You might also like
- Effect of Refractive Error On VEP in Myopic Boys and GirlsDocument3 pagesEffect of Refractive Error On VEP in Myopic Boys and GirlsNational Journal of Medical Research &Yoga ScienceNo ratings yet
- PDF JTN 164Document4 pagesPDF JTN 164Gede SuputraNo ratings yet
- VEP Normative Values and GenderDocument4 pagesVEP Normative Values and GenderJelly BXNo ratings yet
- POAG and Cataract Risk Study Finds No Significant LinkDocument4 pagesPOAG and Cataract Risk Study Finds No Significant LinkFernando CortesNo ratings yet
- Visual Outcomes of Amblyopia Therapy: Ophthalmology Original ArticleDocument6 pagesVisual Outcomes of Amblyopia Therapy: Ophthalmology Original ArticlethomasNo ratings yet
- Early color vision impairment in young patients with demyelinating diseaseDocument12 pagesEarly color vision impairment in young patients with demyelinating diseaseAnjali MohanNo ratings yet
- Jurnal Anti VEFGDocument9 pagesJurnal Anti VEFGFitria Sirr Mu'thiarohmahNo ratings yet
- Developmental Binocular Vision AbnormalitiesDocument10 pagesDevelopmental Binocular Vision AbnormalitiesGian Carlo Giusto BurboaNo ratings yet
- Studio PilotDocument8 pagesStudio PilotAnonymous fyN6ueONo ratings yet
- 1 s2.0 S2211034816302279 Main - EvokedpotentialDocument5 pages1 s2.0 S2211034816302279 Main - EvokedpotentialyeraygranadoNo ratings yet
- Evaluation of The Relationship Between Binocular Anomaly and Headache Prospective Cross Sectional StudyDocument7 pagesEvaluation of The Relationship Between Binocular Anomaly and Headache Prospective Cross Sectional StudyEstefania GuerreroNo ratings yet
- Effect of Ocular Dominance On The Latency and Amplitude of Visual Evoked PotentialsDocument6 pagesEffect of Ocular Dominance On The Latency and Amplitude of Visual Evoked PotentialsMaria FernandaNo ratings yet
- Pi Is 0161642022006698Document7 pagesPi Is 0161642022006698TRẦN NGỌC LAM THANHNo ratings yet
- Article Assessment of Opicinumab in Acute Neuritis Using Multifocal Visual Evoked PotentialDocument13 pagesArticle Assessment of Opicinumab in Acute Neuritis Using Multifocal Visual Evoked PotentialMahesa Kurnianti PutriNo ratings yet
- Pattern of Anti Epileptic Drug Adverse Effect in Tertiary Referral HospitalDocument5 pagesPattern of Anti Epileptic Drug Adverse Effect in Tertiary Referral HospitalTikaa RachmawatiNo ratings yet
- Beck 1988Document3 pagesBeck 1988Sebastian RiveroNo ratings yet
- Clinical Features and Visual Outcomes of Optic Neuritis in Chinese ChildrenDocument7 pagesClinical Features and Visual Outcomes of Optic Neuritis in Chinese ChildrenklinkasikNo ratings yet
- Correlation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine PatientsDocument5 pagesCorrelation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine Patientsmara 11No ratings yet
- DR RatnaDocument6 pagesDR RatnaNi Kadek Eno YuliantariNo ratings yet
- Evaluating central fixation for diagnosing amblyopiaDocument4 pagesEvaluating central fixation for diagnosing amblyopiabrontosaurpNo ratings yet
- Test de Sensibilidad Al Contraste para DMAEDocument6 pagesTest de Sensibilidad Al Contraste para DMAEArturo GuilliemNo ratings yet
- Jurnal Reading GlaucomaDocument6 pagesJurnal Reading GlaucomawidyawirapNo ratings yet
- Analysis of The Clinical Diagnosis and Treatment of UveitisDocument7 pagesAnalysis of The Clinical Diagnosis and Treatment of UveitisRhysandNo ratings yet
- Recurrent Optic Neuritis As A Clinical Manifestation in Multiple Sclerosis A Case Report - Anisa Feby ArifaniDocument11 pagesRecurrent Optic Neuritis As A Clinical Manifestation in Multiple Sclerosis A Case Report - Anisa Feby Arifanidenny070111209No ratings yet
- IBEPE StudyDocument8 pagesIBEPE StudyKaran KumarswamyNo ratings yet
- Efficacy and Toxicity of Intravitreous Chemotherapy For Retinoblastoma: Four-Year ExperienceDocument8 pagesEfficacy and Toxicity of Intravitreous Chemotherapy For Retinoblastoma: Four-Year ExperienceSlr RandiNo ratings yet
- Presbyopia Treatment With Eye Drops: An Eight Year Retrospective StudyDocument8 pagesPresbyopia Treatment With Eye Drops: An Eight Year Retrospective Studyilma nafiaNo ratings yet
- Optometry: JournalDocument7 pagesOptometry: JournalsasyaprastiNo ratings yet
- Commentary: The Optic Neuritis Treatment TrialDocument2 pagesCommentary: The Optic Neuritis Treatment TrialEmmanuel Zótico Orellana JiménezNo ratings yet
- VFQ-25 and 10-Item SupplementDocument12 pagesVFQ-25 and 10-Item SupplementAndreea PlesaNo ratings yet
- Aloysius Elyakim, S.Ked 1408010058 Consulent: DR Donny Argie SP - BS Surgery Departement of W.Z. Johannes Hospital-Nusa Cendana Faculty of MedicineDocument30 pagesAloysius Elyakim, S.Ked 1408010058 Consulent: DR Donny Argie SP - BS Surgery Departement of W.Z. Johannes Hospital-Nusa Cendana Faculty of MedicineShandy BethanNo ratings yet
- Results: Four Hundred Eighty-Seven Eyes of 246 Patients (310Document3 pagesResults: Four Hundred Eighty-Seven Eyes of 246 Patients (310Budi IrawanNo ratings yet
- Natissiyan. 2019. Study Visual Functions in Epileptic Patients During DepakoteDocument3 pagesNatissiyan. 2019. Study Visual Functions in Epileptic Patients During DepakoteRuth RachmawatyNo ratings yet
- Um Estudo Da Visualização Excêntrico Formação para Baixa Visão ReabilitaçãoDocument8 pagesUm Estudo Da Visualização Excêntrico Formação para Baixa Visão ReabilitaçãoEduardo VieiraNo ratings yet
- The Caloric Test and The Video Head-Impulse Test in Patients With VertigoDocument7 pagesThe Caloric Test and The Video Head-Impulse Test in Patients With VertigoDevi DaryaningsihNo ratings yet
- Long-Term Visual and Anatomic Results in Treated ROP-JUZ 11-10-22Document24 pagesLong-Term Visual and Anatomic Results in Treated ROP-JUZ 11-10-22areaNo ratings yet
- Krissa and Drentlaw Visual Acuity The Critical Measure!Document18 pagesKrissa and Drentlaw Visual Acuity The Critical Measure!Jolien WalravenNo ratings yet
- Diagnosis Dan Tatalaksana Pasien Dengan Insufisiensi Akomodasi - Sri Hudaya WidihasthaDocument13 pagesDiagnosis Dan Tatalaksana Pasien Dengan Insufisiensi Akomodasi - Sri Hudaya WidihasthamalaNo ratings yet
- Practice Parameter The Role of Corticosteroids in The Management of Acute Monosymptomatic Optic NeuritisDocument9 pagesPractice Parameter The Role of Corticosteroids in The Management of Acute Monosymptomatic Optic Neuritissatyagraha84No ratings yet
- Ecop 09 00286Document11 pagesEcop 09 00286GabrielNo ratings yet
- Classification of Visual Field Abnormalities in Highly Myopic Eyes Without Pathologic ChangeDocument26 pagesClassification of Visual Field Abnormalities in Highly Myopic Eyes Without Pathologic Change钟华No ratings yet
- 31 Rajesh EtalDocument4 pages31 Rajesh EtaleditorijmrhsNo ratings yet
- Treatment of Strabismic AblyopiaDocument5 pagesTreatment of Strabismic AblyopiaYuke PutriNo ratings yet
- High Myopia and Glaucoma Susceptibility The Beijing Eye StudyDocument5 pagesHigh Myopia and Glaucoma Susceptibility The Beijing Eye StudyDickyStevanoZukhriNo ratings yet
- Bo 403 (32301721022)Document8 pagesBo 403 (32301721022)AvinabaNo ratings yet
- Prospective Evaluation of Acupuncture As Treatment For GlaucomaDocument10 pagesProspective Evaluation of Acupuncture As Treatment For Glaucoma16.11Hz MusicNo ratings yet
- A Comparison of Laser Photocoagulation With Cryotherapy For Threshold Retinopathy of Prematurity at 10 Years Part 2. Refractive OutcomeDocument6 pagesA Comparison of Laser Photocoagulation With Cryotherapy For Threshold Retinopathy of Prematurity at 10 Years Part 2. Refractive OutcomeSalma HamdyNo ratings yet
- Relative Afferent Pupillary Defect in Patients With Asymmetric CataractsDocument5 pagesRelative Afferent Pupillary Defect in Patients With Asymmetric CataractsshishichanNo ratings yet
- Monovision Lasik in Emmetropic Presbyopic PatientsDocument7 pagesMonovision Lasik in Emmetropic Presbyopic PatientsIvana Ester Sinta UliNo ratings yet
- Wavefront Optimized vs Custom-Q Treatments for MyopiaDocument11 pagesWavefront Optimized vs Custom-Q Treatments for MyopiaDewi Puspita SariNo ratings yet
- Effects of Cataract Surgery On Vision-Related Quality of Life in Patients With Retinitis Pigmentosa and The Predictive Factors of Quality of Life ImprovementDocument6 pagesEffects of Cataract Surgery On Vision-Related Quality of Life in Patients With Retinitis Pigmentosa and The Predictive Factors of Quality of Life Improvementbrahmani pitanatriNo ratings yet
- Efecto de La Miopia en PevDocument6 pagesEfecto de La Miopia en PevLuciano RuizNo ratings yet
- Anterior Segment Changes During Accommodation in Accommodative EsotropiaDocument10 pagesAnterior Segment Changes During Accommodation in Accommodative EsotropiaOlla TisyaNo ratings yet
- A New Ocular Trauma Score in Pediatric Penetrating Eye InjuriesDocument5 pagesA New Ocular Trauma Score in Pediatric Penetrating Eye InjuriespaulpiensaNo ratings yet
- Disfunciones No Estrabicas 2019Document6 pagesDisfunciones No Estrabicas 2019ana maria carrillo nietoNo ratings yet
- Moon2019 PDFDocument7 pagesMoon2019 PDFGusti Zidni FahmiNo ratings yet
- Higher Order Aberration and Astigmatism in Children With Hyperopic AmblyopiaDocument7 pagesHigher Order Aberration and Astigmatism in Children With Hyperopic AmblyopiaEko WidayantoNo ratings yet
- Visual and Refractive Outcomes of Small-Incision Lenticule Extraction in High Myopia - 5-Year ResultsDocument7 pagesVisual and Refractive Outcomes of Small-Incision Lenticule Extraction in High Myopia - 5-Year Resultspriscilla christina natanNo ratings yet
- AIOC2006Document2 pagesAIOC2006Vidyut RajhansNo ratings yet
- Pediatric Retinal Vascular Diseases: From Angiography to VitrectomyFrom EverandPediatric Retinal Vascular Diseases: From Angiography to VitrectomyNo ratings yet
- IHS Junior Member Verification FormDocument2 pagesIHS Junior Member Verification Formkaysa3No ratings yet
- ICHD 3 Slide KitDocument166 pagesICHD 3 Slide Kitkaysa3No ratings yet
- 18iommodelpolicy TRDocument37 pages18iommodelpolicy TRkaysa3No ratings yet
- IHS Junior Member Verification FormDocument2 pagesIHS Junior Member Verification Formkaysa3No ratings yet
- CAHABA Neurophysiology Evoked Potentials LCDDocument10 pagesCAHABA Neurophysiology Evoked Potentials LCDkaysa3No ratings yet
- Down Syndrome and Attention-Deficit/Hyperactivity Disorder (ADHD)Document8 pagesDown Syndrome and Attention-Deficit/Hyperactivity Disorder (ADHD)kaysa3No ratings yet
- Notice AuthorsDocument9 pagesNotice Authorskaysa3No ratings yet
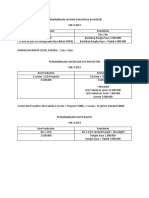
- Backdrop, Screen, Projector, and Photo Booth Rental ComparisonDocument1 pageBackdrop, Screen, Projector, and Photo Booth Rental Comparisonkaysa3No ratings yet
- Icd 9 CM OrthopaediDocument82 pagesIcd 9 CM OrthopaedimoonlightsoantaNo ratings yet
- Sms Masters Project Progress FormDocument6 pagesSms Masters Project Progress Formkaysa3No ratings yet
- Rancang Bangun Aplikasi Penentuan Bahan 4f345af1Document7 pagesRancang Bangun Aplikasi Penentuan Bahan 4f345af1kaysa3No ratings yet
- PregnancyDocument1 pagePregnancyAnonymous pJfAvlNo ratings yet
- Original PassageDocument2 pagesOriginal Passagekaysa3No ratings yet
- DapusDocument1 pageDapuskaysa3No ratings yet
- Lembar FU & BalanceDocument4 pagesLembar FU & Balancekaysa3No ratings yet
- PregnancyDocument1 pagePregnancyAnonymous pJfAvlNo ratings yet
- Sms Masters Research Project Proposal FormDocument4 pagesSms Masters Research Project Proposal Formkaysa3No ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Antepartum HemorrhageDocument48 pagesAntepartum HemorrhageJoshua EvansNo ratings yet
- Rangkuman SlideDocument5 pagesRangkuman Slidekaysa3No ratings yet
- Personality Tes1 FIXDocument4 pagesPersonality Tes1 FIXkaysa3No ratings yet
- Cerebral HemisphereDocument3 pagesCerebral Hemispherekaysa3No ratings yet
- Aging ProcessDocument1 pageAging Processkaysa3No ratings yet
- Agappe Diagnostics Control ValuesDocument1 pageAgappe Diagnostics Control ValuesDinil KannurNo ratings yet
- Health6 q1 Mod2 Selfmanagement v1Document23 pagesHealth6 q1 Mod2 Selfmanagement v1BrianJessenMaweDignosNo ratings yet
- Anthropometric Measurement - Prepare The Materials NeededDocument2 pagesAnthropometric Measurement - Prepare The Materials NeededMemer-alasadNo ratings yet
- 10) One Word That Can Save Your LifeDocument4 pages10) One Word That Can Save Your LifeParesh PathakNo ratings yet
- Breeds of DogsDocument257 pagesBreeds of DogsshayanbzjNo ratings yet
- Maintaining Fluid Balance in Dengue PatientDocument3 pagesMaintaining Fluid Balance in Dengue PatientjhaninahNo ratings yet
- Methodical Pointing For Work of Students On Practical EmploymentDocument32 pagesMethodical Pointing For Work of Students On Practical EmploymentVidhu YadavNo ratings yet
- RD TIPS - 10 Choose Ans From A ListDocument2 pagesRD TIPS - 10 Choose Ans From A ListJess NguyenNo ratings yet
- Biometry: Dr. Sanjay Kumar SarkerDocument67 pagesBiometry: Dr. Sanjay Kumar SarkerNiloy Basak100% (3)
- Pontics (Fixed Prosthodontics Seminar @AmCoFam)Document34 pagesPontics (Fixed Prosthodontics Seminar @AmCoFam)AmericanCornerFamily80% (5)
- 1723-Article Text-7047-4-10-20200605Document7 pages1723-Article Text-7047-4-10-20200605Sarly FebrianaNo ratings yet
- DrMercola SiimLandandJamesDiNicolantonio TheImmunityFixDocument28 pagesDrMercola SiimLandandJamesDiNicolantonio TheImmunityFixRocco LamponeNo ratings yet
- Learning Activity - Coffee PaintingDocument5 pagesLearning Activity - Coffee PaintingElla Mae San BuenaventuraNo ratings yet
- Medical Laboratory Tests: Tang PingDocument42 pagesMedical Laboratory Tests: Tang Pingapi-19916399No ratings yet
- Professional Nursing PhilosophyDocument7 pagesProfessional Nursing Philosophyapi-570211681No ratings yet
- Include Invest: InnovateDocument28 pagesInclude Invest: InnovateAstrisa FaadhilahNo ratings yet
- Different Positions Assumed by A Patient During A Physical Examination ProcedureDocument14 pagesDifferent Positions Assumed by A Patient During A Physical Examination ProcedureAziil LiizaNo ratings yet
- Feed Addditives NEW ANN 211Document44 pagesFeed Addditives NEW ANN 211Mohit BhardwajNo ratings yet
- Diarrhea: For Other Uses, SeeDocument27 pagesDiarrhea: For Other Uses, SeeCrimzonic ShadeNo ratings yet
- Anxiety Attack DLPDocument8 pagesAnxiety Attack DLPAila SastreNo ratings yet
- Ep 306 My Notes Correction Za TichaDocument138 pagesEp 306 My Notes Correction Za TichaKhalid khalifaNo ratings yet
- Ascites (Patient B.U)Document4 pagesAscites (Patient B.U)Max mitchyNo ratings yet
- Acth Stimulation Testing Protocol CanineDocument2 pagesActh Stimulation Testing Protocol CanineSpital Veterinar AndivetNo ratings yet
- Nutrients: Nutrition and Rheumatoid Arthritis in The Omics' EraDocument23 pagesNutrients: Nutrition and Rheumatoid Arthritis in The Omics' EraMikhael FeliksNo ratings yet
- Scrotal Swelling: 'By Kasyeba Sowedi Mbchb-IiiDocument57 pagesScrotal Swelling: 'By Kasyeba Sowedi Mbchb-IiiNinaNo ratings yet
- Nursing Care Plan for Risk of Bleeding During PregnancyDocument4 pagesNursing Care Plan for Risk of Bleeding During PregnancybananakyuNo ratings yet
- UntitledDocument990 pagesUntitledRodica GrecuNo ratings yet
- Material Safety Data Sheet: Silica FumeDocument3 pagesMaterial Safety Data Sheet: Silica FumeEzequiel BeitiaNo ratings yet
- A A PHN IntroDocument354 pagesA A PHN IntroGabriel PhilippeNo ratings yet
- Karolinska Sleepiness Scale (KSS) ChapterDocument2 pagesKarolinska Sleepiness Scale (KSS) ChapterSrija GottiparthiNo ratings yet