You might also like
- Treatment Planning AdhdDocument12 pagesTreatment Planning AdhdLuja2009No ratings yet
- Ball & Bindler Pediatric Nursing - Caring For ChildrenDocument105 pagesBall & Bindler Pediatric Nursing - Caring For Childrenfriendofnurse50% (4)
- Excerpted From "Margaret Sanger: A Life of Passion" by Jean H. BakerDocument26 pagesExcerpted From "Margaret Sanger: A Life of Passion" by Jean H. Bakerwamu885No ratings yet
- Unit 1. Clinical PharmacyDocument5 pagesUnit 1. Clinical PharmacyAashish BhattaraiNo ratings yet
- BQC4ED PreviewDocument51 pagesBQC4ED PreviewJuan Marcos Martinez ZevallosNo ratings yet
- Vol 19.1 - Sleep Disorders.2013Document252 pagesVol 19.1 - Sleep Disorders.2013Martoiu MariaNo ratings yet
- Yasmeen Sitxfa002Document35 pagesYasmeen Sitxfa002ranu jain100% (1)
- Pharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Test Bank 1Document17 pagesPharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Test Bank 1coreyfuentesxfkbzmqpty100% (26)
- Quality of Service of The School Canteen: Part I. Socio-Demographic Profile QuestionnaireDocument2 pagesQuality of Service of The School Canteen: Part I. Socio-Demographic Profile QuestionnaireKB Salandores50% (2)
- Classification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMDocument2 pagesClassification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMCarlos GonzalezNo ratings yet
- Care of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryDocument13 pagesCare of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryRazel Kinette AzotesNo ratings yet
- Journal of The American Pharmacists Association: ResearchDocument11 pagesJournal of The American Pharmacists Association: Researchnoventina7marbunNo ratings yet
- Prescribing Habits and CaregivDocument10 pagesPrescribing Habits and CaregivHerawati YustikasariNo ratings yet
- Institute For Safe Medication PracticesDocument6 pagesInstitute For Safe Medication Practicesadza30No ratings yet
- When Parents Won't Vaccinate Their Children: A Qualitative Investigation of Australian Primary Care Providers' ExperiencesDocument20 pagesWhen Parents Won't Vaccinate Their Children: A Qualitative Investigation of Australian Primary Care Providers' ExperiencesTimmy LarasatiNo ratings yet
- 7 Sadiqua EtalDocument6 pages7 Sadiqua EtaleditorijmrhsNo ratings yet
- Research Papers On Clinical PharmacyDocument6 pagesResearch Papers On Clinical Pharmacyaflbrtdar100% (1)
- Validating The Children's Medicines Use Questionnaire (CMUQ) in AustraliaDocument9 pagesValidating The Children's Medicines Use Questionnaire (CMUQ) in AustraliadidiNo ratings yet
- Strengthening Pharmacy Practice in Vietnam: Findings of A Training Intervention StudyDocument9 pagesStrengthening Pharmacy Practice in Vietnam: Findings of A Training Intervention StudySarahNo ratings yet
- Research Paper Medication ErrorsDocument6 pagesResearch Paper Medication Errorsegxtc6y3100% (1)
- Factors Influencing Paediatric Nurses' Responses To Medication AdministrationDocument4 pagesFactors Influencing Paediatric Nurses' Responses To Medication AdministrationYuni AstutiNo ratings yet
- Objetivo: Determinar El Nivel de Conocimiento Sobre La Prescripción FarmacológicaDocument17 pagesObjetivo: Determinar El Nivel de Conocimiento Sobre La Prescripción FarmacológicaYefferson Hilario LlantoyNo ratings yet
- AMR ResistanceDocument1 pageAMR ResistanceTugume FrancisNo ratings yet
- 2015 Article 516Document12 pages2015 Article 516Mukhtar TarNo ratings yet
- Tren Kesalahan Pengobatan Dan Efek Dari Faktor Yang Berhubungan Dengan Orang, Terkait Lingkungan Dan Komunikasi Pada Kesalahan Pengobatan Di Rumah Sakit AnakDocument7 pagesTren Kesalahan Pengobatan Dan Efek Dari Faktor Yang Berhubungan Dengan Orang, Terkait Lingkungan Dan Komunikasi Pada Kesalahan Pengobatan Di Rumah Sakit AnakEnggar Ardiani TagapNo ratings yet
- Assessment 2 Medication ErrorsDocument9 pagesAssessment 2 Medication Errorsakko aliNo ratings yet
- NCM 103 - Journal Reading Picot - ViosDocument3 pagesNCM 103 - Journal Reading Picot - ViosIra Velle ViosNo ratings yet
- Children and Their Medicines FP Facilitators GuideDocument2 pagesChildren and Their Medicines FP Facilitators Guidedaniela bosoagaNo ratings yet
- Appropriateness of Acetaminophen Dosing by Caregivers of Pediatric Patients Presenting To The Emergency Department at The University Pediatric Hospital in Puerto RicoDocument7 pagesAppropriateness of Acetaminophen Dosing by Caregivers of Pediatric Patients Presenting To The Emergency Department at The University Pediatric Hospital in Puerto RicolizbethNo ratings yet
- Children 01 00424Document17 pagesChildren 01 00424netoginetaNo ratings yet
- Children: Complementary Parent Components For Pediatric Pain Families: Innovations in TreatmentDocument12 pagesChildren: Complementary Parent Components For Pediatric Pain Families: Innovations in Treatmentپردیس سلیمانی اصلNo ratings yet
- Unlicensed and Off Label Uses of Drugs in Paediatrics A Review - Cuzzolin, 2003Document7 pagesUnlicensed and Off Label Uses of Drugs in Paediatrics A Review - Cuzzolin, 2003Mara KalitaNo ratings yet
- Kesehatan Anak 111219b DR Isnatin Merec Bulletin Vol11 No2Document4 pagesKesehatan Anak 111219b DR Isnatin Merec Bulletin Vol11 No2Gianina Yogy100% (1)
- Non-pharmacological behaviour management - 副本Document37 pagesNon-pharmacological behaviour management - 副本刘雨樵No ratings yet
- 2019 Article 305 PDFDocument3 pages2019 Article 305 PDFDipyanalarNo ratings yet
- Case Report: Communication Strategies For Empowering and Protecting ChildrenDocument9 pagesCase Report: Communication Strategies For Empowering and Protecting ChildrennabilahNo ratings yet
- Sudanese Parents' Knowledge, Attitudes and Practice About Self Medication To Their Children: Qualitative StudyDocument5 pagesSudanese Parents' Knowledge, Attitudes and Practice About Self Medication To Their Children: Qualitative StudyMusthafa Afif WardhanaNo ratings yet
- Saudi Pharmaceutical JournalDocument5 pagesSaudi Pharmaceutical JournalVictor TabuncicNo ratings yet
- 17-Evaluation of The Safety of Drugs WorkshopDocument9 pages17-Evaluation of The Safety of Drugs WorkshopsasNo ratings yet
- Attitude On Clinical Pharmacy Training: The Case of Haramaya University, EthiopiaDocument8 pagesAttitude On Clinical Pharmacy Training: The Case of Haramaya University, EthiopiaAychluhm TatekNo ratings yet
- Filipino JournalsDocument9 pagesFilipino JournalsMark Louis ChicaNo ratings yet
- Ni Hms 71150Document22 pagesNi Hms 71150Kiana TehraniNo ratings yet
- Literature Review On Medication Administration ErrorsDocument7 pagesLiterature Review On Medication Administration Errorsea2167raNo ratings yet
- Artikel 3 Berland 2017Document8 pagesArtikel 3 Berland 2017Eline DebaereNo ratings yet
- MederrorpaperDocument6 pagesMederrorpaperapi-642984838No ratings yet
- Pemberian Obat Pada AnakDocument19 pagesPemberian Obat Pada AnakMuhamad RockystankiNo ratings yet
- Pharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Test Bank 1Document34 pagesPharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Test Bank 1matthew100% (51)
- Research Paper On PolypharmacyDocument5 pagesResearch Paper On Polypharmacyefj02jba100% (1)
- Prevalence of Parental Misconceptions About Antibiotic UseDocument13 pagesPrevalence of Parental Misconceptions About Antibiotic UseCGFernandez2014No ratings yet
- Maternal Breast Milk Feeding and Length of Treatment in Infants With Neonatal Abstinence SyndromeDocument7 pagesMaternal Breast Milk Feeding and Length of Treatment in Infants With Neonatal Abstinence SyndromeHariCexinkwaeNo ratings yet
- Consent in Child Leukemia Parent Participation and Physician-Parent Communication During InformedDocument10 pagesConsent in Child Leukemia Parent Participation and Physician-Parent Communication During InformedPutu BudiastawaNo ratings yet
- Factors Associated With Parental Self-Medication of Antibiotics in Health Centers of ManilaDocument20 pagesFactors Associated With Parental Self-Medication of Antibiotics in Health Centers of Manilamatcha18No ratings yet
- Clinical Pharmacy Services in A Pediatric ERDocument4 pagesClinical Pharmacy Services in A Pediatric ERMuhammad Ibraheem AhmadNo ratings yet
- Saya Sedang Berbagi 'Off Label Drug-Dikonversi' Dengan AndaDocument10 pagesSaya Sedang Berbagi 'Off Label Drug-Dikonversi' Dengan AndacahyaNo ratings yet
- Client Safety and Risk Management AssignmentDocument6 pagesClient Safety and Risk Management Assignmentmelanie.acostaa56No ratings yet
- Tanaman HerbalDocument134 pagesTanaman Herbalwhy_smart03No ratings yet
- International Journal of Research in Pharmacology & PharmacotherapeuticsDocument7 pagesInternational Journal of Research in Pharmacology & PharmacotherapeuticskrishnasreeNo ratings yet
- Child Health Nursing Partnering With Children and Families 3rd Edition Ball Test BankDocument15 pagesChild Health Nursing Partnering With Children and Families 3rd Edition Ball Test Bankkevinfryecqiozexkjy100% (25)
- Uva-Dare (Digital Academic Repository) : Maaskant, JolandaDocument21 pagesUva-Dare (Digital Academic Repository) : Maaskant, JolandaYogi SaputraNo ratings yet
- Healthy Horizons-Butler University Ambulatory Care Appe Rotation SyllabusDocument13 pagesHealthy Horizons-Butler University Ambulatory Care Appe Rotation Syllabusapi-316593964No ratings yet
- Exploring The Knowledge and Attitude of Medical and Pharmacy Students About Generic Medicine in Lahore, PakistanDocument7 pagesExploring The Knowledge and Attitude of Medical and Pharmacy Students About Generic Medicine in Lahore, PakistanMathilda UllyNo ratings yet
- 2019 Article 4622Document10 pages2019 Article 4622shizuka samaNo ratings yet
- Effect of The Planned Therapeutic CommunicationDocument12 pagesEffect of The Planned Therapeutic CommunicationsherlyNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationFrom EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNo ratings yet
- Coronavirus Disease 2019 (COVID-19) Treatment Versus Mycobacterial Infections: Better Safe Than Sorry?Document2 pagesCoronavirus Disease 2019 (COVID-19) Treatment Versus Mycobacterial Infections: Better Safe Than Sorry?Nindie AulhieyaNo ratings yet
- Dhillon - Ear, Nose and Throat Head and Neck Surgery at 2000 Churcill LivingstoneDocument124 pagesDhillon - Ear, Nose and Throat Head and Neck Surgery at 2000 Churcill LivingstoneNindie AulhieyaNo ratings yet
- Case Report COVID-19 and Pulmonary Mycobacterium Tuberculosis CoinfectionDocument4 pagesCase Report COVID-19 and Pulmonary Mycobacterium Tuberculosis CoinfectionNindie AulhieyaNo ratings yet
- Pmed 1003208Document23 pagesPmed 1003208Nindie AulhieyaNo ratings yet
- Bmjopen 2019 034828Document9 pagesBmjopen 2019 034828Nindie AulhieyaNo ratings yet
- 2020 Article 5771Document11 pages2020 Article 5771Nindie AulhieyaNo ratings yet
- Accepted Manuscript: Victoria Otuka, Charles Ronga, Philip K. Chebii, Priscillah W. Maina, Zainab JembeDocument27 pagesAccepted Manuscript: Victoria Otuka, Charles Ronga, Philip K. Chebii, Priscillah W. Maina, Zainab JembeNindie AulhieyaNo ratings yet
- Perbandingan Kasus Fatal Akibat Covid-19 Pada Beberapa Negara Asia TenggaraDocument6 pagesPerbandingan Kasus Fatal Akibat Covid-19 Pada Beberapa Negara Asia Tenggarasofia uyNo ratings yet
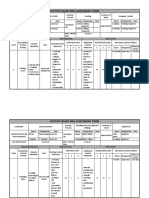
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- Depression Anxiety TreatmentDocument2 pagesDepression Anxiety TreatmentAlex PavNo ratings yet
- Purpose of Travel - SampleDocument3 pagesPurpose of Travel - SampleVirat GadhviNo ratings yet
- 1123 s12 in 22Document4 pages1123 s12 in 22mstudy123456No ratings yet
- Adaptacininstrumentos WASTDocument11 pagesAdaptacininstrumentos WASTAsley Cabrera LopezNo ratings yet
- Monouso Ge Healthcare, Catalogo Prodotti GE HealthcareDocument263 pagesMonouso Ge Healthcare, Catalogo Prodotti GE HealthcareAlessandro ArmaroliNo ratings yet
- History of Perioperative Nursing 2023Document10 pagesHistory of Perioperative Nursing 2023Boniface MogakaNo ratings yet
- Digi T Vigilance TestDocument6 pagesDigi T Vigilance TestJillianne FrancoNo ratings yet
- Common Gynaecological Conditions Leading To Referral - 071118Document20 pagesCommon Gynaecological Conditions Leading To Referral - 071118zehra khowajaNo ratings yet
- Table of Specification For Second Periodical Test in Mapeh IvDocument4 pagesTable of Specification For Second Periodical Test in Mapeh IvJENNIFER SERVONo ratings yet
- What Is MastectomyDocument2 pagesWhat Is MastectomyMyami Bersamen100% (1)
- Blood Transfusion PDFDocument20 pagesBlood Transfusion PDFalaamorsyNo ratings yet
- Tennessee Hazard Mitigation Plan 2018 FINALDocument388 pagesTennessee Hazard Mitigation Plan 2018 FINALAnonymous GF8PPILW5100% (1)
- CID Cheese Mozzarella LiteDocument8 pagesCID Cheese Mozzarella LiteBayu SyurahmadNo ratings yet
- MVA ToolkitDocument89 pagesMVA ToolkitVishal RasalNo ratings yet
- Water Intoxication - Is It Possible To Drink Too Much Water???Document11 pagesWater Intoxication - Is It Possible To Drink Too Much Water???NoraNo ratings yet
- Neonatal MeningitisDocument24 pagesNeonatal MeningitisHelena Trinina Saragih100% (1)
- Home Slim Thick Fitmas Week 6 PDFDocument84 pagesHome Slim Thick Fitmas Week 6 PDFjennaNo ratings yet
- Copd VS AsthmaDocument2 pagesCopd VS AsthmaHarkirat AtwalNo ratings yet
- ICTAPP 23 36 FinalVersionDocument7 pagesICTAPP 23 36 FinalVersionzobiNo ratings yet
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- Ijcpd-15-S103 MetanalysisDocument11 pagesIjcpd-15-S103 MetanalysisGabriela ZuritaNo ratings yet
- P RM 01 Incident Reporting PolicyDocument44 pagesP RM 01 Incident Reporting PolicypatientsafetyNo ratings yet
- Covid-19 Test Report: Patient Name: Akash GargDocument1 pageCovid-19 Test Report: Patient Name: Akash GargGenestrings Diagnostic CenterNo ratings yet