You might also like
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingFrom EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingNo ratings yet
- COVID Guideline v2 6 5 21Document14 pagesCOVID Guideline v2 6 5 21Kamrul AhsanNo ratings yet
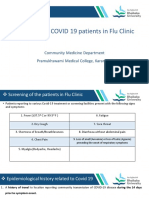
- Screening For COVID-19Document11 pagesScreening For COVID-19ruhulcoc1No ratings yet
- Covid-19 Protocol Severity and ManagementDocument4 pagesCovid-19 Protocol Severity and ManagementMardy DeponaNo ratings yet
- SJDH Chester Kyle Fernandez Risk AssessmentDocument8 pagesSJDH Chester Kyle Fernandez Risk AssessmentChester KyleNo ratings yet
- MoHP Protocol For COVID19 November 2020Document28 pagesMoHP Protocol For COVID19 November 2020medya dostorNo ratings yet
- Laboratory biosafety risk assessment for COVID-19 antigen and PCR testingDocument8 pagesLaboratory biosafety risk assessment for COVID-19 antigen and PCR testingChester KyleNo ratings yet
- Philippine Pediatric Society Guidelines on Screening and Managing Pediatric COVID-19 (39Document20 pagesPhilippine Pediatric Society Guidelines on Screening and Managing Pediatric COVID-19 (39Obree Mdn-RfnNo ratings yet
- Child With Fever in ER Non Covid 19Document6 pagesChild With Fever in ER Non Covid 19Suwandi AlghozyNo ratings yet
- Clinical Management Guidelines For COVID-19 Infections - 1201Document8 pagesClinical Management Guidelines For COVID-19 Infections - 1201Ehtisham KhattakNo ratings yet
- Guidelines Treatment Protocol April 2021 MergedDocument78 pagesGuidelines Treatment Protocol April 2021 Mergedjose j kochuparambilNo ratings yet
- 1.nurse Preparedness Training Against 3rd Wave of CovidDocument52 pages1.nurse Preparedness Training Against 3rd Wave of CovidyeshumasihNo ratings yet
- Covid 19/sars Cov 2Document33 pagesCovid 19/sars Cov 2Wazeed BashaNo ratings yet
- Clinical Management Protocol: Covid-19Document23 pagesClinical Management Protocol: Covid-19Gokul ChandolaNo ratings yet
- A3132020184314919 PDFDocument20 pagesA3132020184314919 PDFAnushka SoniNo ratings yet
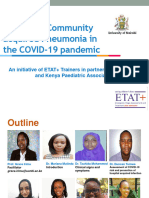
- Community Acquired PNEUMONIADocument4 pagesCommunity Acquired PNEUMONIAjljoioiuNo ratings yet
- DR Irawaty CAP MANAGEMENT UPDATE BASED ON NEW GUIDELINESDocument35 pagesDR Irawaty CAP MANAGEMENT UPDATE BASED ON NEW GUIDELINESKornelis AribowoNo ratings yet
- Management of COVID-19 in ChildrenDocument10 pagesManagement of COVID-19 in ChildrenJuhi NeogiNo ratings yet
- Is It Dengue or Is It COVIDDocument5 pagesIs It Dengue or Is It COVIDKika PunsalanNo ratings yet
- Clincal Case Presentation 5Document32 pagesClincal Case Presentation 5api-635948254No ratings yet
- Clinical Management Protocol For Covid-19: (In Adults)Document22 pagesClinical Management Protocol For Covid-19: (In Adults)Ahmed TarigNo ratings yet
- Kerala State Covid 19 Treatment Guidelines V4 August 5Document124 pagesKerala State Covid 19 Treatment Guidelines V4 August 5Akshay RamakrishnanNo ratings yet
- Coronavirus disease 2019: Understanding transmission, clinical manifestations, diagnosis and treatmentDocument60 pagesCoronavirus disease 2019: Understanding transmission, clinical manifestations, diagnosis and treatmentbekbekk cabahugNo ratings yet
- PNEUMONIA: Phases, Manifestations, and DiagnosisDocument47 pagesPNEUMONIA: Phases, Manifestations, and DiagnosisNica Lopez FernandezNo ratings yet
- Session 4-Management of Paediatric COVID19Document24 pagesSession 4-Management of Paediatric COVID19Uncertain NeuronNo ratings yet
- Rahma Dan CAPDocument17 pagesRahma Dan CAPpeterNo ratings yet
- Covid19 - Pathophysiology and ManagementDocument51 pagesCovid19 - Pathophysiology and ManagementMyraflor CaroNo ratings yet
- 63e61cbd0e9c35001a1a86df 1676025084 CoViDDocument21 pages63e61cbd0e9c35001a1a86df 1676025084 CoViDAlthea Delos reyesNo ratings yet
- Manage COVID-19 with Clinical ProtocolDocument22 pagesManage COVID-19 with Clinical ProtocoleswarNo ratings yet
- ClinicalManagementProtocolforCOVID19dated27062020 PDFDocument22 pagesClinicalManagementProtocolforCOVID19dated27062020 PDFKaran ChhabraNo ratings yet
- ClinicalManagementProtocolforCOVID19dated27062020 PDFDocument22 pagesClinicalManagementProtocolforCOVID19dated27062020 PDFKaran ChhabraNo ratings yet
- Cap ReportDocument49 pagesCap ReportAdrian Levi MagbojosNo ratings yet
- Pneumonia in COVID -19 ContextDocument70 pagesPneumonia in COVID -19 ContextdrshekarforyouNo ratings yet
- Guidelines On Clinical Management of Severe Acute Respiratory Illness PDFDocument11 pagesGuidelines On Clinical Management of Severe Acute Respiratory Illness PDFSandeepNo ratings yet
- Rahma Dan CAPDocument17 pagesRahma Dan CAPpeterNo ratings yet
- COVID19Document79 pagesCOVID19Mohamad El SharNo ratings yet
- Cip On CovidDocument40 pagesCip On CovidLorenz L. Llamas IIINo ratings yet
- Cough: Diagnosis and ManagementDocument65 pagesCough: Diagnosis and Managementsonu_23No ratings yet
- ClinicalManagementProtocolforCOVID19 PDFDocument22 pagesClinicalManagementProtocolforCOVID19 PDFGHAPRC RUDRAPURNo ratings yet
- Covid - 19: Budi SutedjaDocument39 pagesCovid - 19: Budi SutedjaVayaMahdiyaIzzatiNo ratings yet
- Acute Lower Respiratory InfectionsDocument28 pagesAcute Lower Respiratory InfectionsAs Minhas OrigensNo ratings yet
- COVID-19Document38 pagesCOVID-19PPI RSPKUMuhCepuNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICinstalasi kamar bedah RSMINo ratings yet
- Typhoid FeverDocument27 pagesTyphoid FeverDonn Alcayde100% (2)
- 06NTD 2022 - Managing Dengue in Children: An UpdateDocument40 pages06NTD 2022 - Managing Dengue in Children: An UpdateInstitute for Clinical ResearchNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICFirdaus FamilyNo ratings yet
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- Guidelines On Clinical Management of Covid - 19Document15 pagesGuidelines On Clinical Management of Covid - 19shah007zaadNo ratings yet
- 35-Swine Flue 09Document36 pages35-Swine Flue 09Sajjad Ali KhanNo ratings yet
- COVID-19 Protocol July 2022Document36 pagesCOVID-19 Protocol July 2022Mobile AsdNo ratings yet
- In Managing Early Using: New Normal Respiratory Distress HFNTDocument51 pagesIn Managing Early Using: New Normal Respiratory Distress HFNTRaditya DidotNo ratings yet
- Low-Risk CAP ModuleDocument5 pagesLow-Risk CAP ModuleJayson Joseph AngloNo ratings yet
- Pneumonia symptoms, causes, treatment in childrenDocument14 pagesPneumonia symptoms, causes, treatment in childrenRafael Florez HernandezNo ratings yet
- Risk Assessment TemplateDocument9 pagesRisk Assessment TemplateChester KyleNo ratings yet
- CASE 2 PneumoniaDocument12 pagesCASE 2 PneumoniaKenneth MiguelNo ratings yet
- Meningitis Is The Inflammation of The Protective MembranesDocument7 pagesMeningitis Is The Inflammation of The Protective MembranesAtinder PalNo ratings yet
- 3 Types: ApneaDocument5 pages3 Types: ApneaSanthosh KumarNo ratings yet
- Presentation By:-Capt Narendra Sarlam MH GwaliorDocument66 pagesPresentation By:-Capt Narendra Sarlam MH Gwalioryash shrivastavaNo ratings yet
- Case - PneumoniaDocument31 pagesCase - PneumoniaKimm Delos ReyesNo ratings yet
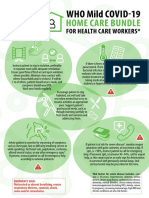
- WHO COVID-19-Home-Care-BundleDocument2 pagesWHO COVID-19-Home-Care-BundleOCSAF - P2LT PUNSALAN MCNo ratings yet
- 42 bpsc03 InstructionDocument1 page42 bpsc03 InstructionAbdul JalilNo ratings yet
- Global Strategy For The Diagnosis and Management of Acute Kidney Injury in Patients With Liver CirrhosisDocument10 pagesGlobal Strategy For The Diagnosis and Management of Acute Kidney Injury in Patients With Liver CirrhosisAbdul JalilNo ratings yet
- Bangladesh Railway e TicketDocument1 pageBangladesh Railway e TicketAbdul JalilNo ratings yet
- What's New in COVID-19 GuidelinesDocument2 pagesWhat's New in COVID-19 GuidelinesAbdul JalilNo ratings yet
- Continue: Sharma Mohan Textbook of Tuberculosis PDFDocument2 pagesContinue: Sharma Mohan Textbook of Tuberculosis PDFAbdul JalilNo ratings yet
- Bangladesh Railway e TicketDocument1 pageBangladesh Railway e TicketAbdul JalilNo ratings yet
- TH, EL®: I I V7i-Life RM Fin Flfin3Document1 pageTH, EL®: I I V7i-Life RM Fin Flfin31114 Ariful IslamNo ratings yet
- Final Anti TB in SP - SituationDocument50 pagesFinal Anti TB in SP - SituationAbdul JalilNo ratings yet
- Strong Letter RecommendationDocument2 pagesStrong Letter RecommendationJorge Luis Sánchez Alarcón100% (1)
- Bangladesh College of Physicians and Surgeons (BCPS)Document6 pagesBangladesh College of Physicians and Surgeons (BCPS)Abdul JalilNo ratings yet
- Maitree Express: 1. Name and Number of The TrainDocument3 pagesMaitree Express: 1. Name and Number of The TrainShahriar Al KabirNo ratings yet
- NDD Operational GuidelinesDocument32 pagesNDD Operational GuidelinesAbdul JalilNo ratings yet
- A Child With Joint PainDocument49 pagesA Child With Joint PainAbdul JalilNo ratings yet
- Welcome To Journal Presentation: Dr. Md. Ali Akbar Khan (Rakib) MD (Cardiology) Phase A Resident NicvdDocument50 pagesWelcome To Journal Presentation: Dr. Md. Ali Akbar Khan (Rakib) MD (Cardiology) Phase A Resident NicvdAbdul JalilNo ratings yet
- Notice: Bangladesh of Physicians andDocument4 pagesNotice: Bangladesh of Physicians andAbdul JalilNo ratings yet
- Normal trachea is in midlineDocument52 pagesNormal trachea is in midlineAbdul JalilNo ratings yet
- Totali 4: NotificationDocument2 pagesTotali 4: NotificationAbdul JalilNo ratings yet
- Fcps 25Document1 pageFcps 25Abdul JalilNo ratings yet
- Bangladesh Railway e TicketDocument1 pageBangladesh Railway e TicketAbdul JalilNo ratings yet
- BD Home Profit Rate Islamic Novmeber As Per New Circular Islamic BankDocument1 pageBD Home Profit Rate Islamic Novmeber As Per New Circular Islamic BankAbdul JalilNo ratings yet
- Hypertrophic Cardiomyopathy: Life WithDocument34 pagesHypertrophic Cardiomyopathy: Life WithAbdul JalilNo ratings yet
- Admission Test Result: March, 2021: Faculty: Faculty of Medicine Course: MD Discipline: NeurologyDocument1 pageAdmission Test Result: March, 2021: Faculty: Faculty of Medicine Course: MD Discipline: NeurologyAbdul JalilNo ratings yet
- Choose The Stethoscope That Helps You Achieve Your Best.: Classic Cardiology Electronic LightweightDocument2 pagesChoose The Stethoscope That Helps You Achieve Your Best.: Classic Cardiology Electronic LightweightAbdul JalilNo ratings yet
- Student Short Stature Approach HANDOUT PDFDocument45 pagesStudent Short Stature Approach HANDOUT PDFAbdul JalilNo ratings yet
- Guidelines Station 5 ScenariosDocument37 pagesGuidelines Station 5 ScenariosAbdul JalilNo ratings yet
- (Scan) PDFDocument17 pages(Scan) PDFAbdul JalilNo ratings yet
- 2021 Main Residency Match Calendar: S 12:00 P.M. ETDocument2 pages2021 Main Residency Match Calendar: S 12:00 P.M. ETAbdul JalilNo ratings yet
- Obstructive Sleep Apnoea (OSA) Definition of Obstructive Sleep Apnoea (OSA)Document4 pagesObstructive Sleep Apnoea (OSA) Definition of Obstructive Sleep Apnoea (OSA)Abdul JalilNo ratings yet
- Towerblock Rota Start of 2019 Is Established Commune AreaDocument47 pagesTowerblock Rota Start of 2019 Is Established Commune AreaLingNo ratings yet
- Handbook AdhesiveDocument68 pagesHandbook Adhesivec100% (2)
- Diabetes PDFDocument5 pagesDiabetes PDFErica MailigNo ratings yet
- Soft Skills in The Pharmacy Curriculum: Lilian M. AzzopardiDocument14 pagesSoft Skills in The Pharmacy Curriculum: Lilian M. Azzopardishailendra patilNo ratings yet
- Sanjeevini Combination Sheet For SSC 13 Sinus and ColdDocument1 pageSanjeevini Combination Sheet For SSC 13 Sinus and ColdEduardoNo ratings yet
- Perfume Notes & FamiliesDocument24 pagesPerfume Notes & Familiesmohamed tharwatNo ratings yet
- Metal Hose Manual 1301 - Uk - 8 - 05 - 20 - PDFDocument388 pagesMetal Hose Manual 1301 - Uk - 8 - 05 - 20 - PDFklich77No ratings yet
- PSC NKDocument44 pagesPSC NKDito Aprian100% (2)
- Stress in The WorkplaceDocument10 pagesStress in The WorkplaceWendyLu32100% (1)
- Production of Non Ferrous MetalsDocument68 pagesProduction of Non Ferrous MetalsDrTrinath TalapaneniNo ratings yet
- CLC Customer Info Update Form v3Document1 pageCLC Customer Info Update Form v3John Philip Repol LoberianoNo ratings yet
- The Logic of Immunity Deciphering An EnigmaDocument204 pagesThe Logic of Immunity Deciphering An EnigmaSatyabrataSahaNo ratings yet
- Long Life Lithium Battery TitleDocument2 pagesLong Life Lithium Battery Titleluis_claudino6263No ratings yet
- IJST - Vol (7) - No (4) December 2012Document153 pagesIJST - Vol (7) - No (4) December 2012Taghreed hashim AlnoorNo ratings yet
- Hydraulic Fluids in Mobile Application Re98128 - 2015-06 - Online PDFDocument13 pagesHydraulic Fluids in Mobile Application Re98128 - 2015-06 - Online PDFDennis Huanuco CcamaNo ratings yet
- Starch Industry Effluent Treatment PlantDocument30 pagesStarch Industry Effluent Treatment PlantBSridhar50% (2)
- Gualberto Vs GualbertoDocument16 pagesGualberto Vs GualbertoTalina BinondoNo ratings yet
- Valtek Beta Positioners: For Control ValvesDocument8 pagesValtek Beta Positioners: For Control Valvesابزار دقیقNo ratings yet
- Đề Ôn Thi Tuyển Sinh Lớp 6 Môn Tiếng AnhDocument7 pagesĐề Ôn Thi Tuyển Sinh Lớp 6 Môn Tiếng AnhHoa TrònNo ratings yet
- 6 Review of Related LiteratureDocument2 pages6 Review of Related Literaturerusty0% (2)
- Prayer of Protection Against The PlagueDocument9 pagesPrayer of Protection Against The PlagueJuan Jaylou Ante100% (2)
- Intelli Trac X1Document2 pagesIntelli Trac X1nadjibnetNo ratings yet
- A Review On The Biosurfactants Properties Types and Its Applications 2090 4541 1000248Document6 pagesA Review On The Biosurfactants Properties Types and Its Applications 2090 4541 1000248Mo NassifNo ratings yet
- GFT 4 Rail Installation Guide 20171219 1Document31 pagesGFT 4 Rail Installation Guide 20171219 1Comsip400No ratings yet
- 19 - Kyocera Milling - Endmill - Radius - Ball-Nose 2010-2011 (ENG)Document24 pages19 - Kyocera Milling - Endmill - Radius - Ball-Nose 2010-2011 (ENG)karadimasNo ratings yet
- Reviewer Ansc 111Document6 pagesReviewer Ansc 111Jeric MadroñoNo ratings yet
- Tle9agricropproduction q1 m5 ProvidingworksupportinaccordancewithOHSforhorticulturalproductionwork v3Document26 pagesTle9agricropproduction q1 m5 ProvidingworksupportinaccordancewithOHSforhorticulturalproductionwork v3Marycon Lao NacitoNo ratings yet
- GCSE Biology - Homeostasis - WorksheetDocument2 pagesGCSE Biology - Homeostasis - WorksheetalexNo ratings yet
- Quality Management System: ISO 9001 - 2000 ClausesDocument18 pagesQuality Management System: ISO 9001 - 2000 ClausesRambabuNo ratings yet
- ASME I & ASME VIII FundamentalsDocument55 pagesASME I & ASME VIII FundamentalsFabio Peres de Lima100% (2)
- Pressure VesselDocument114 pagesPressure Vesseldanemsal100% (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)