You might also like
- Clinicians Guide To AutismDocument20 pagesClinicians Guide To AutismNadia Desanti RachmatikaNo ratings yet
- ADHD and BPD Review PaperDocument15 pagesADHD and BPD Review Paperrupangishah7No ratings yet
- Functional Consequences of Attention-De Ficit Hyperactivity Disorder On Children and Their FamiliesDocument15 pagesFunctional Consequences of Attention-De Ficit Hyperactivity Disorder On Children and Their FamiliesAlba VilaNo ratings yet
- Brain Development in ADHDDocument6 pagesBrain Development in ADHDalexmeduernNo ratings yet
- Case Report II Anxiety DisorderDocument11 pagesCase Report II Anxiety DisorderUnza Ahmad100% (1)
- ADHD: Symptoms and Solutions for Men and Women with Attention Deficit Hyperactivity DisorderFrom EverandADHD: Symptoms and Solutions for Men and Women with Attention Deficit Hyperactivity DisorderNo ratings yet
- InfographicsDocument36 pagesInfographicsalissandra100% (5)
- Neuropsychological Assessment in Children and AdolescentsDocument13 pagesNeuropsychological Assessment in Children and AdolescentsPradeep100% (1)
- Attention-Defi Cit Hyperactivity Disorder 2: SeriesDocument11 pagesAttention-Defi Cit Hyperactivity Disorder 2: SeriesCaio MayrinkNo ratings yet
- Attention Deficit Hyperactivity Disorder in Nepal: A Qualitative StudyDocument9 pagesAttention Deficit Hyperactivity Disorder in Nepal: A Qualitative StudyNijan KhatiwadaNo ratings yet
- NAVIGATE b2 Upperintermediate TEACHER Guide With ResourcesDocument264 pagesNAVIGATE b2 Upperintermediate TEACHER Guide With ResourcesNadine Maksimova100% (2)
- Attention Deficit Hyperactivity Disorder - A Lifespan SynthesisDocument14 pagesAttention Deficit Hyperactivity Disorder - A Lifespan SynthesisNeuroCoaching Portugal100% (1)
- Adhd Research PaperDocument29 pagesAdhd Research PaperEunice Doctolero100% (1)
- Professional Salesmanship: The Salesman'S Responsibilities, Duties, and QualificationsDocument20 pagesProfessional Salesmanship: The Salesman'S Responsibilities, Duties, and Qualificationsryan100% (1)
- Improving Fluency in Young Readers - Fluency InstructionDocument4 pagesImproving Fluency in Young Readers - Fluency InstructionPearl MayMayNo ratings yet
- English For Academic and Professional PurposesDocument13 pagesEnglish For Academic and Professional Purposesjay89% (125)
- Adult Attention-Deficit Hyperactivity Disorder Key Conceptual IssuesDocument12 pagesAdult Attention-Deficit Hyperactivity Disorder Key Conceptual IssuesJason100% (1)
- Teacher's M & E ReportDocument2 pagesTeacher's M & E ReportElbert NatalNo ratings yet
- Cause and Effect EssayDocument5 pagesCause and Effect Essay민수No ratings yet
- Faulty LogicDocument6 pagesFaulty LogicMel Joyce Rumay100% (4)
- Affective Domain Assessment - 1Document17 pagesAffective Domain Assessment - 1Jhener Nonesa100% (1)
- On ADHDDocument14 pagesOn ADHDZara DanishNo ratings yet
- ADHD, Asperger Syndrome, and High-Functioning Autism: ArticleDocument4 pagesADHD, Asperger Syndrome, and High-Functioning Autism: Articlelaura2121No ratings yet
- Develop Med Child Neuro - 2007 - Watemberg - Developmental Coordination Disorder in Children With Attention DeficitDocument6 pagesDevelop Med Child Neuro - 2007 - Watemberg - Developmental Coordination Disorder in Children With Attention DeficitAllana FrósNo ratings yet
- JDN 10089Document18 pagesJDN 10089Lívia MeloNo ratings yet
- The Road To Diagnosis and Treatment in Girls and Boys With ADHD Gender Differences in The Diagnostic ProcessDocument6 pagesThe Road To Diagnosis and Treatment in Girls and Boys With ADHD Gender Differences in The Diagnostic ProcessOana OrosNo ratings yet
- Medical Comorbidities in Children and AdolescentsDocument12 pagesMedical Comorbidities in Children and AdolescentsSalud-psicología-psiquiatria DocenciaNo ratings yet
- Prevalence of Attention-Deficit/hyperactivity and Other Disruptive Behaviour Disorder Symptoms Among Primary School-Age Children in Kayseri, TurkeyDocument13 pagesPrevalence of Attention-Deficit/hyperactivity and Other Disruptive Behaviour Disorder Symptoms Among Primary School-Age Children in Kayseri, TurkeyalfymaydoNo ratings yet
- Research in Developmental Disabilities: Contents Lists Available atDocument10 pagesResearch in Developmental Disabilities: Contents Lists Available atCristinaNo ratings yet
- Group Cognitive RemediationDocument8 pagesGroup Cognitive RemediationFlorencia CalodolceNo ratings yet
- Travail 2.0Document13 pagesTravail 2.0diego caputoNo ratings yet
- Art.2011 Psychoanalytic Conceptualizations of The Internal Object in An ADHD ChildDocument17 pagesArt.2011 Psychoanalytic Conceptualizations of The Internal Object in An ADHD Childdiana noliNo ratings yet
- Research Paper On Attention Deficit Hyperactivity DisorderDocument6 pagesResearch Paper On Attention Deficit Hyperactivity DisorderzxnrvkrifNo ratings yet
- A Different Approach To Rising Rates of ADHD DiagnosisDocument1 pageA Different Approach To Rising Rates of ADHD DiagnosisPaul AsturbiarisNo ratings yet
- A Review of Executive Function Deficits in AutismDocument12 pagesA Review of Executive Function Deficits in AutismKarel GuevaraNo ratings yet
- Research in Developmental Disabilities: J. Keating, J. Bramham, M. DownesDocument13 pagesResearch in Developmental Disabilities: J. Keating, J. Bramham, M. DownesBotez MartaNo ratings yet
- 01 - The Science of ADHD - CHADDDocument6 pages01 - The Science of ADHD - CHADDtenahernanNo ratings yet
- TDAHDocument15 pagesTDAHGabriel QueijoNo ratings yet
- Goodman D2010 The Black Bookof ADHDDocument19 pagesGoodman D2010 The Black Bookof ADHDRadja Er GaniNo ratings yet
- Symptoms Associated With Attention Deficit/ Hyperactivity Disorder and Autism Spectrum Disorders in School-Aged Children Prenatally Exposed To SubstancesDocument8 pagesSymptoms Associated With Attention Deficit/ Hyperactivity Disorder and Autism Spectrum Disorders in School-Aged Children Prenatally Exposed To SubstancesDárcio CasteloNo ratings yet
- Groen Et Al. - 2019 - A Situation-Specific Approach To Measure AttentionDocument32 pagesGroen Et Al. - 2019 - A Situation-Specific Approach To Measure Attentionmaria samNo ratings yet
- A Review of Heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD)Document12 pagesA Review of Heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD)CristinaNo ratings yet
- Castle 2007Document9 pagesCastle 2007stupidshitNo ratings yet
- Antoniou 2021Document15 pagesAntoniou 2021Raul Morales VillegasNo ratings yet
- Genetic Evaluation ReferalsDocument6 pagesGenetic Evaluation Referalsviviana84No ratings yet
- ASD + ADHD Assessment ResourcesDocument28 pagesASD + ADHD Assessment Resourcesعلم ينتفع بهNo ratings yet
- High Intelligence and The Risk of ADHD and Other PsychopathologyDocument7 pagesHigh Intelligence and The Risk of ADHD and Other PsychopathologyVicente CáceresNo ratings yet
- Week 4 Learning Attention Writing and Processing Speed in Typical Children and Children With ADHD Autism Anxiety Depression and Oppositional Defiant DisorderDocument26 pagesWeek 4 Learning Attention Writing and Processing Speed in Typical Children and Children With ADHD Autism Anxiety Depression and Oppositional Defiant DisorderOsmar RomeroNo ratings yet
- Mood Dysregulation - OutcomeDocument18 pagesMood Dysregulation - OutcomeRafael MartinsNo ratings yet
- Autistic Traits in Children With and Without ADHD-Kotte Et Al., 2013Document13 pagesAutistic Traits in Children With and Without ADHD-Kotte Et Al., 2013piso4r1No ratings yet
- Journal Related To Neurodevelopmental DisordersDocument4 pagesJournal Related To Neurodevelopmental DisordersRuchelle SemsemNo ratings yet
- Children With Borderline Intellectual Functioning and Autism Spectrum Disorder: Developmental Trajectories From 4 To 11 Years of AgeDocument8 pagesChildren With Borderline Intellectual Functioning and Autism Spectrum Disorder: Developmental Trajectories From 4 To 11 Years of Ageyeremias setyawanNo ratings yet
- Guia para El TDAHDocument23 pagesGuia para El TDAHEstebanGiraNo ratings yet
- Precision Medicine Care in ADHD The Case For Neural Excitation and InhibitionDocument12 pagesPrecision Medicine Care in ADHD The Case For Neural Excitation and InhibitionDaria DanielNo ratings yet
- Jama DualdxDocument6 pagesJama DualdxGise QuinteroNo ratings yet
- DBP 0b013e3181e121bdDocument14 pagesDBP 0b013e3181e121bdJavier CáceresNo ratings yet
- Attention Deficit Hyperactivity Disorder (ADHD) in Children: A Short Review and LiteratureDocument9 pagesAttention Deficit Hyperactivity Disorder (ADHD) in Children: A Short Review and LiteratureMihaela CherejiNo ratings yet
- Generalidades PDFDocument7 pagesGeneralidades PDFD.MNo ratings yet
- Adhd Research Paper TopicsDocument4 pagesAdhd Research Paper Topicsfvffv0x7100% (1)
- Attentiondeficit-Hyperactivity-Disorder-Adhd-In-Children-A-Movetowards-Developmental-Perspectives-2469-9837-1000171 (1) - DikonversiDocument8 pagesAttentiondeficit-Hyperactivity-Disorder-Adhd-In-Children-A-Movetowards-Developmental-Perspectives-2469-9837-1000171 (1) - Dikonversi6558No ratings yet
- Jurnal AdhdDocument38 pagesJurnal AdhdbimoNo ratings yet
- Epigenetics and ADHDDocument26 pagesEpigenetics and ADHDJulius Cesar RomanNo ratings yet
- Jaramillo Et Al. 2021 - ADHDDocument25 pagesJaramillo Et Al. 2021 - ADHDLaura DecockNo ratings yet
- University of Economics - Academic English - Causes of ADHDDocument9 pagesUniversity of Economics - Academic English - Causes of ADHDLê Hải Anh ThưNo ratings yet
- Peds 20171377Document8 pagesPeds 20171377Nurten Arslan IşıkNo ratings yet
- Child Psychology Psychiatry - 2012 - Simonoff - Severe Mood Problems in Adolescents With Autism Spectrum DisorderDocument10 pagesChild Psychology Psychiatry - 2012 - Simonoff - Severe Mood Problems in Adolescents With Autism Spectrum DisorderlidiaNo ratings yet
- Pork Pies Article 12Document15 pagesPork Pies Article 12Richard SmithNo ratings yet
- Bipolar 2 PDFDocument3 pagesBipolar 2 PDFPrecious Ann ParelNo ratings yet
- Rahul Shaik Kamala Kumari.P Syed Ahmed Basha: BackgroundDocument6 pagesRahul Shaik Kamala Kumari.P Syed Ahmed Basha: BackgroundMutiarahmiNo ratings yet
- 2011 Sleep 34 (4) 503-507Document5 pages2011 Sleep 34 (4) 503-507Avilla Ane LukitoNo ratings yet
- 18iommodelpolicy TRDocument37 pages18iommodelpolicy TRkaysa3No ratings yet
- Retrospective Analysis of N75-P100 Amplitudes and P100 Latencies of Veps in Patients Having One-Sided Visual ProblemsDocument6 pagesRetrospective Analysis of N75-P100 Amplitudes and P100 Latencies of Veps in Patients Having One-Sided Visual Problemskaysa3No ratings yet
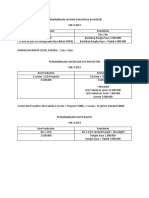
- Perbandingan Ukuran Dan Harga BackdropDocument1 pagePerbandingan Ukuran Dan Harga Backdropkaysa3No ratings yet
- DapusDocument1 pageDapuskaysa3No ratings yet
- Sms Masters Research Project Proposal FormDocument4 pagesSms Masters Research Project Proposal Formkaysa3No ratings yet
- 2013 Sweller Effectis of Speaker Variability On Learning Foreign-Accented EnglishDocument17 pages2013 Sweller Effectis of Speaker Variability On Learning Foreign-Accented EnglishatsushilgNo ratings yet
- Differenciate Between Ralph TylerDocument3 pagesDifferenciate Between Ralph TylerSudheer AyazNo ratings yet
- EWU MBA BC Course OutlinesDocument4 pagesEWU MBA BC Course OutlineskhantabassumanikaNo ratings yet
- Mapeh5 Week1Document12 pagesMapeh5 Week1Arlyn MirandaNo ratings yet
- What Are The Advantages and Disadvantages of The PPP and ESA? PPP (Presentation, Practice, Production) AdvantagesDocument2 pagesWhat Are The Advantages and Disadvantages of The PPP and ESA? PPP (Presentation, Practice, Production) AdvantagesLan NguyễnNo ratings yet
- VinodhDocument4 pagesVinodhapi-511841129No ratings yet
- Lecture 7 CrosstabsDocument20 pagesLecture 7 CrosstabsibmrNo ratings yet
- While Brain Lesson PlanDocument5 pagesWhile Brain Lesson PlanMark Anthony M TolentinoNo ratings yet
- A Systemic Approach To Quality in Early Childhood Services For Children From 3 - 10 021018 V1.0 FINAL - 0 PDFDocument78 pagesA Systemic Approach To Quality in Early Childhood Services For Children From 3 - 10 021018 V1.0 FINAL - 0 PDFBoldsuren BishkhorlooNo ratings yet
- Course Syllabus: Catering 101Document6 pagesCourse Syllabus: Catering 101Sandre WaldenNo ratings yet
- MyTRIZ L2 WorkshopDocument6 pagesMyTRIZ L2 Workshopyudesh.g1857No ratings yet
- Unpacking Curriculum Standards AP LACDocument18 pagesUnpacking Curriculum Standards AP LACLpt DE Quiroz NoelNo ratings yet
- Taking InventoryDocument4 pagesTaking InventoryMaura CrossinNo ratings yet
- M1 Research MethodologyDocument18 pagesM1 Research MethodologyLarissa Rodrigues GCHSNo ratings yet
- Positive Learning Environments Creating and Maintaining Productive Classrooms 1st Edition Nobile Solutions ManualDocument24 pagesPositive Learning Environments Creating and Maintaining Productive Classrooms 1st Edition Nobile Solutions ManualMichaelWrighttcfb100% (49)
- PR2 Worktext Weeks 3-DesamitoDocument1 pagePR2 Worktext Weeks 3-Desamitoneon trueNo ratings yet
- Daily Lesson Log: School District Teacher Grade School Code JUNE 22, 2018 (Friday)Document2 pagesDaily Lesson Log: School District Teacher Grade School Code JUNE 22, 2018 (Friday)Dave ClaridadNo ratings yet
- Service Ecosystem Design:: Josina Vink, Kaisa Koskela-Huotari, Bård Tronvoll, Bo Edvardsson, and Katarina Wetter-EdmanDocument8 pagesService Ecosystem Design:: Josina Vink, Kaisa Koskela-Huotari, Bård Tronvoll, Bo Edvardsson, and Katarina Wetter-EdmanJens Paulin EbdrupNo ratings yet
- Learning Guide #6: Topics: Past SimpleDocument6 pagesLearning Guide #6: Topics: Past SimpleJuan ZuletaNo ratings yet
- Lesson Plan: Industrial University of Ho Chi Minh CityDocument8 pagesLesson Plan: Industrial University of Ho Chi Minh CityThư TrầnNo ratings yet