORKSHEET Slides 1 To 4Document4 pagesMUSCULAR SYSTEM WORKSHEET Slides 1 To 4kwaiyuen ohnNo ratings yet
- C32 MOTOR CAT Electronic Unit Injector - TestDocument2 pagesC32 MOTOR CAT Electronic Unit Injector - TestFreddy Villegas100% (1)