You might also like
- Application For Employment: Family BackgroundDocument3 pagesApplication For Employment: Family BackgroundPrincess Ordonio100% (1)
- Application Form SEMPHILDocument3 pagesApplication Form SEMPHILDeanne Reyes75% (4)
- 1964-1986 OMC Sterndrive ManualDocument572 pages1964-1986 OMC Sterndrive ManualBarry Pieters75% (4)
- Application Form: Personal BiodataDocument2 pagesApplication Form: Personal BiodataNoela TiaganNo ratings yet
- D20 Modern - Evil Dead PDFDocument39 pagesD20 Modern - Evil Dead PDFLester Cooper100% (1)
- Employee Verification FormDocument4 pagesEmployee Verification FormHarshit Suri100% (9)
- Backgroud Check Form With LOADocument6 pagesBackgroud Check Form With LOASho VictoriaNo ratings yet
- Kra (Key Result Area) 1 Marketing Manager Measurement Factor KPI/TargetDocument3 pagesKra (Key Result Area) 1 Marketing Manager Measurement Factor KPI/TargetAmit Shukla100% (2)
- Presentation of E Commerce Website ProjectDocument13 pagesPresentation of E Commerce Website ProjectSibu Star25% (4)
- Sample Demotion Letter After ReviewerDocument2 pagesSample Demotion Letter After Reviewerusman466No ratings yet
- Learning Recovery Plan2Document8 pagesLearning Recovery Plan2Remelyn RodrigoNo ratings yet
- Age of Empires III Standard Manual PDFDocument80 pagesAge of Empires III Standard Manual PDFnico100% (8)
- Job Application Form Template 2Document8 pagesJob Application Form Template 2marklola12No ratings yet
- An Introduction To The Study of Medieval Latin VersificationDocument246 pagesAn Introduction To The Study of Medieval Latin VersificationGregorio Gonzalez Moreda100% (1)
- OBE-Syllabus Photography 2015Document8 pagesOBE-Syllabus Photography 2015Frederick Eboña100% (1)
- Kotak Joining Kit PDFDocument18 pagesKotak Joining Kit PDFDhiraj SirsatNo ratings yet
- Joining Report Passport PhotoDocument7 pagesJoining Report Passport PhotoPranav SinghNo ratings yet
- MAP Application Form V2 Current 4Document5 pagesMAP Application Form V2 Current 4nickyNo ratings yet
- Teleysia Employee Joining FormDocument2 pagesTeleysia Employee Joining FormdevdasNo ratings yet
- Candidate Info SheetDocument5 pagesCandidate Info SheetSri KumaranNo ratings yet
- BGV Form Template - HBIDocument8 pagesBGV Form Template - HBIMarivic CaderaoNo ratings yet
- EMPLOYMENT VERIFICATION FORMDocument8 pagesEMPLOYMENT VERIFICATION FORMgopikiran6No ratings yet
- Candidate Info SheetDocument4 pagesCandidate Info SheetKarthik cNo ratings yet
- Employment ApplicationDocument3 pagesEmployment ApplicationKeyser HHNo ratings yet
- Application Form 1Document5 pagesApplication Form 1harryNo ratings yet
- EWRB Application FormDocument2 pagesEWRB Application FormBeverly Gene Geraldizo - DañasNo ratings yet
- Coforge Background Check FormDocument3 pagesCoforge Background Check FormmgdawaraNo ratings yet
- KLBM Application For Employment FormDocument4 pagesKLBM Application For Employment FormRyn nordinNo ratings yet
- Zimbabwe Application For RegistrationDocument9 pagesZimbabwe Application For Registrationpeemutongoza051No ratings yet
- Application Form - GET-2020 PDFDocument4 pagesApplication Form - GET-2020 PDFkshitij shahNo ratings yet
- HRD P 51584 FormDocument5 pagesHRD P 51584 FormTiwari's Virtual ClassesNo ratings yet
- Application Form Knockmitten Youth and Community CentreDocument7 pagesApplication Form Knockmitten Youth and Community Centreapi-412313510No ratings yet
- Revised GSK Application For Employment - With Criminal DisclosureDocument4 pagesRevised GSK Application For Employment - With Criminal DisclosurePravallika Rao TadepalliNo ratings yet
- Application FormDocument6 pagesApplication FormAkarshit NandeshwarNo ratings yet
- Voltas Limited: MR/MS. First Name) (Middle Name) (Surname)Document5 pagesVoltas Limited: MR/MS. First Name) (Middle Name) (Surname)nspatil008No ratings yet
- Application Form Cook TempDocument8 pagesApplication Form Cook Tempmasoncherry2010No ratings yet
- Crest Internship FormDocument4 pagesCrest Internship FormAna Nur MashitahNo ratings yet
- Ctrltech e FormDocument13 pagesCtrltech e FormArshad KhalidNo ratings yet
- ZDA Job Application FormDocument5 pagesZDA Job Application FormSaim SultanNo ratings yet
- 02 Background Check FormsDocument8 pages02 Background Check FormsKisha MarieNo ratings yet
- Employment Application FormDocument4 pagesEmployment Application FormYopie FebriantoNo ratings yet
- GAVL Candidate Application Form-WordDocument2 pagesGAVL Candidate Application Form-WordGAURAV MASKARNo ratings yet
- Application Form (Eng) - Plaza KuninganDocument3 pagesApplication Form (Eng) - Plaza KuninganBabas KunNo ratings yet
- SFL Joining KitDocument11 pagesSFL Joining Kitdharam singhNo ratings yet
- Personal Information: Date of Birth Marital Status Single / MarriedDocument4 pagesPersonal Information: Date of Birth Marital Status Single / Marriedfly2m2k86fly2m2kNo ratings yet
- Application For Internship CollegeDocument3 pagesApplication For Internship CollegeAly SiazonNo ratings yet
- INSTRUCTIONSDocument5 pagesINSTRUCTIONSNitiNo ratings yet
- Application Form - RH Petrogas (v.3.2-2020-F)Document4 pagesApplication Form - RH Petrogas (v.3.2-2020-F)Tri MiaNo ratings yet
- Vanguard - Job Application Form For ABS-CBN V3Document5 pagesVanguard - Job Application Form For ABS-CBN V3RRNo ratings yet
- Application ehDocument3 pagesApplication ehdmorancie69No ratings yet
- Supplementary Employment Application Form NdvoDocument7 pagesSupplementary Employment Application Form NdvoSamuel MutahiNo ratings yet
- SATS Executive Application GuideDocument5 pagesSATS Executive Application GuidejammushaNo ratings yet
- TFAT Application FormDocument5 pagesTFAT Application FormMadeleineNo ratings yet
- Temenos India Employee ProfileDocument5 pagesTemenos India Employee ProfileTony FreekzNo ratings yet
- Employee Application FormDocument5 pagesEmployee Application FormRatih. Angelina97No ratings yet
- RFCL Job Application InsightsDocument6 pagesRFCL Job Application InsightsSwarup NayakNo ratings yet
- Halo - Application FormDocument5 pagesHalo - Application Formsh8132397No ratings yet
- Personal History Form EComm Org - NewDocument4 pagesPersonal History Form EComm Org - NewRamNo ratings yet
- Updated BGV FORM and LOADocument7 pagesUpdated BGV FORM and LOAReymar BanaagNo ratings yet
- DEMO RELIANCE Application Form - GET 2022Document4 pagesDEMO RELIANCE Application Form - GET 2022Mouhanit LimbachiyaNo ratings yet
- Carolfortuna - Project Fuse BV CheckDocument7 pagesCarolfortuna - Project Fuse BV CheckCarol Mundin FortunaNo ratings yet
- Application For Employment FormDocument2 pagesApplication For Employment FormJohn JeffreyNo ratings yet
- Application For EmploymentDocument4 pagesApplication For EmploymentJain AzarNo ratings yet
- Employee Department (Managment)Document2 pagesEmployee Department (Managment)Engr Touseef GhalibNo ratings yet
- US Technology International Pvt. LTD: Application For EmploymentDocument5 pagesUS Technology International Pvt. LTD: Application For EmploymentJagadeesh VarmaNo ratings yet
- Artech Infosystems PVT LTD Background Verification FormDocument7 pagesArtech Infosystems PVT LTD Background Verification FormThiyagesh DhandapaniNo ratings yet
- Bursaries Learner Registration Form v1Document3 pagesBursaries Learner Registration Form v1nonkululekoh2No ratings yet
- 0HRF4 Application Form General November 2019Document12 pages0HRF4 Application Form General November 2019Erick SungaNo ratings yet
- The Ultimate Cover Letter Mastery: From Overlooked To Shortlisted And InterviewedFrom EverandThe Ultimate Cover Letter Mastery: From Overlooked To Shortlisted And InterviewedNo ratings yet
- Fixed Term and Temp Template LettersDocument6 pagesFixed Term and Temp Template LettersSvsSridharNo ratings yet
- Job Position Details-K.williamDocument1 pageJob Position Details-K.williamSvsSridharNo ratings yet
- Profile VTV 1Document4 pagesProfile VTV 1SvsSridharNo ratings yet
- Daily status-TSI, SODocument2 pagesDaily status-TSI, SOSvsSridharNo ratings yet
- Candidate Information Sheet - Final - Oct 2017Document2 pagesCandidate Information Sheet - Final - Oct 2017Yuva TechnologiesNo ratings yet
- Xyz Private Limited - NdaDocument3 pagesXyz Private Limited - NdaSvsSridharNo ratings yet
- ToDoOwnerReport 22 Nov 22Document60 pagesToDoOwnerReport 22 Nov 22SvsSridharNo ratings yet
- Online AssessmentDocument8 pagesOnline AssessmentSvsSridharNo ratings yet
- The Tamil Nadu Industrial Establishments (National and Festival Holidays) Rules Form ViDocument1 pageThe Tamil Nadu Industrial Establishments (National and Festival Holidays) Rules Form ViSvsSridharNo ratings yet
- Name Change Correction Form-1Document1 pageName Change Correction Form-1SvsSridharNo ratings yet
- ANF2ADocument6 pagesANF2Anehal28100% (2)
- Handbook On Spices and Condiments - Cultivation Processing and ExtractionDocument62 pagesHandbook On Spices and Condiments - Cultivation Processing and ExtractionSvsSridharNo ratings yet
- Manager HR JD PDFDocument1 pageManager HR JD PDFSvsSridharNo ratings yet
- The Tamil Nadu Industrial Establishments (National and Festival Holidays) Rules Form ViDocument1 pageThe Tamil Nadu Industrial Establishments (National and Festival Holidays) Rules Form ViSvsSridharNo ratings yet
- Adminstration Manual For Whom They Joined in New To The AreaDocument2 pagesAdminstration Manual For Whom They Joined in New To The AreaSvsSridharNo ratings yet
- Work Stream of DeptsDocument43 pagesWork Stream of DeptsAneesh KallumgalNo ratings yet
- Employees' Pension Scheme - 95 Calculator: Particulars Date MonthDocument2 pagesEmployees' Pension Scheme - 95 Calculator: Particulars Date MonthSachin JainNo ratings yet
- Payment of Gratuity Act & SuccessionDocument21 pagesPayment of Gratuity Act & SuccessionSvsSridharNo ratings yet
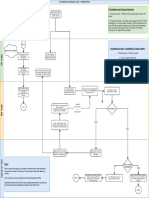
- Attendance Flow - FinalDocument1 pageAttendance Flow - FinalSvsSridharNo ratings yet
- ReadmeDocument12 pagesReadmeselo57No ratings yet
- Sample Transfer LetterDocument1 pageSample Transfer LetterSvsSridharNo ratings yet
- Biodata Format FinalDocument2 pagesBiodata Format Finalanon-90865197% (120)
- Form 15HDocument2 pagesForm 15Hgbiyer1234No ratings yet
- In Out Punch Import SamplesDocument3 pagesIn Out Punch Import SamplesSvsSridharNo ratings yet
- Lopr PDFDocument24 pagesLopr PDFdeepak kumarNo ratings yet
- Rating Sheet Name: SALINI.A Reg. No: 1913323036036Document1 pageRating Sheet Name: SALINI.A Reg. No: 1913323036036SvsSridharNo ratings yet
- Rigging & Slinging For Engineers - Purchasers PDFDocument2 pagesRigging & Slinging For Engineers - Purchasers PDFΈνκινουαν Κόγκ ΑδάμουNo ratings yet
- Motor Vehicles Act SummaryDocument111 pagesMotor Vehicles Act SummarySardaar Harpreet Singh HoraNo ratings yet
- Integrated BMSDocument14 pagesIntegrated BMSjim.walton100% (5)
- İngilizce A1 Seviye FiillerDocument70 pagesİngilizce A1 Seviye FiillerMehmet DursunNo ratings yet
- ISE215 Lecture4 Usingtheproduct Andre SjsuDocument25 pagesISE215 Lecture4 Usingtheproduct Andre SjsuHALASA TextilHogarNo ratings yet
- UoGx ECEg4155 Chapter 7 8Document45 pagesUoGx ECEg4155 Chapter 7 8Abdi ExplainsNo ratings yet
- Intro To Rhetorical FunctionDocument28 pagesIntro To Rhetorical FunctiondianNo ratings yet
- Tadimalla Bala ChaitanyaDocument4 pagesTadimalla Bala ChaitanyaTADIMALLA BALA CHAITANYANo ratings yet
- Maintenance and Service GuideDocument185 pagesMaintenance and Service GuidenstomarNo ratings yet
- Storyboard: Video Script and Storyboard On Evaluating Functions LessonDocument2 pagesStoryboard: Video Script and Storyboard On Evaluating Functions LessonIvanhoe BalaroteNo ratings yet
- Neap and Seameo Batch 2 InfoDocument28 pagesNeap and Seameo Batch 2 InfoAPPLE GOLANGAYANNo ratings yet
- Organic Agriculture Gr11 Q2.Module5 LRDocument17 pagesOrganic Agriculture Gr11 Q2.Module5 LRJam Hamil AblaoNo ratings yet
- Impact of Product Rebranding On Organization ProfitabilityDocument63 pagesImpact of Product Rebranding On Organization ProfitabilityDaniel ObasiNo ratings yet
- 동일고무 (TTV Fender 카탈로그)Document60 pages동일고무 (TTV Fender 카탈로그)조건현No ratings yet
- Atterberg's Limits Soil Classification - Liquid Limit, Plastic Limit, ShrinkageDocument5 pagesAtterberg's Limits Soil Classification - Liquid Limit, Plastic Limit, Shrinkagetombasingh100% (1)
- Activityideabank FinalDocument72 pagesActivityideabank FinalJoy Tu TranNo ratings yet
- AYUDA Multi-Words VerbsDocument6 pagesAYUDA Multi-Words VerbsGabriel RodriguezNo ratings yet
- Ambahan Poetry of The HanuooDocument4 pagesAmbahan Poetry of The HanuooJayrold Balageo MadarangNo ratings yet
- Anuraj JainDocument3 pagesAnuraj Jainanuraj1983No ratings yet
- Elon Musk AchievementsDocument13 pagesElon Musk AchievementsCarlos SuárezNo ratings yet
- What is Economics? - The study of production, distribution and consumption /TITLEDocument37 pagesWhat is Economics? - The study of production, distribution and consumption /TITLEparthNo ratings yet
- A CHAIN OF THUNDER: A Novel of The Siege of Vicksburg by Jeff ShaaraDocument13 pagesA CHAIN OF THUNDER: A Novel of The Siege of Vicksburg by Jeff ShaaraRandom House Publishing Group20% (5)
- Case Study - FGD PDFDocument9 pagesCase Study - FGD PDFLuthfanTogarNo ratings yet
- Grand Hotel PLCDocument2 pagesGrand Hotel PLCP.RAJAGURUNo ratings yet