You might also like
- Information SystemDocument6 pagesInformation SystemFaisal NiaziNo ratings yet
- Tizon, R. - Assignment in NCM 112Document4 pagesTizon, R. - Assignment in NCM 112Royce Vincent TizonNo ratings yet
- According To JMIR PublicationsDocument3 pagesAccording To JMIR PublicationsJanine KhoNo ratings yet
- Topics: in Public Health InformaticsDocument6 pagesTopics: in Public Health InformaticsRonny BudimanNo ratings yet
- Module 14Document5 pagesModule 14camille nina jane navarroNo ratings yet
- Evelyn Hone College: School of Applied Health and SciencesDocument6 pagesEvelyn Hone College: School of Applied Health and SciencesDave0% (1)
- NCM 112 Assignment on Public Health InformaticsDocument4 pagesNCM 112 Assignment on Public Health InformaticsRoyce Vincent TizonNo ratings yet
- Tic 33Document13 pagesTic 33Alexsander SarmientoNo ratings yet
- Mobile Technologies & Community Case Management: Solving The Last Mile in Health Care DeliveryDocument22 pagesMobile Technologies & Community Case Management: Solving The Last Mile in Health Care DeliveryHelen Rocio MartínezNo ratings yet
- Merging Current Health Care Trends: Innovative Perspective in Aging CareDocument57 pagesMerging Current Health Care Trends: Innovative Perspective in Aging CareInosha AberathneNo ratings yet
- Merging Current Health Care Trends: Innovative Perspective in Aging CareDocument75 pagesMerging Current Health Care Trends: Innovative Perspective in Aging CareInosha AberathneNo ratings yet
- What Is EDocument4 pagesWhat Is ECake ManNo ratings yet
- NURSING INFORMATICS Community Health ApplicationsDocument6 pagesNURSING INFORMATICS Community Health ApplicationsThirdy Aquino100% (2)
- What Is The Critical Care Information System? What Comprises It and How Does It Work?Document2 pagesWhat Is The Critical Care Information System? What Comprises It and How Does It Work?FANER, ANGELINE N.No ratings yet
- Health Applications of The InternetDocument70 pagesHealth Applications of The InternetSamson ZaphaniahNo ratings yet
- Abstract The Roleof Health Information Systemsin Achieving Universal Health Coverage AbdullaDocument2 pagesAbstract The Roleof Health Information Systemsin Achieving Universal Health Coverage AbdullaROBBIE PALCENo ratings yet
- Chapter 9.a New TechnologiesDocument9 pagesChapter 9.a New TechnologieslaniNo ratings yet
- E Mental HealthDocument8 pagesE Mental HealthAlter NehebicaNo ratings yet
- Community Health Nursing Also Called Public Health Nursing or Community NursingDocument2 pagesCommunity Health Nursing Also Called Public Health Nursing or Community NursingZanie CruzNo ratings yet
- ConclusionDocument2 pagesConclusionJon SnowNo ratings yet
- Health informatics: Improving patient careFrom EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITRating: 3 out of 5 stars3/5 (1)
- Health Systems Engineering: Building A Better Healthcare Delivery SystemFrom EverandHealth Systems Engineering: Building A Better Healthcare Delivery SystemNo ratings yet
- MIS Model for Process-Oriented HealthcareDocument10 pagesMIS Model for Process-Oriented HealthcareNabeel GondalNo ratings yet
- Benefits of Iclinicsys in The Rural Health Unit of Lupi, Camarines SurDocument5 pagesBenefits of Iclinicsys in The Rural Health Unit of Lupi, Camarines SurattyleoimperialNo ratings yet
- E-Benefits of E-HealthDocument19 pagesE-Benefits of E-HealthKomal HiraveNo ratings yet
- WHO - The Need For Strong Health Information Systems - Rationale For The HMN FrameworkDocument4 pagesWHO - The Need For Strong Health Information Systems - Rationale For The HMN FrameworkHarumNo ratings yet
- Informatics (Requirements)Document4 pagesInformatics (Requirements)aninNo ratings yet
- Part B: The Feasibility and Acceptability of Mi SMART, A Nurse-Led Technology Intervention For Multiple Chronic ConditionsDocument10 pagesPart B: The Feasibility and Acceptability of Mi SMART, A Nurse-Led Technology Intervention For Multiple Chronic Conditionsindah sundariNo ratings yet
- SOC326 Advanced Healthcare TechnologyDocument6 pagesSOC326 Advanced Healthcare TechnologyJasperl Niña MalabuyocNo ratings yet
- Position Paper MhealthDocument23 pagesPosition Paper MhealthAnonymous fFNBawAgwfNo ratings yet
- Business Case Study - CompetitionDocument5 pagesBusiness Case Study - CompetitionDarshanShahNo ratings yet
- HMISDocument6 pagesHMISaryanboxer786No ratings yet
- Health InformationDocument30 pagesHealth InformationifelakojaofinNo ratings yet
- HIS VidDocument8 pagesHIS VidJacqueline HarleNo ratings yet
- Module 4 2Document4 pagesModule 4 2api-642701476No ratings yet
- Hsci 6250Document4 pagesHsci 6250api-642711495No ratings yet
- WHO MBHSS 2010 Section3 WebDocument16 pagesWHO MBHSS 2010 Section3 WebAn Nisa Akhlaqul KarimahNo ratings yet
- Articol Final Rev MG-MK LB Engleza - Clinica Virtuala OnlineDocument14 pagesArticol Final Rev MG-MK LB Engleza - Clinica Virtuala Onlineadina1971No ratings yet
- AHC in NEJM PDFDocument4 pagesAHC in NEJM PDFiggybauNo ratings yet
- Organizing US Healthcare DeliveryDocument20 pagesOrganizing US Healthcare DeliveryJeffersonNo ratings yet
- Medical Informatics Activity No.1Document3 pagesMedical Informatics Activity No.1leomillmendiolaNo ratings yet
- Arnold Ventures Finance Committee Behavioral Health LetterDocument4 pagesArnold Ventures Finance Committee Behavioral Health LetterArnold VenturesNo ratings yet
- Blue River Case StudyDocument19 pagesBlue River Case StudyAnam AbroNo ratings yet
- Overview of ReportsDocument4 pagesOverview of ReportsMuhammad UmerNo ratings yet
- Review of Literature on Nursing Information SystemsDocument6 pagesReview of Literature on Nursing Information SystemsSkyla FiestaNo ratings yet
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument11 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeAnnaNo ratings yet
- State Success Spurs National Innovation in Health Information Exchanges - Shared HealthDocument6 pagesState Success Spurs National Innovation in Health Information Exchanges - Shared Healthlisarx5No ratings yet
- Sent Via Federal Erulemaking Portal: The Medicare Payment Advisory Commission. - July 17, 2020Document4 pagesSent Via Federal Erulemaking Portal: The Medicare Payment Advisory Commission. - July 17, 2020Arnold VenturesNo ratings yet
- Information Technology and Community HealthDocument9 pagesInformation Technology and Community HealthAngel Joy CATALAN (SHS)100% (3)
- Digitalisation of Healthcare in India Promotes Access, Quality and AffordabilityDocument11 pagesDigitalisation of Healthcare in India Promotes Access, Quality and Affordabilityprakhar jainNo ratings yet
- Roadmap For Personalized Health Care April 2011Document8 pagesRoadmap For Personalized Health Care April 2011divith3010No ratings yet
- HMODocument8 pagesHMOrunass_07No ratings yet
- Public Health InformaticsDocument6 pagesPublic Health InformaticsShaina OturdoNo ratings yet
- Shared Nationwide Interoperability Roadmap PDFDocument1 pageShared Nationwide Interoperability Roadmap PDFiggybauNo ratings yet
- 1ausing Information Systems To Improve Population Outcomes Concepts in Program Design and Development Structure SystemsDocument7 pages1ausing Information Systems To Improve Population Outcomes Concepts in Program Design and Development Structure Systemsapi-678571963No ratings yet
- Mhealth Position Paper Discussion DraftDocument39 pagesMhealth Position Paper Discussion DraftSteveEpsteinNo ratings yet
- Mhealth ApplicationsDocument6 pagesMhealth ApplicationsparrexNo ratings yet
- Stress and Coping: Prof. Ronnell D. Dela Rosa, PHD, DNM, RN, RM, LPTDocument7 pagesStress and Coping: Prof. Ronnell D. Dela Rosa, PHD, DNM, RN, RM, LPTRose Lyn Camarista VelascoNo ratings yet
- Ocular and Otic Drugs for Infections and InflammationDocument6 pagesOcular and Otic Drugs for Infections and InflammationRose Lyn Camarista VelascoNo ratings yet
- Ethical Leadership-Is Leadership That Is Directed by Respect For Ethical Beliefs andDocument9 pagesEthical Leadership-Is Leadership That Is Directed by Respect For Ethical Beliefs andRose Lyn Camarista VelascoNo ratings yet
- 1 Introduction To Mental Health and Psychiatric NursingDocument6 pages1 Introduction To Mental Health and Psychiatric NursingRose Lyn Camarista VelascoNo ratings yet
- Amazing Asia-Exploring South AsiaDocument20 pagesAmazing Asia-Exploring South AsiaRose Lyn Camarista VelascoNo ratings yet
- Human AnatomyDocument4 pagesHuman AnatomyRose Lyn Camarista VelascoNo ratings yet
- Immunization in New BornDocument5 pagesImmunization in New BornRose Lyn Camarista VelascoNo ratings yet
- President of Service Centrer President of Service Centrer R RDocument3 pagesPresident of Service Centrer President of Service Centrer R RRose Lyn Camarista VelascoNo ratings yet
- PCAP-C Signs SymptomsDocument2 pagesPCAP-C Signs SymptomsRose Lyn Camarista VelascoNo ratings yet
- New Technologies Related To Public Health Electronic InformationDocument5 pagesNew Technologies Related To Public Health Electronic InformationRose Lyn Camarista VelascoNo ratings yet
- Oxygen Administration Checklist 1Document1 pageOxygen Administration Checklist 1Rose Lyn Camarista VelascoNo ratings yet
- Concept Map: Lupang HinirangDocument2 pagesConcept Map: Lupang HinirangRose Lyn Camarista VelascoNo ratings yet
- Patricia BennerDocument1 pagePatricia BennerRose Lyn Camarista VelascoNo ratings yet
- NoteDocument1 pageNoteRose Lyn Camarista VelascoNo ratings yet
- Ethical Leadership-Is Leadership That Is Directed by Respect For Ethical Beliefs andDocument9 pagesEthical Leadership-Is Leadership That Is Directed by Respect For Ethical Beliefs andRose Lyn Camarista VelascoNo ratings yet
- Anti in Flama ToriesDocument1 pageAnti in Flama ToriesRose Lyn Camarista VelascoNo ratings yet
- Drugs For Disorders of EarDocument6 pagesDrugs For Disorders of EarRose Lyn Camarista VelascoNo ratings yet
- Anatomy and Physiology Abruptio PlacentaDocument2 pagesAnatomy and Physiology Abruptio PlacentaRose Lyn Camarista VelascoNo ratings yet
- Conceptual ModelDocument3 pagesConceptual ModelRose Lyn Camarista VelascoNo ratings yet
- Anti in Flama ToriesDocument1 pageAnti in Flama ToriesRose Lyn Camarista VelascoNo ratings yet
- Conceptual ModelDocument3 pagesConceptual ModelRose Lyn Camarista VelascoNo ratings yet
- HydrocephalusDocument14 pagesHydrocephalusRose Lyn Camarista VelascoNo ratings yet
- 8 HydroDocument1 page8 HydroRose Lyn Camarista VelascoNo ratings yet
- Pathophysiology of Non-Communicating Congenital HydrocephalusDocument3 pagesPathophysiology of Non-Communicating Congenital HydrocephalusRose Lyn Camarista VelascoNo ratings yet
- Drug Study CaseDocument7 pagesDrug Study CaseRose Lyn Camarista VelascoNo ratings yet
- Business Plan Template 16x9Document5 pagesBusiness Plan Template 16x9Andika Wirasatria DonyNo ratings yet
- Corporation Investors Stock Shareholders Liability Assets Publicly-Held Corporation BondsDocument1 pageCorporation Investors Stock Shareholders Liability Assets Publicly-Held Corporation BondsRose Lyn Camarista VelascoNo ratings yet
- Procedure PerformedDocument1 pageProcedure PerformedRose Lyn Camarista VelascoNo ratings yet
- Piaget vs Erikson: A Comparison of Two Major Developmental TheoriesDocument4 pagesPiaget vs Erikson: A Comparison of Two Major Developmental TheoriesRose Lyn Camarista VelascoNo ratings yet
- Gtu Mba BookDocument7 pagesGtu Mba BookAkshat PrajapatiNo ratings yet
- Interdisciplinary Project 1Document11 pagesInterdisciplinary Project 1api-424250570No ratings yet
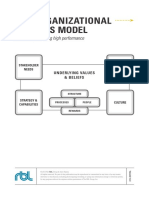
- Organizational+Systems+Model+ +Dave+HannaDocument12 pagesOrganizational+Systems+Model+ +Dave+HannaYashu BhimaniNo ratings yet
- Understanding Business Processes and IS ModelingDocument13 pagesUnderstanding Business Processes and IS ModelingMardhiah RamlanNo ratings yet
- Dr. Amor Lazzez: Overview of Systems Integration: Challenges and DrivesDocument20 pagesDr. Amor Lazzez: Overview of Systems Integration: Challenges and DrivesArsenia DuldulaoNo ratings yet
- TOAST: Online ASPIC+ Implementation: Frontiers in Artificial Intelligence and Applications January 2012Document3 pagesTOAST: Online ASPIC+ Implementation: Frontiers in Artificial Intelligence and Applications January 2012patriciaNo ratings yet
- UserManualDocument12 pagesUserManualChrisrephot Delos ReyesNo ratings yet
- ApprovedDocument52 pagesApprovedZig Kapingiri LuijNo ratings yet
- Chapter One: Managing and The Manager's Job: EffectiveDocument26 pagesChapter One: Managing and The Manager's Job: EffectiveLuna VeraNo ratings yet
- The Collected Essays of Dewey B LarsonDocument148 pagesThe Collected Essays of Dewey B LarsonDavid WaycasterNo ratings yet
- IOT Based Solar Dryer and Irrigation SystemDocument8 pagesIOT Based Solar Dryer and Irrigation SystemIJRASETPublicationsNo ratings yet
- SoftWARE Engineering Lab Program 2 To 7Document16 pagesSoftWARE Engineering Lab Program 2 To 7Abhishek MathurNo ratings yet
- 00 - ST-PCS7SYS - V8.0 - Register 20 enDocument1 page00 - ST-PCS7SYS - V8.0 - Register 20 enSohail AhmedNo ratings yet
- Treinamento PP DS InglesDocument56 pagesTreinamento PP DS InglesponsiaNo ratings yet
- Real-Time SystemsDocument29 pagesReal-Time Systemshowida nafaaNo ratings yet
- Sheffi Urban Trans Networks 18 42 (1) 12 25Document14 pagesSheffi Urban Trans Networks 18 42 (1) 12 25kevinNo ratings yet
- Canyonland History DocumentDocument74 pagesCanyonland History Documentapi-316835550100% (1)
- SEPMDocument21 pagesSEPMPRAKNo ratings yet
- Lecture 2 B.SC (Construction Management)Document54 pagesLecture 2 B.SC (Construction Management)mohamed elnourNo ratings yet
- Location Awareness in Cognitive Radio NetworksDocument135 pagesLocation Awareness in Cognitive Radio Networksnitish raguramanNo ratings yet
- Finite State MachineDocument20 pagesFinite State MachineClyde CauchiNo ratings yet
- QHSEOFFICE DNV-MANAGING-THE-RISKS-of-BLACKOUTDocument52 pagesQHSEOFFICE DNV-MANAGING-THE-RISKS-of-BLACKOUTRitmuri HateganeNo ratings yet
- A S WatsonDocument13 pagesA S WatsonDENNIS KIHUNGINo ratings yet
- CS2301 SOFTWARE ENGINEERING - Important Questions With Answers PDFDocument14 pagesCS2301 SOFTWARE ENGINEERING - Important Questions With Answers PDFlucifer100% (3)
- English CG!Document247 pagesEnglish CG!Ronah Vera B. TobiasNo ratings yet
- Career Planning Career PlanningDocument6 pagesCareer Planning Career PlanningMajor SaifNo ratings yet
- Systems Engineering Management: MSE607B Chapter 6 Part I of II System Engineering Program PlanningDocument41 pagesSystems Engineering Management: MSE607B Chapter 6 Part I of II System Engineering Program PlanningWajdiNo ratings yet
- Document Types and Naming ConventionsDocument17 pagesDocument Types and Naming Conventionssmm999999999No ratings yet
- Meeker 2014Document26 pagesMeeker 2014Carlos Bathuel Ramirez P.No ratings yet
- IPIECA - IOGP - Oil Spill Response Introduction - GPGDocument24 pagesIPIECA - IOGP - Oil Spill Response Introduction - GPGseawolf50No ratings yet